Craniocervical Instability Treatment in Sarasota, Florida
Craniocervical instability (CCI) is a condition in which the ligaments and connective tissues that stabilize the junction between the skull and the upper cervical spine become weakened or damaged. This instability allows excessive or abnormal movement between the head and neck, which can irritate the brainstem, spinal cord, and upper cervical nerves. As a result, people with CCI may experience symptoms such as neck pain, headaches, dizziness, brain fog, visual disturbances, fatigue, and autonomic nervous system dysfunction. CCI is often associated with trauma, connective tissue disorders, or repetitive strain and can significantly affect neurological function and overall quality of life
Craniocervical Instability (CCI) in Sarasota, Florida: Understanding the Condition and the Role of Gentle Upper Cervical Care
By Dr. Rusty Lavender and Dr. Jacob Temple — Lavender Family Chiropractic, Sarasota, FL
Few conditions are as confusing, frightening, or misunderstood as craniocervical instability. Patients often arrive at our Sarasota office after months or years of searching — a stack of normal test results in one hand, a growing list of symptoms in the other, and the unsettling sense that something at the very top of their neck is not holding the way it should. They describe a head that feels too heavy for the neck to support, a “bobblehead” sensation, pain at the base of the skull that worsens the longer they sit upright, and a cascade of neurological symptoms that seem to have no single explanation.
If that describes you, we want to start with honesty rather than hype. Craniocervical instability is a serious condition, and in its true, structural form it is a medical and sometimes neurosurgical concern that deserves proper diagnosis. Gentle upper cervical care is not a cure for it — no honest provider should claim to physically repair damaged ligaments. What this guide will do instead is explain what craniocervical instability actually is at an anatomical level, how it is properly diagnosed, why it produces such a wide range of symptoms, and where careful, precise upper cervical chiropractic carecan have a supportive role as part of a larger picture.
At Lavender Family Chiropractic, we focus exclusively on the upper cervical spine: the atlas (C1), the axis (C2), and the junction where the skull meets the spine. We use 3D CBCT imaging, paraspinal infrared thermography, and the low-force Knee Chest Upper Cervical technique. Because we work in exactly the region where craniocervical instability lives, we are often one of the first stops for patients trying to understand what is happening to them — and part of our job is helping people figure out whether they need a chiropractor, a physician, a neurosurgeon, or some coordinated combination of the three. Let’s begin with the anatomy.
What Is Craniocervical Instability, Really?
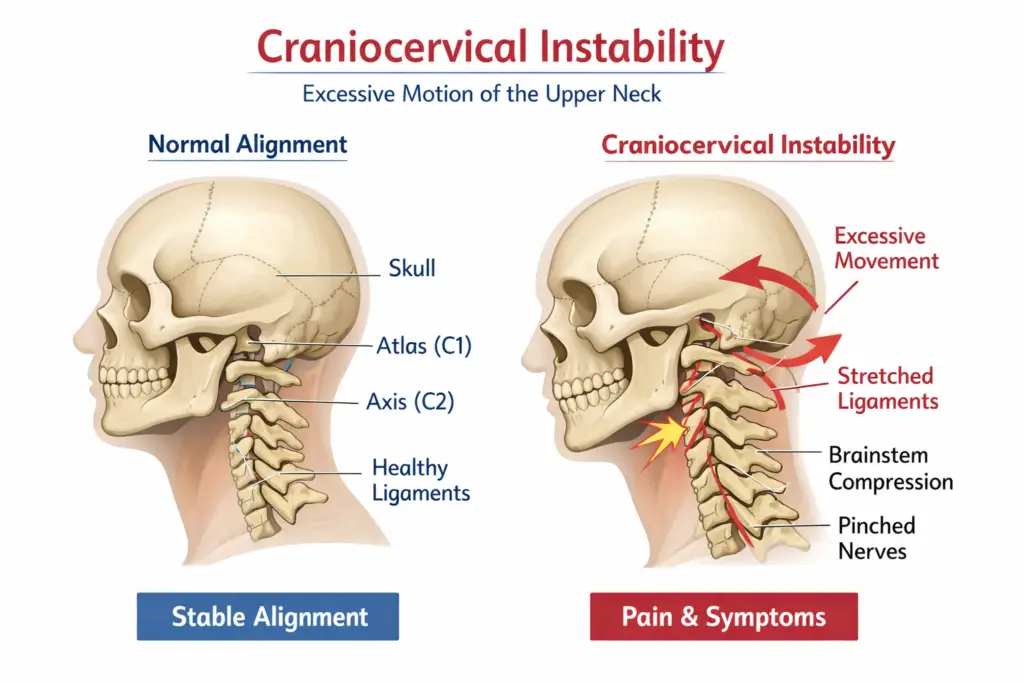
Craniocervical instability, or CCI, is a condition in which the ligaments and connective tissues that stabilize the junction between the skull and the upper cervical spine become weakened, stretched, or injured. When those stabilizing structures cannot do their job, the result is excessive or abnormal movement between the head and the top of the neck. That abnormal motion can irritate or place mechanical stress on the brainstem, the upper spinal cord, and the nerves and blood vessels that pass through this densely packed region.
It helps to be precise about language here, because the word “instability” gets used loosely. True craniocervical instability refers to a measurable, structural problem with the ligaments that hold the head to the neck — most importantly the alar ligaments, the transverse ligament, and the tectorial membrane. This is different from a simple upper cervical misalignment, in which the atlas or axis has shifted from its ideal position but the stabilizing ligaments are still fundamentally intact. The two can overlap, they can produce similar symptoms, and they can coexist — but they are not the same thing, and the distinction matters enormously when it comes to what kind of care is safe and appropriate.
CCI is most commonly associated with three things: significant trauma, such as a high-impact car accident, sports collision, or fall; hereditary disorders of connective tissue, most notably the Ehlers-Danlos syndromes and related hypermobility conditions; and, less commonly, complications following certain surgeries or in the setting of inflammatory or degenerative disease. In the hereditary connective tissue disorders, the underlying genetics affect the strength and integrity of collagen throughout the body, which means the ligaments of the craniocervical junction may be inherently more lax and prone to instability. A systematic review of craniocervical instability in Ehlers-Danlos syndrome describes exactly this relationship, along with the diagnostic and surgical criteria specialists use when instability becomes severe.
Because the symptoms of CCI are wide-ranging, fluctuating, and overlap with many other conditions, it is frequently misunderstood, missed, or over-diagnosed. Some patients spend years being told nothing is wrong. Others encounter the opposite problem and are told they have severe instability on the basis of a single measurement without adequate context. Both errors cause real harm. A careful, honest evaluation — one that neither dismisses your symptoms nor exaggerates the findings — is the foundation of good care.
The Anatomy of the Craniocervical Junction
To understand why craniocervical instability produces such dramatic symptoms, you have to understand just how unusual this small region of the body really is.
Your skull rests on the atlas (C1), a ring-shaped bone with no vertebral body and no disc above or below it. Beneath the atlas sits the axis (C2), which has a distinctive upward bony projection called the odontoid process, or dens. The dens rises up through the ring of the atlas and acts as a pivot, allowing your head to rotate. This design gives the upper neck extraordinary mobility — roughly half of your head’s rotation happens between C1 and C2 alone — but it comes at a cost. Unlike the rest of the spine, which is braced by discs and interlocking bony structures, the craniocervical junction relies overwhelmingly on ligaments for its stability.
Three ligamentous structures do most of the work. The transverse ligament stretches across the ring of the atlas and holds the dens firmly against the front of the atlas, preventing the atlas from sliding forward on the axis. The paired alar ligaments run from the top of the dens to the base of the skull and limit rotation and side-bending. The tectorial membrane, a continuation of a major spinal ligament, adds further restraint. An anatomic, functional, and radiographic review of the ligaments of the craniocervical junction details how these structures work together to allow motion while protecting the neural structures behind them.
The biomechanics are remarkably specific. As detailed in an update on the biomechanics of the craniocervical junction focused on the alar ligament, the alar ligaments are primary restraints against excessive rotation, and even partial injury to them can allow abnormal motion that the body then tries to compensate for through muscle guarding and altered movement patterns. This is why craniocervical instability is not just a matter of “loose ligaments” in the abstract — it changes how the entire head-neck system moves and loads.
What sits directly behind these ligaments is what makes the region so consequential: the brainstem and the upper spinal cord, the vertebral arteries that supply blood to the back of the brain, and the roots of nerves that influence everything from facial sensation to heart rate and digestion. When the stabilizing ligaments fail to control motion at this junction, the structures they were protecting can be affected. That is the anatomical heart of why CCI can feel like a whole-body illness rather than a neck problem.
Why Craniocervical Instability Causes So Many Different Symptoms
Patients with craniocervical instability often feel dismissed because their symptoms seem too varied to be “one thing.” But the diversity of symptoms makes complete sense once you understand the anatomy. When abnormal motion at the craniocervical junction places mechanical stress on the brainstem and upper cord, the effects ripple outward through every system those structures help regulate.
Common symptoms include a persistent headache at the base of the skull, often worse when upright and better when lying down; neck pain and the sensation that the head is unstable or too heavy; dizziness, unsteadiness, and balance problems; visual disturbances; brain fog and cognitive difficulty; fatigue that rest does not relieve; and a range of autonomic symptoms such as changes in heart rate, blood pressure swings, temperature dysregulation, and digestive problems. In more severe cases, patients may develop what specialists call cervical medullary syndrome — a constellation of neurological findings that arise from compression or deformation of the lower brainstem and upper cord.
The autonomic symptoms deserve special mention because they are so often overlooked. The lower brainstem contains the control centers for many automatic functions, and the vagus nerve — the body’s primary parasympathetic pathway — originates in this region. When the craniocervical junction is unstable, these pathways can be affected, which is part of why CCI overlaps so heavily with conditions like dysautonomia and POTS. We explore that overlap in our related discussion of vagus nerve dysfunction and upper cervical care.
There is an important honesty point embedded here. Because these symptoms are shared with dozens of other conditions — migraine, vestibular disorders, anxiety, chronic fatigue syndrome, and more — the presence of these symptoms does not by itself mean you have craniocervical instability. Many people with these exact complaints have upper cervical misalignment or other treatable problems rather than true structural instability. Sorting this out requires proper evaluation, not assumption.
How Craniocervical Instability Is Properly Diagnosed
This is the section we wish every patient would read before drawing conclusions from the internet. Craniocervical instability is a radiological and clinical diagnosis that belongs in the hands of physicians and specialists who work with this region.
Diagnosis generally combines a careful clinical history and neurological examination with specialized imaging. Standard X-rays and even conventional MRIs, taken lying down, often look normal in CCI because the instability may only reveal itself under load or in specific head positions. For that reason, specialists frequently rely on upright, flexion-extension, or rotational imaging, along with specific craniometric measurements. As described in the clinical literature on cervical medullary syndrome secondary to craniocervical instability in hereditary hypermobility connective tissue disorders, measurements such as the clivo-axial angle, the Grabb-Oakes measurement, and the basion-dens interval are used to quantify brainstem compression and vertical or horizontal instability. These are not measurements to be interpreted casually; the same source emphasizes how specific radiographic thresholds are correlated with neurological findings before major intervention is considered.
The point is this: a diagnosis of true craniocervical instability should be made by a qualified physician using appropriate imaging and clinical correlation — ideally a neurologist, neurosurgeon, or a specialist experienced with connective tissue disorders. If you suspect you have CCI, that medical workup is essential, and it is not something we or any chiropractor can replace. Where we can help is in evaluating the upper cervical spine for misalignment and mechanical stress, and in being an honest voice about when your findings point toward a need for medical or surgical referral.
Where Precise Upper Cervical Care Fits Into the CCI Picture
First, it is worth clearing up a common and important misconception. What we do is not high-velocity, twisting neck manipulation — the forceful “cracking” style of adjustment that people picture when they hear the word “chiropractor,” and that understandably raises concern in a sensitive neck. The Knee Chest Upper Cervical technique is the opposite of that. It is a precise, low-force correction with no twisting, no rotation, and no thrusting of the neck — a specific, gentle impulse calculated from your individual imaging. That precision and gentleness are exactly why it is well suited to this delicate region.
At the same time, we are honest about what the correction is and is not. It does not physically repair torn or lax ligaments, and it is not a substitute for the medical or neurosurgical evaluation that true structural instability deserves. And regardless of technique, any patient with signs of significant neurological compromise — progressive weakness, worsening coordination, swallowing or speech changes, or other red-flag findings — needs urgent medical attention.
With that context, here is where precise upper cervical care has a supportive role. Many patients who worry about craniocervical instability actually have upper cervical misalignment — the atlas or axis sitting out of its ideal position — which can create mechanical stress on the same region and produce similar symptoms. Others have a degree of instability alongside a correctable misalignment. In these situations, restoring better alignment of the atlas and axis can reduce abnormal mechanical stress on the junction, help the supporting musculature stop guarding, and allow the nervous system to function with less interference. The aim is a more stable, better-organized upper neck.
We still begin with a careful evaluation, and we work in coordination with your physicians when your situation calls for it. If we believe you would be better served by medical management, we will tell you plainly and help point you in the right direction.
Our Approach at Lavender Family Chiropractic
Our approach to the upper cervical spine is built on three commitments: measure precisely, proceed gently, and stay honest about what care can and cannot do.
Every relationship begins with a thorough consultation. We take the time to hear your full history — your symptoms, any trauma, any diagnosis of a connective tissue disorder, prior imaging, and what other providers have told you. This conversation is where we begin to sort out whether your picture looks more like a correctable upper cervical misalignment, more like true structural instability that needs medical oversight, or some combination that calls for co-management. This consultation is complimentary, and if we do not believe upper cervical care is right for you, we will say so.
When it is appropriate to proceed, we use 3D CBCT imaging to measure the upper cervical spine in three dimensions, allowing us to see the alignment of the atlas, axis, and skull base in fine detail. We pair this with paraspinal infrared thermography, a radiation-free scan that gives a functional read of how your nervous system is behaving along the spine. From these findings, we calculate a correction specific to you.
The correction itself uses the low-force Knee Chest Upper Cervical technique — no twisting, no popping. We then give your body time to hold the correction and adapt, rather than adjusting reflexively at every visit. We work from customized care plans built around your individual findings and goals, and we are transparent about expectations, including the reality that responses vary and that some patients, particularly those with significant structural instability, are better served primarily by their medical team. Where appropriate, we are glad to work alongside your physicians rather than in place of them.
→ If you are trying to make sense of upper cervical symptoms and want a careful, honest evaluation, call Lavender Family Chiropractic at (941) 243-3729 or schedule a complimentary consultation online. We are located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — right at the corner of University and Whitfield.
What the Research Says
We believe you deserve to see the evidence and understand its context. Here is what the peer-reviewed literature shows about the craniocervical junction and instability.
A systematic review of craniocervical instability in Ehlers-Danlos syndrome examined how instability arises in hereditary connective tissue disorders and outlined the diagnostic and surgical treatment criteria specialists use. The review underscores that in these patients the underlying cause is ligamentous laxity from a genetic collagen disorder, and that surgical intervention is reserved for well-defined, severe cases meeting specific clinical and radiographic thresholds — a reminder of how serious true structural CCI can be.
An anatomic, functional, and radiographic review of the ligaments of the craniocervical junction details how the transverse ligament, alar ligaments, and tectorial membrane stabilize the junction, and how imaging is used to assess them. This work grounds the entire concept of instability in specific, identifiable structures rather than vague notions of a “loose neck.”
An update on the biomechanics of the craniocervical junction focused on the alar ligament explains how the alar ligaments restrain rotation and side-bending, and how injury to them alters motion at the junction. It illustrates why even partial ligament compromise can create outsized effects on movement and stability.
A comprehensive review of the craniocervical junction’s embryology, anatomy, biomechanics, and imaging in blunt trauma describes how traumatic forces — the kind involved in car accidents and falls — can injure the stabilizing ligaments of this region and how imaging is used to evaluate the damage. This is directly relevant to the many patients whose symptoms began after a significant impact.
Finally, a clinical study on cervical medullary syndrome secondary to craniocervical instability in hereditary hypermobility connective tissue disorders describes the craniometric measurements used to diagnose severe instability with brainstem compression, and the outcomes of surgical stabilization in carefully selected patients. It is a sobering, clarifying look at what the most severe end of the CCI spectrum involves — and why proper diagnosis matters so much.
Taken together, the research paints a consistent picture: the craniocervical junction is a ligament-dependent, neurologically critical region; true instability is a definable structural problem that ranges from mild to severe; trauma and connective tissue disorders are the major drivers; and severe cases are medical and surgical matters. None of this literature suggests that any conservative provider can reverse structural instability — and we would be misleading you to claim otherwise. What careful upper cervical care offers is attention to alignment and mechanical stress in this region, as one part of a well-coordinated approach.
Lifestyle and Self-Care Considerations
If you are living with upper cervical symptoms or a diagnosis of instability, day-to-day habits matter, and some common advice can actually make things worse. Please treat the following as general education and coordinate specifics with your own care team, because the right approach depends heavily on your individual diagnosis.
Protect the neck from provocative positions. Sustained forward-head posture from phones and screens increases load on the upper neck. Raising screens to eye level and taking frequent movement breaks reduces that strain.
Be thoughtful about sleep support. A pillow that keeps the head and neck in a neutral position, rather than propped too high or dropped too low, helps limit overnight stress on the junction. Many patients find side-sleeping with proper head support more comfortable than stomach sleeping, which forces sustained rotation.
Avoid aggressive self-manipulation. The habit of forcefully cracking or twisting your own neck to chase relief can worsen instability over time. If your neck constantly feels like it “needs” to crack, that is worth discussing rather than acting on repeatedly.
Move gently and build stability, carefully. For appropriate patients, gentle, professionally guided strengthening of the deep neck and postural muscles can support the region. But with instability, generic neck exercises and end-range stretching can be counterproductive, so this should always be individualized under qualified guidance.
Mind the whole system. Because CCI overlaps with autonomic and vestibular symptoms, attention to hydration, stress regulation, and paced activity often helps day-to-day function. For readers whose main experience is dizziness and imbalance, our related guide on craniocervical instability, vertigo, neck pain, and migraines walks through how these threads connect.
Serving Sarasota and Surrounding Communities
Lavender Family Chiropractic is located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield, just minutes from downtown Sarasota, Lakewood Ranch, and Bradenton.
We are proud to serve patients from across the region, including Sarasota, Bradenton, Lakewood Ranch, Venice, Palmer Ranch, Osprey, Siesta Key, Longboat Key, Lido Key, University Park, Parrish, Ellenton, Myakka City, Punta Gorda, and St. Petersburg. Because specific, gentle upper cervical care is uncommon, many patients travel a considerable distance to be evaluated — and because craniocervical concerns can be complex, we are always glad to communicate with your existing physicians so your care stays coordinated.
Top 15 Questions We Hear About Craniocervical Instability
What is the difference between craniocervical instability and an upper cervical misalignment? Instability refers to a structural problem with the ligaments that stabilize the head-neck junction, allowing abnormal motion. A misalignment means the atlas or axis is out of its ideal position while the ligaments remain fundamentally intact. They can look similar and can coexist, but they are not the same, and telling them apart is central to safe care.
Can upper cervical chiropractic cure craniocervical instability? No. Care cannot repair torn or lax ligaments, and no honest provider should claim to cure instability. Gentle care may support better alignment and reduce mechanical stress in the region for appropriate patients, as part of a broader plan.
How is CCI diagnosed? Through a combination of clinical examination and specialized imaging, often upright or flexion-extension MRI, interpreted by physicians using specific craniometric measurements. This medical workup is essential and cannot be replaced by a chiropractic exam.
Isn’t getting your neck adjusted risky with instability? It is important to separate two very different things. The forceful, high-velocity, twisting manipulation that most people picture is not what we do. Our Knee Chest Upper Cervical technique is a precise, low-force correction with no twisting or thrusting, which is exactly why it is gentle enough for this delicate region. We evaluate carefully first and coordinate with your medical team when appropriate.
What causes craniocervical instability? The main drivers are significant trauma (such as car accidents, falls, or sports impacts), hereditary connective tissue disorders like the Ehlers-Danlos syndromes, and less commonly certain post-surgical or disease-related situations.
Why do I have so many symptoms that seem unrelated? Because the craniocervical junction sits at the brainstem, where pathways controlling balance, autonomic function, and sensation converge. Mechanical stress here can affect many systems at once, which is why CCI can feel like a whole-body illness.
My MRI was normal — does that rule out CCI? Not necessarily. Standard MRIs taken lying down can miss instability that only appears under load or in certain positions. This is why specialists sometimes use upright or dynamic imaging. It also means a normal lying-down MRI does not confirm CCI either — proper evaluation is needed in both directions.
Do I need surgery? Only a minority of patients with severe, well-documented structural instability and neurological compromise are considered for surgical stabilization, and that decision belongs to a neurosurgical specialist. Most people exploring these symptoms are not in that category, which is another reason accurate diagnosis matters.
I have Ehlers-Danlos syndrome — should I be concerned about my neck? Connective tissue disorders can increase the risk of craniocervical instability, so upper cervical symptoms deserve careful medical evaluation. If you have EDS and neck or neurological symptoms, coordinating with physicians familiar with the condition is important.
Can a car accident cause CCI? Trauma can injure the stabilizing ligaments of the craniocervical junction. Many patients date their symptoms to a specific impact. Post-traumatic upper cervical problems are worth evaluating, and we discuss related injuries in our material on whiplash and upper cervical care.
Will I need to come in forever? No. For appropriate patients, the goal is to help the correction hold for longer periods so visits become less frequent over time. Your plan is based on your findings and how your body responds.
Do you take insurance? We are a cash-pay, out-of-network office and do not bill insurance directly. We provide superbills that you may submit to your insurance company for possible out-of-network reimbursement, depending on your individual plan. This lets us focus fully on your care.
How is your care structured? After your evaluation, we build a customized care plan around your specific findings and goals, and we explain our recommendations up front so you always know what to expect.
When should I go to the emergency room instead? Seek urgent medical care for progressive weakness, worsening balance or coordination, difficulty swallowing or speaking, fainting, severe new headaches, or any rapidly changing neurological symptoms. These can signal serious compression and are medical emergencies.
How do I get started? Call (941) 243-3729 or visit our website to book a complimentary consultation. We will listen to your history, evaluate whether gentle upper cervical care is appropriate for you, and be honest about whether you would be better served by medical referral or coordinated care.
You Deserve Answers and an Honest Plan
Craniocervical instability can be an isolating diagnosis. The symptoms are real, the fear is understandable, and the path to good care is rarely straightforward. What we want you to take from this guide is that clarity is possible. There is a real anatomy behind your symptoms, there is a proper way to diagnose what is actually going on, and there is a difference between conditions that need gentle conservative support and those that need medical or surgical management.
Our commitment to you is honesty first. We will help you understand your upper cervical spine, we will offer gentle care when it is appropriate, and we will tell you plainly when your situation calls for a physician or specialist instead of — or alongside — what we do.
Call (941) 243-3729 or schedule online to book a complimentary consultation with Dr. Rusty Lavender or Dr. Jacob Temple. We are located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, at the corner of University and Whitfield. Let’s find out what is really going on — and build a plan that treats your situation with the seriousness and honesty it deserves.
Related Articles