Neck Pain Treatment in Sarasota, Florida
Neck pain is a condition that many people struggle with. Lavender Family Chiropractic is known for their focus on the neck. Our Sarasota Florida clinic can help you to feel better fast and deliver long term relief.
Neck Pain in Sarasota, FL: The Upper Cervical Approach That Resolves What Other Treatments Miss
By Dr. Rusty Lavender and Dr. Jacob Temple — Lavender Family Chiropractic, Sarasota, FL
Neck pain has a way of touching every corner of your day. The dull ache when you finally sit down at your desk. The sharp catch when you turn your head to back out of the driveway. The grinding tension that creeps up the side of your skull by mid-afternoon and steals your focus. The stiffness that wakes you up at three in the morning and won’t let you settle back into sleep.
If you’ve reached the point of searching for real answers — not another bottle of ibuprofen, not another round of stretches that worked for a week and stopped, not another massage that felt good for two hours — you’re in the right place. This guide will walk you through what neck pain actually is at a biological level, why so many treatments fail to resolve it long-term, and how a specific and gentle approach focused on the top of your spine can finally address the root cause.
At Lavender Family Chiropractic in Sarasota, Florida, we focus exclusively on the upper cervical spine — the atlas (C1) and axis (C2) — and the role these two small but critical bones play in chronic neck pain. We use 3D CBCT imaging, Tytron functional nervous system scans, and the Knee Chest Upper Cervical technique to find and correct the specific misalignment driving your symptoms. No twisting, no popping, no force.
This is the comprehensive guide. We’ll cover causes, anatomy, why the upper neck is different from the rest of your spine, what the latest research shows, what to expect at your first visit, and the most common questions we hear from patients. Let’s start with what neck pain actually is.
What Is Neck Pain, Really?
Neck pain, in medical terms, refers to discomfort anywhere from the base of your skull down to the top of your shoulders, including the seven vertebrae of the cervical spine, the muscles that support them, the discs between them, the nerves that pass through them, and the ligaments holding it all together.
It’s not a small problem. Neck pain affected more than 203 million people worldwide in 2020, and that number is projected to rise by roughly 33% by 2050. In high-income regions like North America, the burden is even higher than the global average. Women experience neck pain at meaningfully higher rates than men, and the highest prevalence occurs between ages 45 and 74 — right when most people are at the peak of their work and family responsibilities. (We’ll cite the research at length later.)
But statistics don’t capture the daily reality. Patients walk into our Sarasota office describing the same patterns again and again:
The desk-job ache that starts on the right side of the neck and travels up behind the ear by 2 p.m. The stiffness that won’t let you check a blind spot without rotating your whole upper body. The dull soreness at the base of the skull that turns into a tension headache if you ignore it long enough. The sharp pinch when you turn your head a certain way — sometimes the same way every time. The numbness or tingling that radiates down into the shoulder, arm, or hand. The bone-deep fatigue from constantly bracing against discomfort you can’t quite locate.
These aren’t separate problems. They’re variations of the same underlying issue showing up in different bodies — and in the majority of cases we see, the upper cervical spine is at the center of the story.
The Anatomy Most Doctors Skip Past
Your neck contains seven vertebrae, labeled C1 through C7 from top to bottom. The bottom five (C3 through C7) look more or less like the vertebrae below them — boxy bones with discs between them, held in place by muscle and ligament, designed to flex, extend, and rotate.
The top two are different. Radically different.
The atlas (C1) is a small ring-shaped bone that sits directly under your skull. It has no body. No disc above it. No disc below it. It cradles your roughly 10–12-pound head and is held in position primarily by ligaments and muscles — not by the bracing structures that stabilize the rest of your spine.
The axis (C2) sits beneath the atlas. It has a unique vertical bony projection called the odontoid process (or “dens”) that fits up through the ring of the atlas like a pivot. This atlanto-axial joint is responsible for roughly 60% of your head’s rotation. When you turn your head left to right, most of that motion is happening between C1 and C2, not lower in your neck.
This region — the occipito-atlanto-axial complex — is where the spinal cord meets the brainstem. It’s the bottleneck through which every nerve signal between your brain and your body has to pass. The vertebral arteries, which supply blood to the brainstem and the back of your brain, travel through small openings in these bones and follow a serpentine path that no other part of your spine demands.
It’s worth understanding what makes this design so unusual. Below C2, every vertebra has a disc above and below it that helps absorb load and maintain spacing. The atlas has neither. It floats between the skull above and the axis below, held in place entirely by ligaments — the transverse ligament that holds the dens (the upward projection of C2) in position, the alar ligaments that limit rotation, the apical ligament, and the tectorial membrane. This ligamentous stabilization gives the upper neck its remarkable mobility — your head can rotate, tilt, and nod with precision — but it also makes the region uniquely vulnerable to injury. A car accident, a sports impact, a hard fall, or even repetitive stress over years can stretch or strain these ligaments without producing the kind of damage that shows up on standard imaging.
The muscles in this region are equally specialized. The suboccipital muscles — the rectus capitis posterior major and minor, the obliquus capitis superior and inferior — are densely packed with proprioceptive fibers, far more than muscles anywhere else in the body. These tiny muscles are not just movers; they are sensors, constantly feeding information about head position to the brain. When they are tense, hyperactive, or sending distorted signals because of an underlying misalignment, the consequences are not just local soreness. They’re systemic — confusion in the brain’s spatial awareness, disruption of balance signals, and amplification of pain perception in the head, face, and upper body.
In other words: the top of your neck is not just “the upper part of your neck.” It’s the most neurologically and vascularly significant region in your entire spine — and the most vulnerable to subtle misalignment.
When the atlas or axis shifts even a fraction of a millimeter out of its ideal position, the consequences ripple outward. Muscles tighten to stabilize the misalignment. The lower neck compensates with altered movement patterns. The nerves passing through the area can become irritated. Blood flow can subtly change. And the brainstem — which regulates pain perception, muscle tone, autonomic function, and a hundred other essential processes — receives garbled information.
This is the layer that traditional medical evaluations rarely look at. Your MRI may read normal. Your X-ray may show “no significant findings.” Your bloodwork may be clean. And the pain persists, because the problem isn’t structural damage — it’s positional. It’s not a torn disc or a fractured vertebra. It’s the alignment of the bones themselves.
Why Your Upper Neck Drives So Much More Than Just Neck Pain
Patients are often surprised when we explain that the upper cervical spine is implicated not just in neck pain, but in migraines, vertigo, TMJ dysfunction, dizziness, and even autonomic symptoms like POTS. The reason is anatomical.
At the C2 level, the dorsal root ganglion — the cluster of nerve cell bodies that processes sensation from the upper neck and back of the head — shares overlapping pathways with the trigeminal nerve, which is the primary sensory nerve of the face. When the C2 region is irritated, the brain can interpret signals from this area as coming from the head, the face, or the jaw. This is the neurological basis for what’s called a “cervicogenic” headache — a headache that originates in the neck but is felt in the head.
The vestibular system, which controls your sense of balance and spatial orientation, receives major proprioceptive input from the small muscles of the upper neck — the suboccipital muscles, the rectus capitis muscles, and the obliquus capitis. When these muscles are tense, hyperactive, or providing distorted positional information, the result can be dizziness, vertigo, or a sense of imbalance even when the inner ear is functioning normally.
The vagus nerve and the autonomic pathways that regulate heart rate, blood pressure, digestion, and stress response all pass through or near the upper cervical region. Irritation in this zone can contribute to symptoms that seem to have nothing to do with the neck — racing heart, blood pressure swings, digestive issues, anxiety, brain fog.
This is why we so often see patients whose chief complaint is neck pain but whose other symptoms melt away once the upper cervical misalignment is corrected. The neck pain was the loudest signal. The other symptoms were the quieter signals from the same source.
Why Traditional Neck Pain Treatments So Often Fall Short
Most people with neck pain follow a predictable path. They try heat or ice. They try over-the-counter painkillers. They try a new pillow. They schedule a massage. If the pain persists, they see their primary care doctor, who may prescribe muscle relaxers or stronger NSAIDs and refer them to physical therapy. PT often helps temporarily — stretching, exercise, and strengthening the deep cervical flexors do address part of the problem — but the pain frequently returns.
Some patients end up at a chiropractor who delivers a high-velocity twisting adjustment to the entire neck. They feel relief for a few days, then the pain comes back, and they go in again. And again. And again. The “popping” never fully resolves the issue because the technique isn’t specific enough to correct the precise misalignment at the top of the neck.
Others escalate further: injections, nerve blocks, sometimes even fusion surgery.
Here’s the hard truth that most of these approaches miss. The latest research suggests that cervical facet joints — the small joints between the vertebrae — are the primary source of pain in roughly 25–67% of patients with chronic neck pain. The atlanto-axial joint specifically (C1-C2) accounts for 60% of all neck rotation, and dysfunction here creates compensation patterns up and down the cervical chain. If the top of the chain is misaligned and no one is checking it, no amount of massage, stretching, or general manipulation lower in the spine is going to fix the root cause.
That’s the missing layer in most neck pain care. And that’s the layer we focus on.
How Upper Cervical Chiropractic Care Works at Lavender Family Chiropractic
Our approach is built around three principles: measure precisely, correct gently, give the body time to heal.
The first visit is a consultation. We sit down with you, listen to the full history of your symptoms, ask the questions that don’t get asked in a 15-minute medical appointment, and determine whether you’re a candidate for upper cervical care. This consultation is complimentary. If we don’t think we can help you, we’ll tell you and point you toward a better fit.
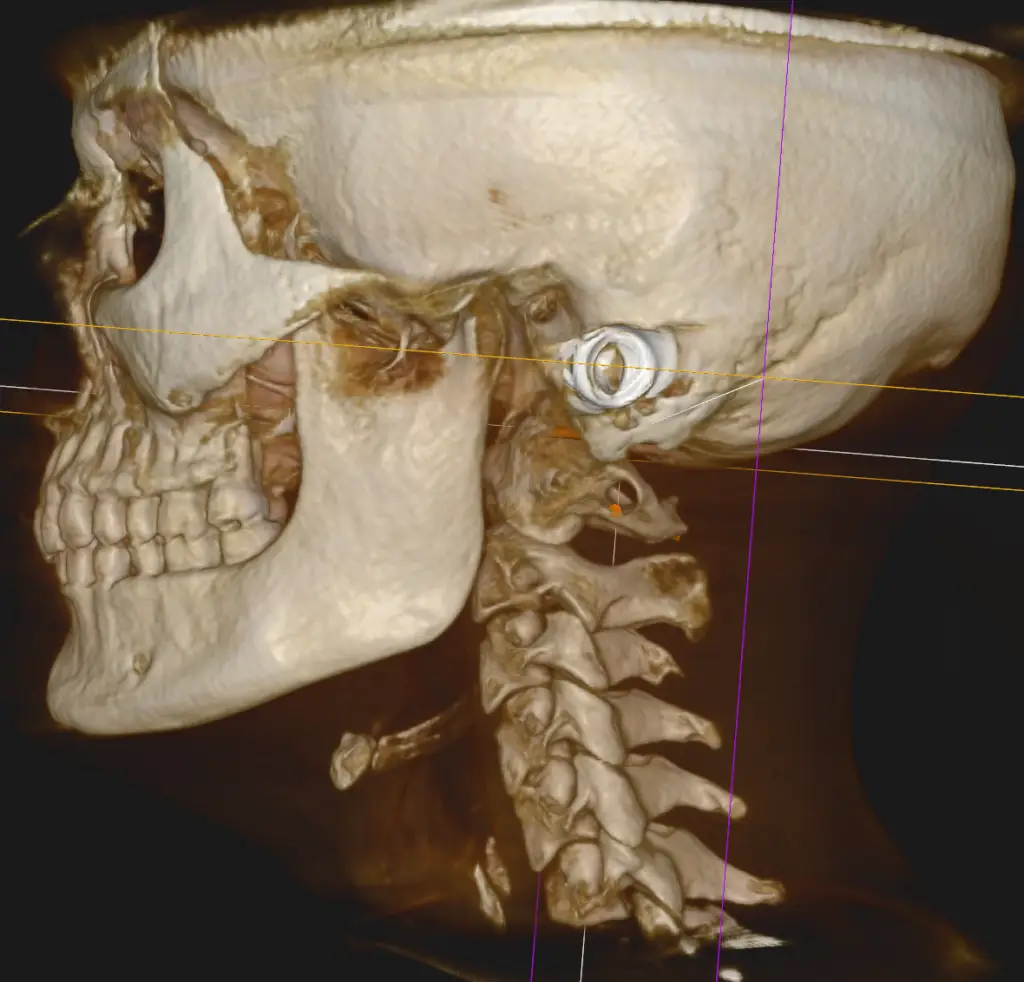
If you decide to move forward, we use 3D CBCT (cone beam computed tomography) imaging to measure your upper cervical spine in three dimensions. This is not a standard X-ray. CBCT produces a detailed three-dimensional view of the atlas, axis, and skull base, and allows us to measure the misalignment down to a hundredth of a millimeter. We pair this with Tytron paraspinal thermography, which provides a functional read of your nervous system by measuring temperature differences along the spine — a non-invasive way to see where the nerves are stressed.
From these measurements, we calculate the specific vector — the precise angle and force — needed to correct your unique misalignment. No two patients receive the same adjustment, because no two misalignments are identical.
The correction itself uses the Knee Chest Upper Cervical technique. You lie face-down on a specialized adjusting table. Our doctors deliver a low-force, highly specific impulse to the atlas. There’s no twisting. No popping. No cracking. Most patients are surprised by how gentle it is.
Then we let your body do what bodies are designed to do: heal. We don’t believe in adjusting people every visit just to keep them coming back. The goal is for your correction to hold — sometimes for weeks, sometimes for months — so that your nervous system can settle, your muscles can release the protective tension they’ve been holding, and your body can rebuild healthier patterns.
We do work from customized care plans tailored to your specific case. Some patients need a more intensive initial phase to retrain the spine and stabilize the correction; others stabilize more quickly. We’ll be transparent about what we recommend and why, and the plan will be built around what your imaging and exam findings actually show — not around a one-size-fits-all package.
→ Ready to find out if upper cervical care can help your neck pain? Call (941) 243-3729 to schedule your complimentary consultation, or book online at www.chiropractorsarasotaflorida.com. We’re located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — right at the corner of University and Whitfield.
What the Research Actually Says
We believe in evidence-based care, and we want you to make an informed decision. Here’s what the current peer-reviewed research shows about neck pain and the role of upper cervical care.
The Global Burden of Disease Study 2021, published in The Lancet Rheumatology in March 2024, analyzed neck pain across 204 countries and territories. The investigators found that neck pain affected 203 million people globally in 2020, with the highest age-standardized prevalence in older adults and meaningfully higher rates in women than men. The number of cases is projected to rise by 32.5% by 2050. This is one of the most comprehensive epidemiological analyses of neck pain ever published.
A 2024 randomized controlled trial published in Healthcare directly compared upper cervical spine manipulation to a combination of cervical, cervicothoracic junction, and thoracic spine manipulations in 186 patients with chronic non-specific neck pain. The researchers measured pain intensity, disability, and cervical range of motion. Both approaches produced improvements, but the upper cervical group showed meaningful short-term benefits in pain reduction and functional improvement — supporting the targeted upper cervical approach for patients who haven’t responded to broader manual therapy.
A landmark consensus paper from an international multispecialty working group, published in 2021, examined the role of cervical facet joints in chronic neck pain. The authors concluded that cervical facet joints are the primary source of pain in 25–67% of patients with chronic neck pain. The atlanto-axial joint (C1-C2) was identified as accounting for roughly 60% of cervical rotational movement and as a common — and frequently overlooked — source of upper neck pain, headache, and dysfunction.
A peer-reviewed paper on cervical ligamentous biomechanics published in PMC examined how the transverse, alar, and capsular ligaments stabilize the upper cervical spine. The authors detail how laxity or injury in these ligaments — particularly after whiplash or repetitive strain — can produce chronic neck pain, restricted range of motion, and referred symptoms into the head and shoulders. They specifically describe how the atlanto-axial complex’s unique reliance on ligamentous stability (rather than disc-based bracing) makes it especially vulnerable.
A cross-sectional study on forward head posture published in PMC examined the relationship between forward head position and cervical pain mechanosensitivity. Subjects with forward head posture demonstrated significantly lower pressure pain thresholds across multiple cervical structures and reduced cervical extension and rotation range of motion compared to controls — biomechanical evidence for why “tech neck” and prolonged screen use are driving the modern epidemic of chronic neck pain.
We could cite dozens more papers, but these five give you the foundation: neck pain is highly prevalent and rising; targeted upper cervical care produces measurable improvements; the upper cervical region is a major and frequently overlooked source of pain; the ligamentous structure of the area makes it uniquely vulnerable to misalignment; and modern lifestyle factors are making the problem worse.
Lifestyle Factors That Make Neck Pain Worse — and What Helps
Care in the office is only half of the equation. The other half is what you do the other 23 hours of the day. Here are the most important lifestyle factors we discuss with patients.
Screen position. The number-one driver of neck pain in patients under 50 is sustained forward head posture from looking down at phones, laptops, and tablets. For every inch your head moves forward from neutral, the effective load on your cervical spine increases substantially. Raise your screen. Put your phone at eye level. Use a laptop stand. Take micro-breaks every 30 minutes to reset.
Sleep position. Stomach sleeping is the worst position for the cervical spine — it forces sustained rotation for hours at a time. Side sleeping with a properly contoured pillow that fills the space between your ear and shoulder is generally best. Back sleeping works with a thinner pillow that supports the natural cervical curve.
Hydration and movement. Cervical discs and the small joints of the neck depend on movement and adequate hydration to exchange nutrients and maintain their structure. Long periods of immobility — whether driving, working, or watching TV — accelerate degeneration. Hydrate. Move every hour.
Stress and the jaw. Most people with chronic neck tension also clench their jaw, often without realizing it. The masseter, temporalis, and suboccipital muscles all overlap functionally. Working on stress regulation, jaw awareness, and breath patterns reduces compensatory neck tension.
Strength, not just stretching. Stretching tight neck muscles without strengthening the deep cervical flexors and the upper back almost always backfires. The neck needs both mobility and stability. Targeted exercises that strengthen the deep flexors and the scapular stabilizers are far more effective than stretching alone.
For a deeper dive into self-care strategies, see our companion guide: Natural Neck Pain Remedies.
Serving Sarasota and Surrounding Communities
Lavender Family Chiropractic is located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield, just minutes from downtown Sarasota, Lakewood Ranch, and Bradenton.
We’re proud to serve patients from across the region, including Sarasota, Bradenton, Lakewood Ranch, Venice, Palmer Ranch, Osprey, Siesta Key, Longboat Key, Lido Key, University Park, Parrish, Ellenton, Myakka City, Punta Gorda, and St. Petersburg. Many of our patients travel from across Florida — and even from out of state — because specific upper cervical care is rare and the results are worth the drive.
Top 15 Questions We Hear About Neck Pain
What’s the difference between upper cervical chiropractic and regular chiropractic? Regular chiropractic typically involves high-velocity adjustments to multiple areas of the spine, often with audible cracks and pops. Upper cervical chiropractic focuses exclusively on the atlas (C1) and axis (C2) and uses low-force, highly specific corrections based on detailed 3D imaging. There’s no twisting or popping. The goal is one precise correction that allows the rest of the spine to self-organize.
How long does it take to feel relief? Some patients feel a difference within a few days of their first correction. Others take several weeks as the nervous system settles and the body unwinds compensatory patterns. Chronic conditions that have been present for years usually take longer than recent issues.
Do you take insurance? We are out-of-network with insurance. We provide superbills so you can submit for reimbursement to your insurance company. We also offer flexible payment options to make care accessible.
Is the adjustment safe? Yes. The technique we use is one of the lowest-force forms of chiropractic adjustment in practice. There’s no twisting, no rapid rotation, and no “cracking.” The vector is calculated from your specific 3D imaging.
What conditions besides neck pain do you help with? Migraines, vertigo, POTS, TMJ dysfunction, post-concussion symptoms, whiplash recovery, fibromyalgia symptoms, ear pressure, tinnitus, and a range of conditions linked to upper cervical dysfunction.
Will I need to come in forever? No. The goal of care is to stabilize your correction so it holds for longer and longer periods. Many patients move into a maintenance phase where they come in only occasionally.
Why did my MRI say everything is normal but I still have pain? MRIs are excellent at showing structural damage — herniations, fractures, severe degeneration. They’re not designed to detect millimeter-level misalignments of the atlas. A normal MRI doesn’t rule out upper cervical involvement.
I’ve already tried physical therapy. Why would this be different? Physical therapy addresses muscle balance, mobility, and strength. Upper cervical care addresses positional misalignment at the top of the spine. They’re complementary, not redundant. Many patients benefit from both, but PT alone often misses the upper cervical layer.
Is it normal for my neck to crack on its own? Occasional spontaneous cracking is usually harmless. Chronic, repetitive self-cracking — especially the kind people do to relieve tension — often indicates underlying instability that isn’t being resolved by the cracking itself.
Can stress really cause neck pain? Stress doesn’t typically cause misalignment, but it powerfully worsens the symptoms of an existing misalignment by increasing muscle tone, sympathetic nervous system activity, and inflammation. Resolving the structural issue often makes neck pain much more resilient to stress.
What about pinched nerves and radiating pain into my arm? Radiating pain into the shoulder, arm, or hand can result from nerve root irritation lower in the cervical spine, but it’s often driven or amplified by upper cervical dysfunction that creates compensatory tension below. We evaluate the whole cervical chain.
How is whiplash different from regular neck pain? Whiplash involves rapid acceleration and deceleration that strains the ligaments stabilizing the upper cervical spine. It frequently produces upper cervical misalignment that doesn’t resolve on its own, even after the soft tissue heals.
I’m older — am I too old for this? No. We treat patients of all ages, from young children to people in their 90s. The adjustment is gentle enough to be appropriate across the age range.
How often do I need to come in? The initial phase of care typically involves more frequent visits to retrain the spine. As your correction stabilizes, visits become less frequent. Your specific care plan will be based on your imaging, your exam, and how your body responds.
How do I schedule a consultation? Call (941) 243-3729 or visit www.chiropractorsarasotaflorida.com to book online. Initial consultations are complimentary — we want to make sure we’re a good fit before you commit to anything.
You Don’t Have to Live With This
Neck pain has a way of becoming the background music of your life. You adapt to it. You work around it. You assume it’s just part of getting older, part of having a desk job, part of being human.
It doesn’t have to be.
If your neck pain isn’t responding to the things you’ve tried — if the medications, the stretches, the massages, the heating pads, even the chiropractic adjustments aren’t getting you where you want to be — there’s a good chance the upper cervical spine is the missing piece. And there’s a way to find out.
Call (941) 243-3729 or schedule online at www.chiropractorsarasotaflorida.com to book your complimentary consultation with Dr. Rusty Lavender or Dr. Jacob Temple. We’re at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243.
There is hope. There is a path forward. And it starts with a precise look at the part of your spine that most providers never check.
Related Articles
Natural Neck Pain Remedies and Upper Cervical Chiropractic Care
Can Neck Pain Cause Headaches? The Atlas Connection