By Dr. Rusty Lavender — Lavender Family Chiropractic, Sarasota, FL
Craniocervical and Atlantoaxial Instability: Few regions of the human body are as intricate, as heavily trafficked by delicate structures, or as easy to misunderstand as the junction where the skull meets the top of the spine. When patients come to our Sarasota office describing a head that feels “too heavy” for the neck, a sense that the skull might shift when they turn, or a cascade of neurological symptoms that seem to defy easy explanation, two terms often surface in their research: craniocervical instability (CCI) and atlantoaxial instability (AAI). These two conditions are frequently mentioned in the same breath, and for good reason — they are neighbors, they share overlapping ligaments, and they can produce a strikingly similar collection of symptoms. Yet they are not the same thing, and understanding the difference matters a great deal for anyone trying to make sense of upper neck symptoms.
At Lavender Family Chiropractic, we believe that clear, honest education is one of the most valuable things we can offer. Both craniocervical instability and atlantoaxial instability, in their true structural forms, are serious medical concerns that require accurate diagnosis and, in many cases, coordinated care with medical and surgical specialists. We want to be direct from the outset: precise, low-force upper cervical chiropractic care does not repair torn or lax ligaments, and it is not a substitute for a proper medical workup. What we can do — carefully, gently, and only for appropriate patients — is assess how the top bones of your neck are aligned relative to your head, measure patterns of nervous system stress, and provide precise, low-force correction that supports the way your upper cervical spine functions day to day.
This article is written to help you understand what separates these two conditions, where they overlap, who is most at risk, and how thoughtful upper cervical care fits into the bigger picture. Along the way, we will point you toward research, describe what our approach can and cannot do, and explain when a symptom warrants urgent medical attention rather than a chiropractic visit. If you live in Sarasota, Bradenton, Lakewood Ranch, Venice, or any of the surrounding communities and you have been wrestling with confusing upper neck symptoms, we hope this gives you a clearer map.
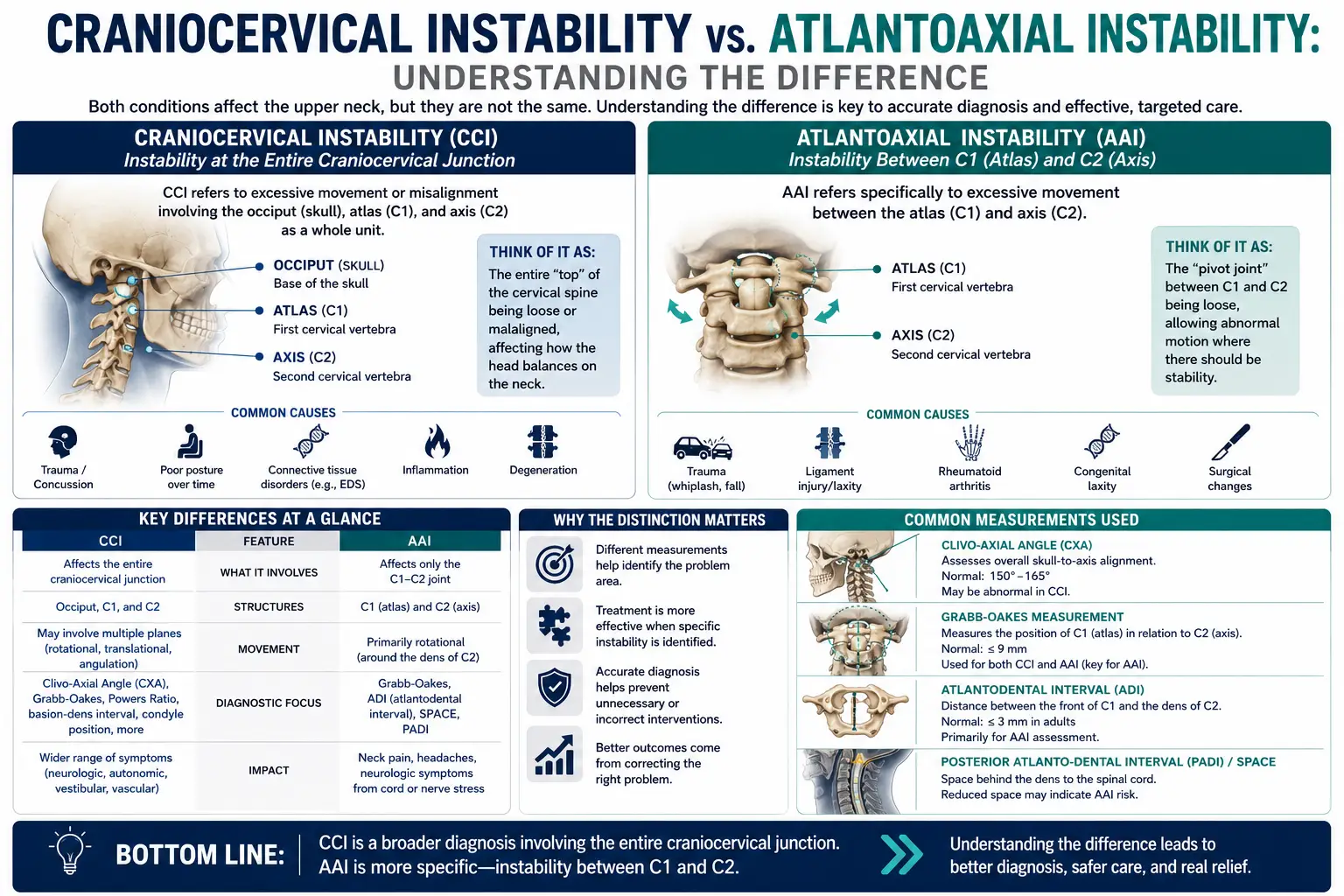
Defining the Two: Craniocervical Instability (C0-C1-C2 / skull-to-neck) vs. Atlantoaxial Instability (specifically C1-C2)
The simplest way to keep these two conditions straight is to remember which joints each one describes.
Craniocervical instability (CCI) refers to excessive or abnormal movement across the craniocervical junction — the transition zone that connects your skull (the occiput, often labeled C0) to the first cervical vertebra (the atlas, C1) and the second cervical vertebra (the axis, C2). In other words, CCI is a broad term describing instability of the whole skull-to-upper-neck complex. It involves the occiput-C1 joint (also called the atlanto-occipital joint) and often the C1-C2 relationship as well. When clinicians talk about CCI, they are usually concerned with how the head sits and moves on top of the spinal column, and whether that motion has become excessive enough to stress or compress the brainstem, upper spinal cord, blood vessels, or nerves that pass through this crowded corridor.
Atlantoaxial instability (AAI) is more specific. It describes excessive movement specifically at the atlantoaxial joint — the articulation between C1 (the atlas) and C2 (the axis). This is the joint responsible for a large share of your neck’s rotational movement; roughly half of your ability to turn your head left and right happens right here at C1-C2. AAI is fundamentally about the relationship between the atlas and the axis, and in particular about a small but critically important peg of bone called the dens, or odontoid process, which rises up from C2 and acts as a pivot for C1 to rotate around.
Here is the relationship in plain terms: the craniocervical junction is the larger neighborhood, and the atlantoaxial joint is one house within it. Because AAI involves C1-C2, and because the craniocervical junction also involves C1-C2, the two conditions overlap. A person can have craniocervical instability, atlantoaxial instability, both, or a variant of one that primarily affects a single joint. Some patients have instability that is mostly at the skull-to-C1 level; others have it concentrated at C1-C2; and some have a combined picture. This overlap is exactly why the two terms get confused and why careful, individualized assessment matters so much. You can learn more about the broader condition on our dedicated craniocervical instability resource page, which serves as a companion to this article.
It is also worth stating plainly that “instability” is a spectrum and a clinical judgment, not a single yes-or-no switch. Mild ligament laxity that produces occasional symptoms is very different from frank structural instability with measurable subluxation and neurological compromise. The latter is a neurosurgical concern. That distinction runs throughout everything that follows.
The Anatomy Behind Each
To appreciate the difference between CCI and AAI, it helps to walk through the anatomy of this remarkable region.
The craniocervical junction and its ligaments
The craniocervical junction is held together not primarily by large muscles or interlocking bones, but by an elegant system of ligaments. Unlike the lower spine, where the vertebrae have generous bony contact and thick discs, the upper cervical spine sacrifices bony stability in exchange for mobility. That trade-off is what lets you nod, tilt, and rotate your head through such a wide range of motion — but it also means the ligaments are doing a great deal of the work.
Several ligaments are central to craniocervical stability. The alar ligaments are two strong bands that run from the sides of the dens up to the occiput (and to the atlas), and they act as important checks on rotation and side-bending of the head. The transverse ligament (part of the larger cruciate ligament) stretches horizontally across the ring of the atlas, holding the dens snugly against the front arch of C1 and preventing the atlas from sliding forward on the axis. The tectorial membrane, apical ligament, and the capsular ligaments of the joints add further support, and together this network functions as a suspension system for the head. A published anatomic and radiographic review of the craniocervical junction ligaments describes how these structures work in concert to permit motion while restraining excessive translation and rotation — a balance that, when disrupted, sets the stage for instability.
In CCI, the concern is that this ligamentous suspension system has become lax, stretched, injured, or congenitally weak, allowing the occiput and upper cervical vertebrae to move more than they should relative to one another. Because the brainstem and the very top of the spinal cord sit right at this junction, abnormal motion here can, in significant cases, produce neurological symptoms.
The dens, the transverse ligament, and the C1-C2 joint
Atlantoaxial instability zooms in on a single, elegant mechanical arrangement. Picture the atlas (C1) as a ring, and the dens (odontoid process) of the axis (C2) as a vertical peg rising up into the front portion of that ring. The atlas rotates around the dens like a wheel turning on an axle. What keeps the atlas from sliding forward off that axle is chiefly the transverse ligament, which pins the dens against the anterior arch of C1. The alar ligaments provide secondary restraint, particularly limiting excessive rotation.
AAI develops when this specific arrangement fails or loosens. There are a few broad ways this can happen. The transverse ligament can become incompetent — through injury, inflammatory erosion, or congenital laxity — allowing the atlas to shift forward relative to the axis (anterior atlantoaxial subluxation). The dens itself can be abnormal: some people are born with an unfused or separate ossicle called os odontoideum, or with a hypoplastic (underdeveloped) dens, which removes the very peg the transverse ligament relies on. Rotational instability can also occur when the C1-C2 relationship becomes abnormal in the rotational plane. In each case, the underlying problem is that C1 and C2 are no longer held in their correct, stable relationship, and the spinal cord passing through that ring can be at risk when the space available for it narrows.
Overlap and differences
The alar and transverse ligaments belong to both stories, which is precisely why CCI and AAI overlap. A dedicated biomechanical review of the alar ligament highlights its role as a key restraint of the craniocervical junction, limiting rotation and contralateral side-bending — functions that are relevant to both skull-on-atlas and atlas-on-axis stability. The key distinction is the level of primary concern. CCI is oriented around the occiput-C1 (and the whole junction) and how the head sits on the spine; AAI is oriented around C1-C2 and the dens. In everyday clinical language, if the main problem is the head shifting on the neck, that points toward the craniocervical picture; if the main problem is the atlas shifting on the axis around the dens, that points toward the atlantoaxial picture. Real patients, of course, do not always sort themselves neatly into one box, which is why imaging and specialist evaluation are so important when true structural instability is suspected.
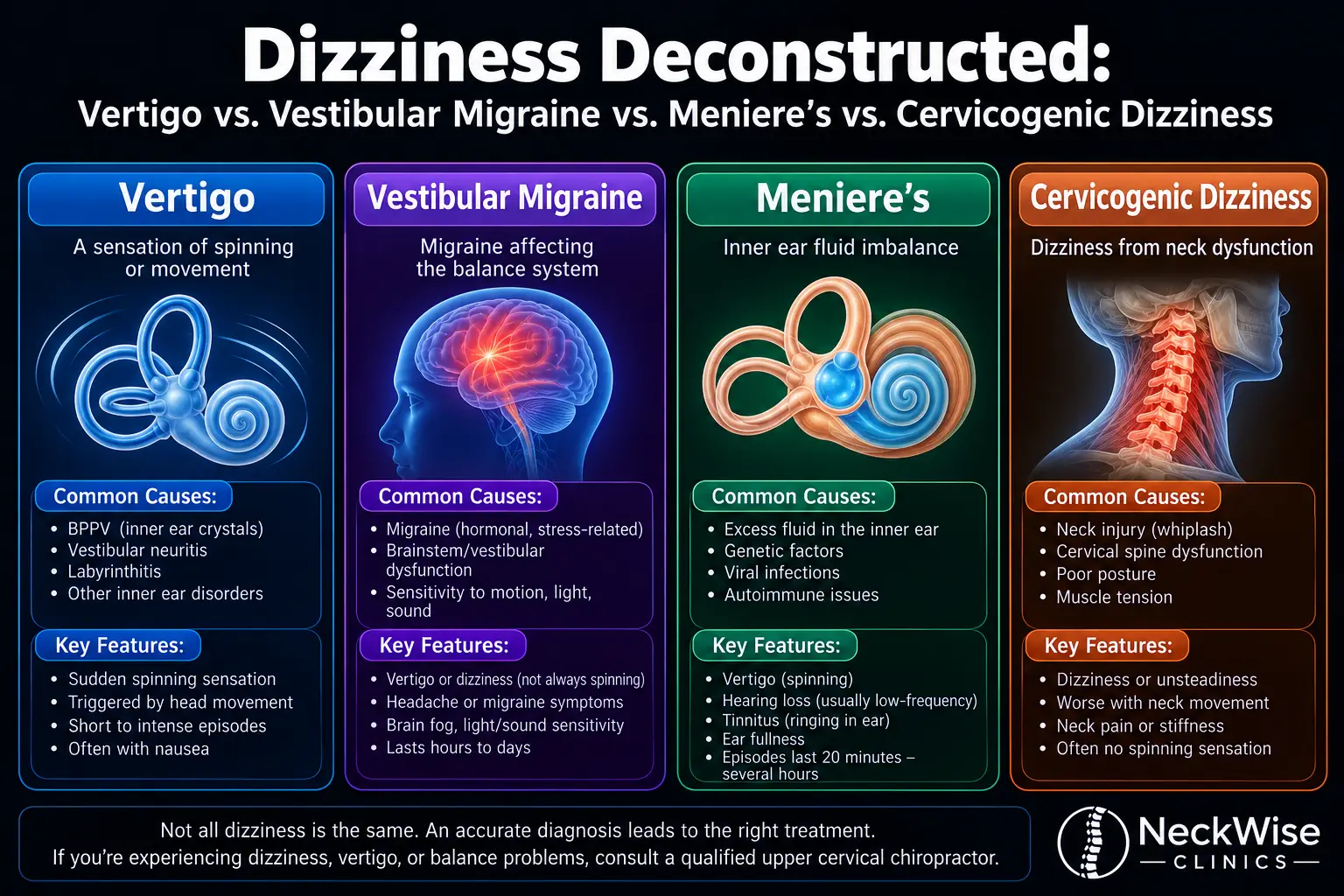
Symptoms, Overlap, and How They Differ
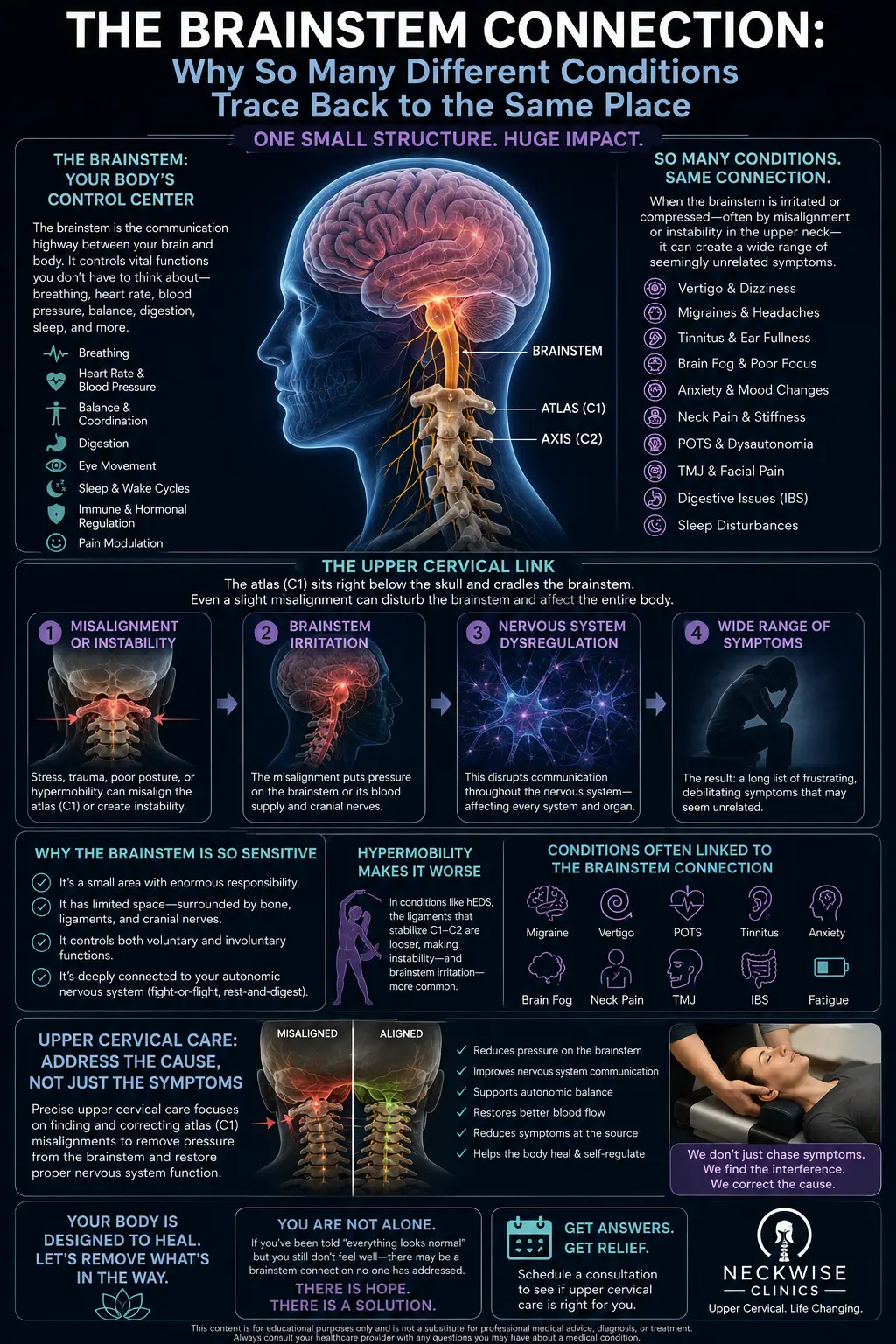
One of the most challenging aspects of both conditions is that their symptoms can be diffuse, variable, and easy to attribute to something else. Because the craniocervical junction houses the brainstem, the upper spinal cord, cranial nerves, and important blood vessels, dysfunction in this area can generate a wide and sometimes bewildering symptom list.
Commonly reported symptoms that overlap across both CCI and AAI include:
- A sensation that the head is heavy or that the neck cannot comfortably support it (some patients describe needing to hold their head up with their hands, sometimes called the “bobblehead” feeling)
- Suboccipital headaches, often at the base of the skull
- Neck pain and stiffness, particularly high in the neck
- Dizziness, lightheadedness, or a sense of imbalance
- Visual disturbances or difficulty with focus and concentration (“brain fog”)
- Ringing in the ears or a feeling of pressure in the head
- Nausea
- Symptoms that worsen with upright posture or certain neck positions and ease when lying down
If you find that your head feels persistently too heavy for your neck, we discuss that specific experience in more depth on our page about craniocervical instability and the “head feels too heavy” sensation.
How do the two differ symptomatically? The differences are matters of emphasis rather than hard lines. AAI, because it centers on the rotational C1-C2 joint, may be more strongly associated with symptoms provoked by head rotation — turning to look over the shoulder, for instance — and with rotational neck stiffness. In more advanced atlantoaxial instability, especially when the dens or a subluxation encroaches on the spinal cord, patients may develop myelopathic signs: changes in the arms or legs, altered coordination, weakness, numbness or tingling in the limbs, changes in fine motor control, gait disturbance, or in serious cases problems with bladder or bowel function. CCI, involving the occiput and the whole junction, is often described in the context of head-on-neck instability and brainstem-related symptoms, which can include a similarly broad neurological picture.
Here is the honest and important point: these overlapping symptoms are also produced by many other, far more common conditions — ordinary muscular neck strain, migraine, benign positional vertigo, anxiety, and more. The presence of these symptoms does not mean you have structural instability. At the same time, certain symptoms should never be brushed off. Progressive weakness, worsening numbness or tingling in the limbs, loss of coordination, difficulty walking, swallowing or speech changes, fainting, or changes in bladder or bowel control are red flags. These warrant prompt medical evaluation — often urgent or emergency care — not a wait-and-see approach and not a chiropractic adjustment. We will return to this point, because it is central to caring for people honestly.
Populations at Risk
Neither CCI nor AAI strikes at random. Certain groups carry a meaningfully higher risk, and knowing whether you belong to one of them changes how aggressively instability should be screened for and how cautious any hands-on care needs to be.
Down syndrome (Trisomy 21). Atlantoaxial instability is especially important in individuals with Down syndrome, where ligamentous laxity and skeletal differences at C1-C2 are more common. This is one of the best-recognized associations in all of spine care. Because of this elevated risk, radiological screening and careful clinical vigilance have long been part of the conversation for children and adults with Down syndrome, particularly before activities that load the neck. A recent systematic review focused specifically on radiological screening of atlantoaxial instability in children with Trisomy 21 examined how best to identify those at risk and offered evidence-based screening recommendations — a reflection of just how central AAI is in this population. For anyone with Down syndrome, upper neck symptoms deserve especially careful medical attention.
Rheumatoid arthritis and other inflammatory arthropathies. Rheumatoid arthritis (RA) is a systemic inflammatory disease that can erode the ligaments and bone of the upper cervical spine over time. The transverse ligament and the tissues around the dens can be weakened by chronic inflammation, and the cervical spine — particularly the atlantoaxial region — is a well-documented site of RA involvement. Atlantoaxial subluxation is a recognized complication of longstanding RA. Related inflammatory conditions, such as psoriatic arthritis and ankylosing spondylitis, can also affect this region. Anyone with a long history of inflammatory arthritis who develops new neck pain or neurological symptoms should be evaluated with this possibility in mind.
Ehlers-Danlos syndrome and connective tissue disorders. Heritable connective tissue disorders, most notably the Ehlers-Danlos syndromes (EDS), are characterized by unusually lax and fragile collagen — the very material that makes up ligaments. Because craniocervical and atlantoaxial stability depend so heavily on ligamentous integrity, people with EDS and related hypermobility disorders are recognized as being at higher risk for craniocervical and atlantoaxial instability. A systematic review of craniocervical instability in Ehlers-Danlos syndrome examined diagnostic and surgical treatment criteria in this group, underscoring both the reality of the association and the genuine diagnostic complexity involved. If you have EDS or a hypermobility spectrum disorder, this is worth discussing candidly with your care team.
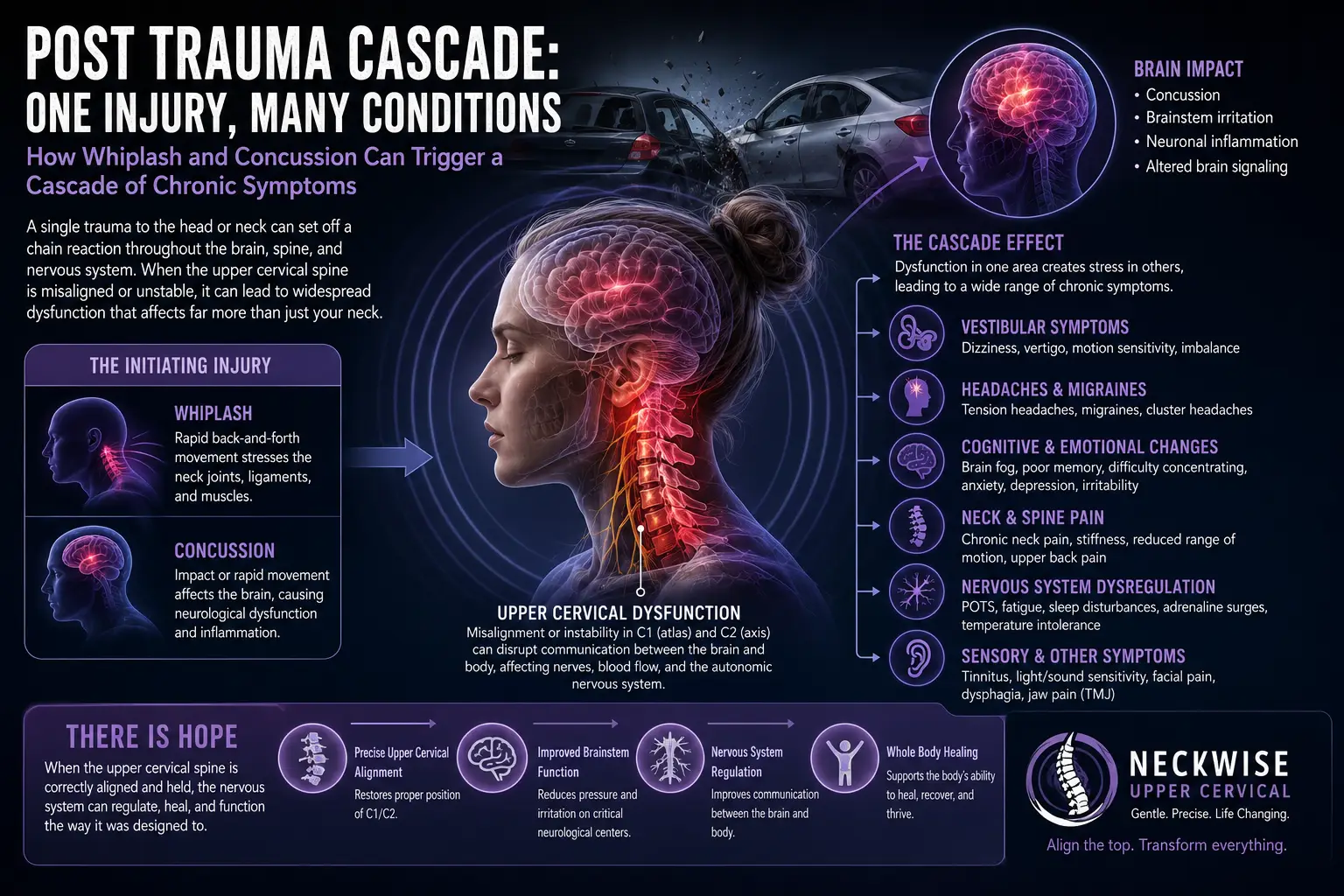
Trauma. Finally, acute trauma — motor vehicle collisions, falls, sports impacts, and similar high-energy events — can injure the ligaments of the craniocervical junction and the atlantoaxial joint directly. Traumatic instability is a medical emergency in the acute setting and must be evaluated with appropriate imaging. Even well after an injury has healed, some people are left with residual laxity or altered mechanics that continue to generate symptoms.
Recognizing that you fall into one of these categories does not mean you have instability — many people in these groups never develop it. But it does mean that upper neck symptoms should be taken seriously and evaluated thoughtfully, and it means that any hands-on care must be selected and delivered with extra care.
Where the Upper Neck and Precise Upper Cervical Care Fit
Given everything above, a fair question is: where does chiropractic care belong in this picture at all? It is a question we take seriously, and our answer begins with honesty about boundaries.
Let us be clear about what precise upper cervical care cannot do. It does not repair, tighten, or regenerate torn or stretched ligaments. It does not reverse the structural changes of rheumatoid erosion, os odontoideum, or a congenitally hypoplastic dens. It is not a treatment for frank, structural craniocervical or atlantoaxial instability with neurological compromise — those situations are the province of neurosurgeons and appropriate medical specialists, and care should be coordinated accordingly. If you have been diagnosed with, or are strongly suspected of having, true structural instability, our first role is to make sure you are connected with the right medical team, not to substitute for it.
Within those boundaries, here is where thoughtful, precise, low-force upper cervical chiropractic care can play a supportive role for appropriate patients. Our approach is built around the idea that the alignment and function of the top bones of the neck — the atlas and axis in particular — influence how the nervous system operates and how comfortably the head is carried. Our care is not high-velocity twisting manipulation. We do not crack or forcefully torque the neck. Instead, we use the Knee Chest Upper Cervical technique, a precise and low-force method of upper cervical correction that is specific to each patient’s measured misalignment. The gentleness and specificity of this approach are exactly why it appeals to people who are wary of aggressive neck adjustments.
Careful assessment comes first, and it is the most important part. We use 3D CBCT imaging to visualize the upper cervical anatomy in three dimensions, which lets us understand each patient’s individual bone structure and alignment with a level of detail that flat, two-dimensional films cannot provide. We also use Tytron paraspinal infrared thermographyto measure patterns of heat along the spine that reflect autonomic nervous system activity — an objective way to track how the nervous system is responding over time. Together, this information guides whether upper cervical care is appropriate at all, and if so, exactly how a correction should be delivered.
Screening is where honesty and safety meet. Part of a responsible upper cervical evaluation is looking for the very red flags and risk factors described earlier in this article. If your history, symptoms, or imaging raise concern for true structural instability — or if you belong to a high-risk group like Down syndrome, rheumatoid arthritis, or a connective tissue disorder — that changes everything about how we proceed. In some cases it means we coordinate with your physician or a specialist before doing anything hands-on; in some cases it means precise low-force care can proceed with appropriate caution and communication; and in some cases it means the most responsible recommendation is that upper cervical adjusting is not the right path for you, and we say so plainly. We would rather earn your trust with an honest “not yet” or “not us” than overpromise.
What precise low-force upper cervical care aims to offer appropriate patients is support for upper cervical function and comfort, delivered through customized care plans built around your individual findings rather than a one-size-fits-all routine. It is one piece of a larger picture — a picture that, for anyone with genuine instability, must include the right medical partners.
Ready to Talk With Us About Your Upper Neck?
If confusing upper neck symptoms have been weighing on you and you would like a careful, honest evaluation, we would be glad to help you understand your options. Call Lavender Family Chiropractic at (941) 243-3729, or request a visit through our new patient scheduling page. Our office is located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, right at the corner of University and Whitfield. We serve patients throughout Sarasota, Bradenton, Lakewood Ranch, and the surrounding communities with precise, low-force upper cervical care and a commitment to telling you the truth about what care can and cannot do.
What the Research Says
We think it is important to point you toward the underlying literature so you can read further and discuss it with your own providers. The following five peer-reviewed, open-access sources informed this article. None of them describe chiropractic treatment of instability; rather, they illuminate the anatomy, biomechanics, and clinical realities of these conditions.
- Fiester P, Rao D, Soule E, Orallo P, Rahmathulla G. Anatomic, functional, and radiographic review of the ligaments of the craniocervical junction. Journal of Craniovertebral Junction and Spine, 2021. This review details the ligamentous anatomy that stabilizes the skull-to-upper-neck junction, explaining how the alar, transverse, and related ligaments permit motion while restraining excessive movement — the foundation for understanding craniocervical instability.
- Ishak B, von Glinski A, Dupont G, et al. Update on the Biomechanics of the Craniocervical Junction, Part II: Alar Ligament. Global Spine Journal, 2021. This biomechanical review focuses on the alar ligament’s role as a key restraint of the craniocervical junction, particularly its function in limiting rotation and side-bending, which is relevant to both craniocervical and atlantoaxial stability.
- Cattarinussi L, Bregou A, Newman CJ, Merckaert SR. Radiological Screening of Atlantoaxial Instability in Children with Trisomy 21: A Systematic Review and Evidence-Based Recommendations. Children (Basel), 2025. This systematic review examines how atlantoaxial instability is screened for radiologically in children with Down syndrome and offers evidence-based recommendations, reflecting how important AAI is in this population.
- Song J, Mai E, Zhang J, et al. Rheumatoid Arthritis in the Cervical Spine: An Updated Review of Epidemiology, Imaging, and Surgical Indications. Spine Surgery and Related Research, 2026. This review summarizes how rheumatoid arthritis affects the cervical spine, including atlantoaxial involvement, along with imaging findings and the indications that guide surgical decision-making.
- Lohkamp LN, Marathe N, Fehlings MG. Craniocervical Instability in Ehlers-Danlos Syndrome — A Systematic Review of Diagnostic and Surgical Treatment Criteria. Global Spine Journal, 2022. This systematic review evaluates how craniocervical instability is diagnosed and, when necessary, surgically managed in patients with Ehlers-Danlos syndrome, underscoring both the association and the diagnostic complexity in connective tissue disorders.
Lifestyle and Precautions
If you are living with upper neck symptoms — whether or not structural instability has been confirmed — a few sensible, conservative habits can make daily life more comfortable while you pursue an accurate diagnosis. None of these are treatments for instability, and none replace medical care, but they reflect common-sense self-care for a sensitive region.
Be mindful of neck positions that consistently provoke your symptoms, and avoid pushing into them. Extreme end-range movements, sudden jerking motions, and high-impact activities are worth approaching cautiously, especially if you belong to one of the higher-risk groups discussed above. Supporting your head and neck well during sleep — with a pillow that keeps your neck in a neutral position rather than cranked up or twisted — is a simple change many patients find helpful. Pay attention to prolonged forward-head posture from phones and screens, which loads the upper neck in ways it was not designed to tolerate for hours at a stretch, and take frequent breaks to reset your posture.
If you have been told you have, or may have, instability, ask your medical team specifically about which activities are safe for you. Some higher-risk individuals are advised to avoid particular sports, amusement park rides, or activities that load the neck, and those recommendations should come from a physician who knows your case. It is also wise to be cautious with aggressive, high-velocity neck manipulation from any provider; this is one reason our practice uses only precise, low-force upper cervical correction rather than forceful twisting.
For more general context on the many causes of neck discomfort and conservative approaches to it, you may find our overview of neck pain a useful companion read. And if any of the red-flag neurological symptoms described earlier appear or worsen — progressive weakness, spreading numbness, coordination or walking difficulties, or changes in bladder or bowel control — treat that as a reason to seek prompt medical or emergency care rather than something to manage at home.
Serving Sarasota and Surrounding Communities
Lavender Family Chiropractic is proud to serve patients from across our region who are seeking precise, low-force upper cervical care and honest guidance about complex conditions like craniocervical and atlantoaxial instability. Our office sits at the corner of University and Whitfield, making us convenient to a wide swath of Southwest Florida.
We welcome patients from Sarasota, Bradenton, Lakewood Ranch, Venice, Palmer Ranch, Osprey, Siesta Key, Longboat Key, Lido Key, University Park, Parrish, Ellenton, Myakka City, Punta Gorda, and St. Petersburg. Whether you are just beginning to research your symptoms or you already have a diagnosis and are looking for a careful, communicative chiropractic partner to work alongside your medical team, we would be glad to hear from you.
Top 15 Questions
1. What is the main difference between craniocervical instability and atlantoaxial instability? Craniocervical instability (CCI) describes excessive motion across the whole skull-to-upper-neck junction (occiput, C1, and C2), centered on how the head sits on the spine. Atlantoaxial instability (AAI) is more specific, describing excessive movement at the C1-C2 joint, particularly around the dens (odontoid process). They overlap at C1-C2, which is why they are often discussed together.
2. Can they occur at the same time? Yes. Because the atlantoaxial joint is part of the craniocervical junction, a person can have both, or a picture that is weighted more toward one level than the other. This is exactly why individualized imaging and specialist evaluation matter when true structural instability is suspected.
3. Can you cure my instability with chiropractic care? No. We want to be completely honest about this: upper cervical chiropractic care does not cure craniocervical or atlantoaxial instability. It does not repair or tighten ligaments, and it is not a substitute for medical or surgical care when true structural instability is present. What precise, low-force upper cervical care can do for appropriate patients is support upper cervical alignment and function and provide an objective way to monitor the nervous system over time. If you have genuine instability, our role includes making sure you are connected with the right medical team.
4. What symptoms should make me seek urgent or emergency care rather than a chiropractic visit? Progressive weakness, spreading or worsening numbness or tingling in the arms or legs, loss of coordination, difficulty walking, changes in speech or swallowing, fainting, severe unrelenting headache, or any change in bladder or bowel control are red flags. These warrant prompt medical evaluation — often at an emergency room — not a wait-and-see approach and not spinal manipulation. When in doubt, err on the side of getting evaluated urgently.
5. Why is atlantoaxial instability such a concern in Down syndrome? Individuals with Down syndrome more commonly have ligamentous laxity and skeletal differences at the C1-C2 level, which raises the risk of atlantoaxial instability. Because of this, radiological screening and careful clinical vigilance are an established part of care in this population, and upper neck symptoms deserve especially careful medical attention.
6. How does rheumatoid arthritis lead to instability? Rheumatoid arthritis is a systemic inflammatory disease that can erode the ligaments and bone of the upper cervical spine over time, including the structures that hold the dens in place. This can lead to atlantoaxial subluxation. Anyone with longstanding RA who develops new neck pain or neurological symptoms should be evaluated with this possibility in mind.
7. I have Ehlers-Danlos syndrome. Does that mean I have instability? Not necessarily. EDS and related connective tissue disorders involve lax, fragile collagen, which raises the risk of craniocervical and atlantoaxial instability — but many people with EDS never develop clinically significant instability. It does mean upper neck symptoms should be evaluated thoughtfully and that any hands-on care must be chosen and delivered with extra caution.
8. Is your upper cervical technique the same as a forceful neck “crack”? No. We use the Knee Chest Upper Cervical technique, which is a precise, low-force method of correction specific to each patient’s measured misalignment. It is not high-velocity twisting manipulation. This gentleness and specificity are part of why patients concerned about their necks are comfortable with our approach.
9. How do you decide whether upper cervical care is appropriate for me? We start with a careful history, examination, and objective assessment using 3D CBCT imaging and Tytron paraspinal infrared thermography. We screen for red flags and risk factors. Based on all of that, we determine whether precise low-force care is appropriate, whether we should coordinate with your physician first, or whether upper cervical adjusting is not the right path for you. We will tell you honestly which of those applies.
10. What is 3D CBCT imaging and why do you use it? CBCT (cone beam computed tomography) produces a three-dimensional view of the upper cervical anatomy, letting us understand your individual bone structure and alignment in detail that flat, two-dimensional films cannot match. This precision helps us determine whether and exactly how a correction should be delivered.
11. What does the Tytron thermography scan measure? The Tytron uses paraspinal infrared thermography to measure patterns of heat along the spine that reflect autonomic nervous system activity. It is a non-invasive, objective way to track how your nervous system is responding over time, which helps guide care decisions.
12. Do you take insurance, and how does payment work? We are a cash-pay, out-of-network practice. That means payment is handled directly rather than billed through insurance networks. We can provide superbills — itemized receipts you can submit to your insurance company for possible out-of-network reimbursement, depending on your individual plan. We are happy to explain how this works before you begin, and we build customized care plans rather than generic routines.
13. Will you coordinate with my medical doctor or specialist? Yes, and for anyone with suspected or diagnosed structural instability, coordination is essential. Precise upper cervical care is one piece of a larger picture, and we believe in communicating with your medical team so everyone is working from the same information.
14. Can care help my symptoms even if I do not have structural instability? Many people with upper neck symptoms do not have true structural instability; their symptoms stem from more common causes. For appropriate patients, precise low-force upper cervical care aims to support upper cervical function and comfort. We cannot promise specific outcomes, and we will always be honest about what we are seeing in your case.
15. How do I get started? The simplest way is to call us at (941) 243-3729 or use our online new patient scheduling. We will walk you through the process, answer your questions, and make sure an evaluation is the right next step for you.
Closing
Craniocervical instability and atlantoaxial instability are related but distinct conditions, and understanding the difference — CCI as the broader skull-to-upper-neck picture, AAI as the specific C1-C2 story built around the dens — is the first step toward navigating them wisely. Both, in their true structural forms, are medical and often neurosurgical concerns that require accurate diagnosis, and no chiropractic care repairs ligaments or substitutes for that workup. What we offer at Lavender Family Chiropractic is precise, low-force upper cervical care for appropriate patients, thorough and honest assessment, careful screening for the concerns that matter, and a genuine willingness to coordinate with your medical team and to tell you the truth about what care can and cannot do.
If you are ready for a careful, honest conversation about your upper neck, we are here. Call (941) 243-3729, book online through our new patient scheduling page, or visit us at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, at the corner of University and Whitfield. You can also reach us anytime through our contact page.
Related Articles
- Craniocervical Instability (CCI) Overview
- How Craniocervical Instability Is Diagnosed
- CCI and Chiari Malformation
This article is for general educational purposes only and is not medical advice, diagnosis, or treatment. It does not create a doctor-patient relationship. Craniocervical and atlantoaxial instability are serious conditions that require evaluation by qualified medical professionals. If you have red-flag neurological symptoms, seek urgent medical care. Individual results vary, and no specific outcome is implied or promised.