By Dr. Rusty Lavender — Lavender Family Chiropractic, Sarasota, FL
How Is Craniocervical Instability Diagnosed? Few conditions in modern medicine are as confusing to live with, and as hard to pin down on paper, as craniocervical instability (CCI). People arrive at our Sarasota office having already spent months, sometimes years, collecting imaging reports that all say some version of the same three words: “unremarkable study.” Their necks feel anything but unremarkable. The head feels heavy, as if it needs to be held up with the hands. There are waves of dizziness, pressure at the base of the skull, brain fog, and a sense that something at the junction between the head and the neck simply is not holding steady. Yet the standard MRI, taken lying flat and still, comes back looking normal. That mismatch — a body that feels unstable and a scan that looks stable — is the single most common reason craniocervical instability goes unrecognized for so long.
The core of the problem is mechanical, and once you understand it, the whole diagnostic picture makes more sense. Craniocervical instability is, by definition, a problem of movement and load. It describes a craniocervical junction — the region where the skull (occiput) meets the first cervical vertebra (atlas, or C1) and the second (axis, or C2) — that allows too much motion under the ordinary demands of gravity and posture. A conventional MRI is designed to capture exquisite detail of soft tissue and bone while the patient lies perfectly still, supine, with the head supported. In that position, the very forces that reveal instability are removed. It is a bit like taking a photograph of a bridge with no traffic on it and concluding the bridge never sways.
This article is written to demystify how craniocervical instability is actually diagnosed by the physicians, radiologists, and neurosurgeons who specialize in it. We will walk through why standard supine MRI so often misses it, how upright, flexion-extension, and rotational imaging change the picture, and what the craniometric measurements — the clivo-axial angle (CXA), the Grabb-Oakes measurement (also called pB-C2), and the basion-dens interval (BDI) — actually mean when a specialist reads them. We will also be honest and specific about where a Sarasota upper cervical chiropractic practice like ours fits: we evaluate upper cervical alignment with our own in-office tools, and we help guide people toward the appropriate medical workup. We do not diagnose structural CCI ourselves, and understanding that boundary is part of getting the right care.
How Is Craniocervical Instability Diagnosed and Why Craniocervical Instability Is Hard to Diagnose
The standard, closed-bore MRI most people receive is a supine study. You lie on your back, your head rests in a padded coil, and the machine images your anatomy while you hold as still as possible. For most conditions this is exactly what you want — stillness produces sharp, detailed pictures. But for a condition defined by abnormal motion under load, stillness is precisely the wrong test condition. When you lie down, the roughly ten-to-twelve-pound weight of the head is no longer being supported by the ligaments and joints of the upper neck. The gravitational load that provokes symptoms disappears, and along with it, the mechanical evidence of instability can disappear too.
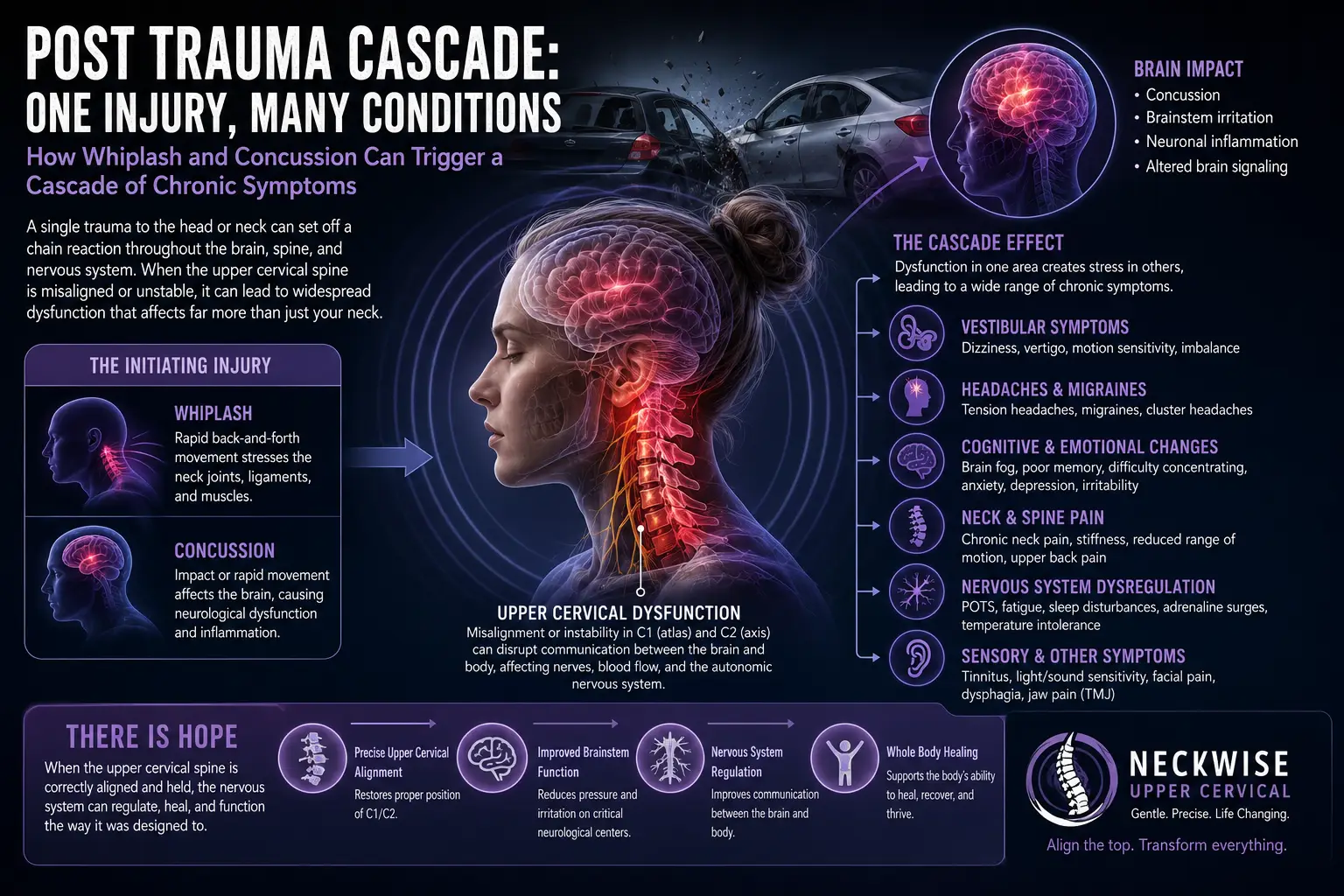
Craniocervical instability lives in the ligaments and joints that stitch the skull to the top of the spine. The alar ligaments, the transverse ligament, the tectorial membrane, and the joint capsules of the occiput-C1 and C1-C2 articulations are the primary restraints that keep the head from translating or tilting too far relative to the neck. When these tissues are lax — whether from a hereditary connective tissue disorder such as an Ehlers-Danlos syndrome, from trauma like a whiplash or a fall, or from repetitive strain — the junction can allow excess motion specifically when it is loaded and moved. A structural review of these ligaments underscores how central they are: the craniocervical junction depends on ligamentous integrity far more than bony interlock, so ligament laxity translates directly into clinical instability that a static image may not capture.
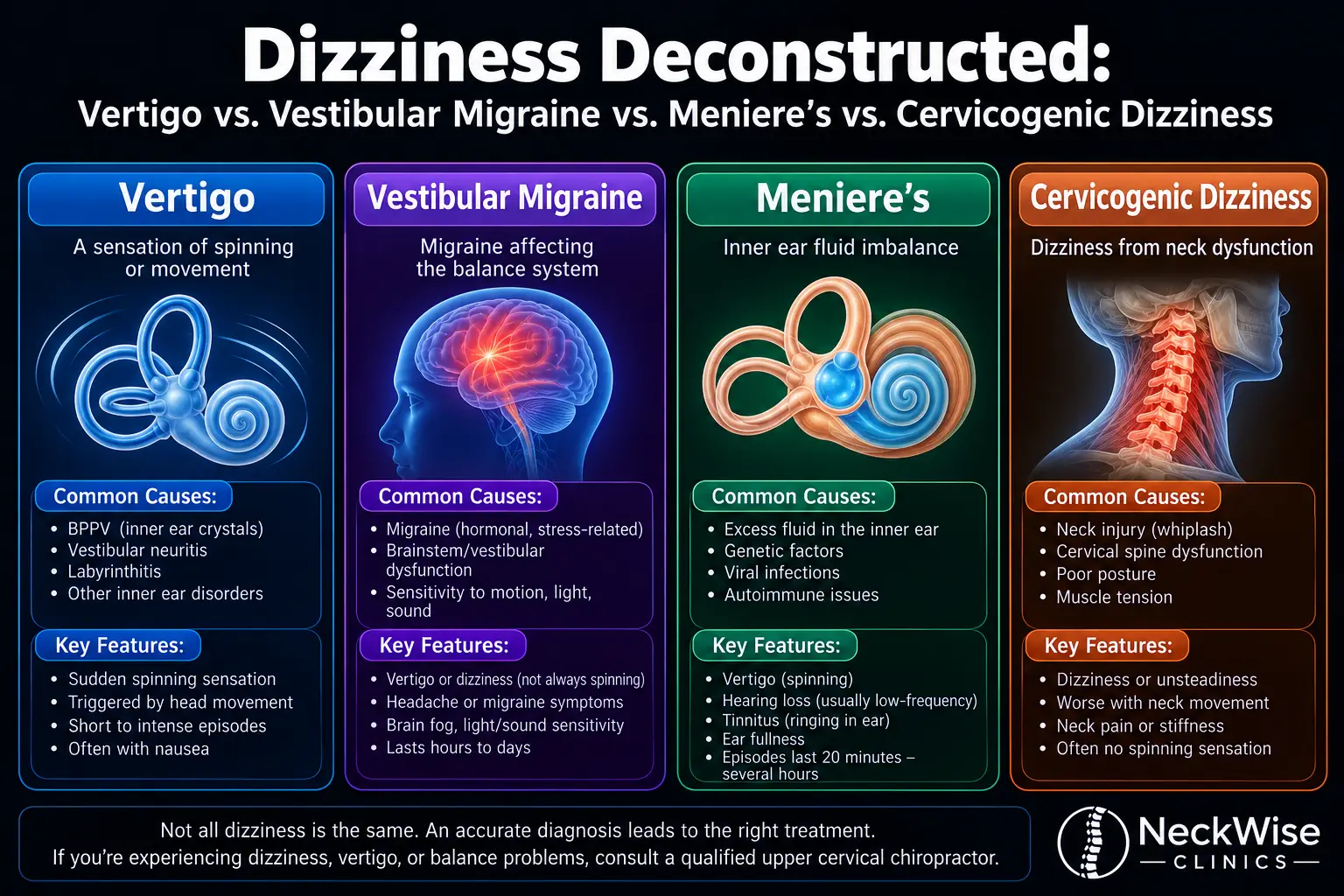
There is a second reason CCI is hard to diagnose, and it has nothing to do with the machine. The symptom picture overlaps with dozens of more common conditions. Headache at the base of the skull, dizziness, visual disturbance, difficulty swallowing, rapid heart rate on standing, fatigue, and cognitive fog can all be attributed to migraine, anxiety, vestibular disorders, dysautonomia, or simply “stress.” When the parts of the picture are examined one specialist at a time, no single one points clearly at the craniocervical junction. It is often only when someone steps back and considers the constellation together — especially in a person with joint hypermobility — that the junction becomes a suspect. Systematic reviews of CCI in connective tissue populations note exactly this: diagnosis rests on combining a suggestive clinical syndrome with dynamic, position-sensitive imaging and specific craniometric measurements, not on any one finding in isolation.
Finally, there is a measurement problem. Even when the right images are obtained, interpreting them requires familiarity with craniometrics — the geometry of lines and angles drawn between specific bony landmarks at the skull base and upper spine. These are not measurements that a general radiology report always includes, and the published thresholds have evolved over time. The takeaway for patients is simple but important: a “normal MRI” from a standard supine study does not rule out craniocervical instability, and getting an accurate answer usually means the right kind of imaging, read by someone who does this work regularly.
The Imaging: Upright, Flexion-Extension, and Rotational MRI
If supine stillness hides instability, the logical answer is to image the craniocervical junction the way it actually lives — upright, under load, and in motion. This is the reasoning behind several specialized imaging approaches that specialists use when CCI is suspected.
Upright MRI, sometimes called positional or weight-bearing MRI, is performed on an open scanner that allows the patient to be imaged while sitting or standing. Restoring gravity puts the true weight of the head back onto the ligaments and joints of the upper neck. In a person with a lax craniocervical junction, structures that sat in acceptable positions while lying down may shift measurably once the head has to be held up against gravity. Upright imaging can also be more comfortable and more feasible for people who cannot tolerate lying flat because doing so worsens their symptoms.
Flexion-extension imaging adds the dimension of movement. Rather than a single static pose, images are captured with the neck bent forward (flexion), held neutral, and tipped back (extension). The craniometric measurements are then compared across positions. In a stable junction, the key angles and distances stay within a narrow range regardless of head position. In an unstable junction, the numbers can swing — an angle that looks acceptable in neutral may become clearly abnormal in flexion, or a gap between two landmarks may widen when the neck extends. This dynamic comparison is frequently where instability finally becomes visible, because it exposes motion that no single snapshot can show. Reviews of craniocervical junction imaging in trauma emphasize this same principle: dynamic and multi-position views reveal abnormal translation and angulation that neutral studies routinely miss.
Rotational imaging, often performed with CT rather than MRI, addresses a different axis of motion. The C1-C2 joint is built for rotation — most of your ability to turn your head left and right happens there. Rotational CT captures the head turned fully to each side and looks for abnormal or asymmetric movement between C1 and C2, which can indicate rotational instability or fixation at that level. Because CT excels at showing bone, it is well suited to measuring how the atlas and axis move relative to one another during rotation.
It is worth being clear about a few practical realities. Upright and dynamic MRI are specialized studies. Not every imaging center offers them, and interpretation depends heavily on the reader’s experience with craniometrics. The images themselves are only half the answer; the measurements drawn on them, and the clinical context they are placed in, are what turn pictures into a diagnosis. This is medical imaging ordered and interpreted by physicians — radiologists, neurosurgeons, and neurologists who focus on the craniocervical junction. Our role at Lavender Family Chiropractic is different and complementary, and we will describe it plainly in a later section.
The Craniometric Measurements Explained
When a specialist evaluates the craniocervical junction for instability, they draw a set of standardized lines between bony landmarks and measure the angles and distances between them. These craniometrics are the numerical backbone of a CCI diagnosis. Three come up most often: the clivo-axial angle, the Grabb-Oakes measurement, and the basion-dens interval. Understanding what each one describes — in plain language — helps demystify the reports patients are handed.
The Clivo-Axial Angle (CXA)
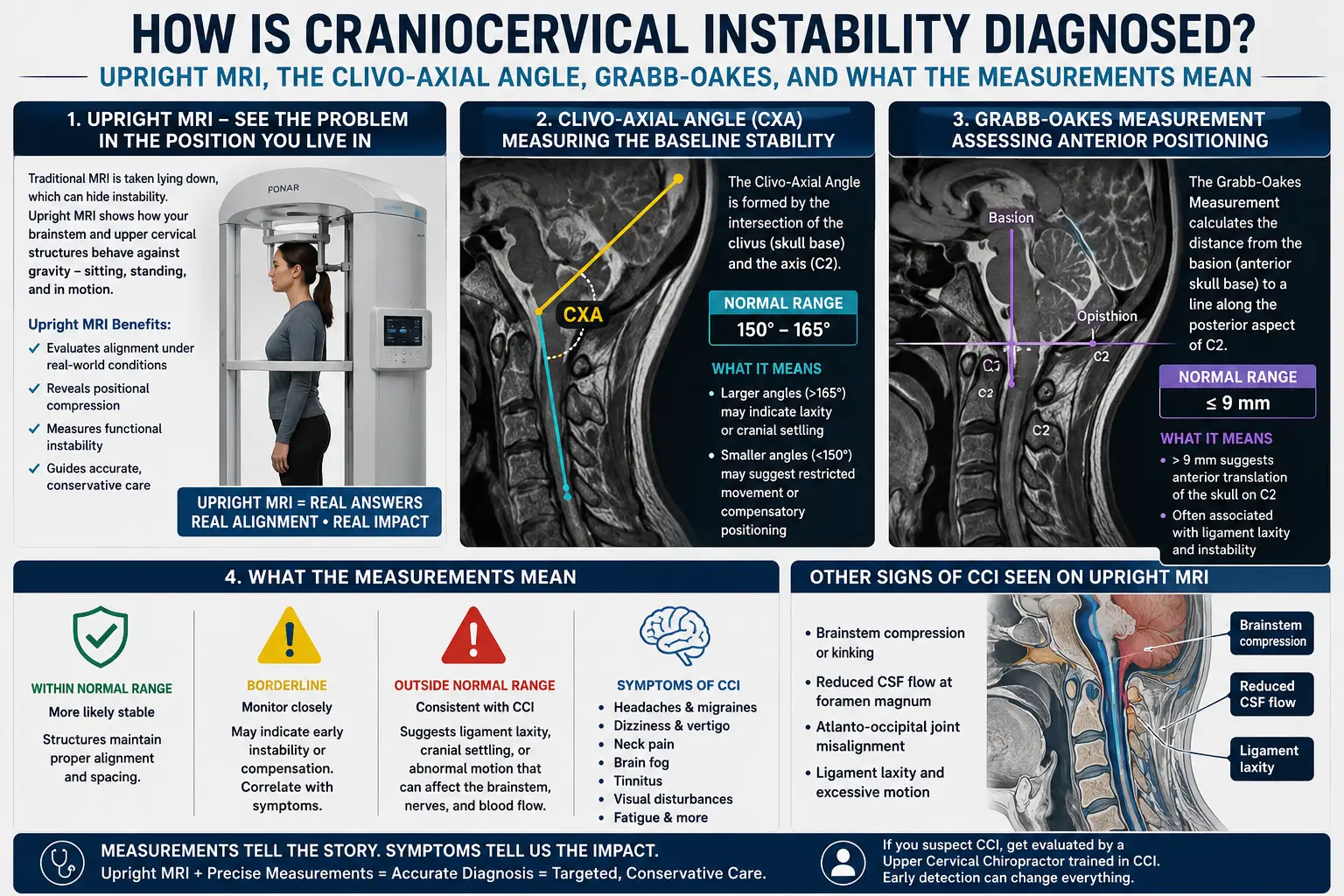
The clivo-axial angle is the angle formed between the clivus (the sloping bone at the base of the skull that leads down toward the foramen magnum, the large opening where the brainstem passes) and the axis (the C2 vertebra, specifically a line up the back of the odontoid and C2 body). In effect, the CXA measures how sharply the brainstem and upper spinal cord have to bend as they pass from the skull into the neck. Think of it as the angle of a garden hose at the point where it turns a corner: a gentle, open curve lets everything pass smoothly, while a sharp kink pinches the contents.
In a healthy craniocervical junction, the CXA is relatively open. Typical normal values reported in the literature fall roughly in the 145 to 160 degree range, with many sources describing a normal neutral angle around 150 to 160 degrees. As the angle closes down — becomes more acute — the ventral (front) surface of the brainstem and cord can be increasingly compressed and stretched over the odontoid. A CXA that falls below about 135 degrees is widely cited as a pathological threshold associated with brainstem deformation and the clinical picture of cervical medullary syndrome. Clinical research on cervical medullary syndrome secondary to craniocervical instability has used the CXA as a central metric, documenting that surgical correction which normalizes an abnormally kyphotic (closed) CXA can correspond with meaningful clinical change. The important nuance, especially relevant to dynamic imaging, is that the CXA is not fixed: it can look acceptable in a neutral, supine position and worsen in flexion, which is exactly why position-sensitive imaging matters.
The Grabb-Oakes Measurement (pB-C2)
The Grabb-Oakes measurement, also written as the pB-C2 line, quantifies ventral brainstem crowding — how much the tissue in front of the brainstem is bulging back toward it. It is drawn by first establishing a line (the “B-C2” line) from the basion (the front edge of the foramen magnum) to the back-bottom corner of the C2 body, and then measuring the perpendicular distance from that line to the dura (the covering) at the back of the odontoid tip. In everyday terms, it estimates how much the odontoid and the soft tissue around it are pushing into the space the brainstem needs to occupy.
A Grabb-Oakes value greater than about 9 millimeters is the commonly cited abnormal threshold, indicating enough ventral encroachment to potentially deform the brainstem and warrant close attention. The measurement was originally developed to help identify who might have ventral brainstem compression significant enough to consider surgical decompression. Contemporary work on basilar invagination and craniovertebral anomalies continues to evaluate the pB-C2 as a practical parameter for gauging the severity of ventral compression and for surgical decision-making, reinforcing its place alongside the CXA in the craniometric toolkit.
The Basion-Dens Interval (BDI)
The basion-dens interval measures the distance between the basion (the front lip of the foramen magnum, at the skull base) and the tip of the dens (the odontoid process, the peg of bone that projects up from C2). It is a marker of vertical stability at the craniocervical junction — specifically, whether the skull is sitting too far above the top of the spine or migrating in a way that suggests the vertical restraints have failed. In adults, a BDI greater than roughly 9 to 12 millimeters (thresholds vary by measurement method and imaging modality) raises concern for craniocervical dissociation or vertical instability, and it is a well-established parameter in trauma imaging where rapid identification of a distracted, unstable junction is lifesaving. Reviews of craniocervical junction imaging describe the BDI, along with related measurements, as part of the standard checklist for assessing the integrity of the skull-to-spine connection.
Why These Numbers Need a Specialist
Two points deserve emphasis. First, these measurements interact. No single number diagnoses CCI in isolation; specialists interpret the CXA, Grabb-Oakes, and BDI together, alongside dynamic behavior across positions and the whole clinical syndrome. Second, the published thresholds are guides, not absolute switches, and different studies define landmarks and cutoffs slightly differently. That is exactly why craniometrics belong in the hands of radiologists and neurosurgeons who read them regularly. A patient can and should understand what the measurements describe — that is the purpose of this article — but interpreting them for a real diagnosis is specialist work.
Where the Upper Neck (Atlas/Axis) and Our In-Office Evaluation Fit
So where does an upper cervical chiropractic practice fit into a picture dominated by upright MRI and craniometrics read by neurosurgeons? The honest answer, and the one we give every patient at Lavender Family Chiropractic, is that we occupy a specific and complementary role — and being clear about its edges is part of earning your trust.
We focus on the alignment and function of the upper cervical spine: the relationship of the atlas (C1) and axis (C2) to the head above and the spine below. This is the same anatomical neighborhood that craniometrics describe, which is why upper cervical care and the CCI conversation are so often intertwined. Our in-office assessment uses two primary tools. The first is 3D cone beam computed tomography (CBCT) imaging, which lets us evaluate upper cervical alignment in three dimensions with far more spatial detail than a conventional flat film. The second is Tytron paraspinal infrared thermography, a radiation-free scan that reads patterns of heat along the spine as an indirect window on how the nervous system is regulating the muscles and blood vessels of the paraspinal region. Together these give us an objective, measurable picture of how your upper cervical spine is positioned and how it is changing over time.
Here is the boundary we hold carefully. Our CBCT evaluates upper cervical alignment. It is not the same thing as the specialized medical diagnosis of structural craniocervical instability, which relies on upright and flexion-extension MRI, dynamic craniometric measurements like the CXA and Grabb-Oakes, and interpretation by physicians, radiologists, and neurosurgeons. We do not claim to diagnose structural CCI, and you should be cautious of anyone who tells you a chiropractic scan alone can. What we can do is evaluate whether your atlas and axis alignment is off, whether it corresponds with the symptoms you are describing, and whether your history and findings point toward the need for a formal medical workup. When they do, we say so, and we help you get there.
Our correction method is the Knee Chest Upper Cervical technique, a precise, low-force approach to influencing upper cervical alignment. It is important to distinguish this from the high-velocity twisting “manipulation” that many people picture when they hear “neck adjustment.” That forceful, rotational maneuver is not what we do. Our upper cervical chiropractic care is built around gentle, specific, carefully measured contacts guided by your imaging. For a person with a genuinely unstable craniocervical junction, high-velocity manipulation is the concerning approach — and it is precisely the approach we avoid. When we work with someone who may have upper cervical involvement, our low-force method and our willingness to refer are features, not afterthoughts.
Every person we see receives a customized care plan based on their individual imaging, history, and goals. There is no one-size-fits-all protocol here, and there is no scenario in which we would push forward with care that your presentation tells us belongs first in the hands of a medical specialist.
If you are in the Sarasota area and want an upper cervical alignment evaluation — or you simply want help understanding your imaging and figuring out your next step — we would be glad to talk. Call us at (941) 243-3729, book online through our new patient scheduling page, or visit us at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, at the corner of University and Whitfield. You can also reach us through our contact page.
What the Research Says
The following five peer-reviewed sources inform the imaging and measurement concepts described in this article. They are written for medical audiences, and we share them so you can see where these ideas come from and, if you choose, bring them into a conversation with your physician.
- Henderson FC, Francomano CA, Koby M, Tuchman K, Adcock J, Patel S. Cervical medullary syndrome secondary to craniocervical instability and ventral brainstem compression in hereditary hypermobility connective tissue disorders: 5-year follow-up after craniocervical reduction, fusion, and stabilization. Neurosurgical Review, 2019. This clinical study centers on craniometric measurements — including the clivo-axial angle and the Grabb-Oakes (pB-C2) measurement — and reports on outcomes in patients with craniocervical instability and ventral brainstem compression, illustrating how these numbers connect to the clinical syndrome.
- Lohkamp LN, Marathe N, Fehlings MG. Craniocervical Instability in Ehlers-Danlos Syndrome — A Systematic Review of Diagnostic and Surgical Treatment Criteria. Global Spine Journal, 2022. This systematic review examines how craniocervical instability is defined and diagnosed in patients with Ehlers-Danlos syndrome, surveying the diagnostic criteria and craniometric thresholds used across the published literature.
- Fiester P, Rao D, Soule E, Orallo P, Rahmathulla G. Anatomic, functional, and radiographic review of the ligaments of the craniocervical junction. Journal of Craniovertebral Junction & Spine, 2021. This review details the ligaments that stabilize the skull-to-spine junction and how they appear on imaging, explaining why ligamentous integrity is so central to craniocervical stability.
- Offiah CE, Day E. The craniocervical junction: embryology, anatomy, biomechanics and imaging in blunt trauma.Insights into Imaging, 2017. This imaging-focused review describes the anatomy and biomechanics of the craniocervical junction and walks through the measurements, including the basion-dens interval, used to assess its integrity when instability is a concern.
- Schneider D, Gandhi SV, Ward M, White TG, Brown EDL, Pennington Z, Zimering J, Latefi A, Rekate H, Sciubba DM, Lo SL. The Association Between Clival Axial Angle and Distal Junctional Failure After Craniocervical Fusion. Global Spine Journal, 2025. This study examines the clival (clivo-) axial angle as a meaningful geometric parameter at the craniocervical junction, reinforcing its role among the craniometrics specialists use to evaluate this region.
What to Bring and Ask at Your Evaluation
If you suspect craniocervical instability, walking into any evaluation — medical or chiropractic — prepared makes an enormous difference. Here is a practical checklist we share with patients.
Bring your actual imaging, not just the reports. Reports summarize; the images themselves can be re-examined. If you have had MRIs or CT scans, request the studies on disc or through a patient portal so any provider can view the source data. If you have had upright or flexion-extension imaging, that is especially valuable — bring it.
Bring a written symptom timeline. Note when symptoms began, whether there was a triggering event (a car accident, a fall, an illness, a period of rapid worsening), what makes symptoms better or worse, and how they change with head position. Because CCI is position- and load-sensitive, details like “my dizziness eases when I lie down and returns within a minute of standing” are genuinely diagnostic clues.
Bring any connective tissue history. If you or close family members have hypermobile joints, easy bruising, stretchy skin, frequent dislocations, or a diagnosed Ehlers-Danlos syndrome, that context matters. Connective tissue laxity is one of the strongest reasons to take a CCI question seriously.
Ask specific questions. Useful ones include: Does my imaging include the craniometric measurements — the clivo-axial angle, Grabb-Oakes/pB-C2, and basion-dens interval? Was my MRI taken supine only, or in upright and flexion-extension positions? Given my symptoms, would dynamic or upright imaging change the picture? And, importantly: which specialist should read these measurements?
Know when a symptom is a red flag. Some findings are not “schedule an appointment next week” issues — they are “seek urgent medical care now” issues. Progressive weakness in the arms or legs, new trouble with balance or walking, difficulty swallowing or breathing, slurred speech, fainting, or a sudden severe change after trauma all warrant emergency evaluation, not an outpatient visit. We will always tell you plainly if what you describe belongs in an emergency department.
At our office, your alignment evaluation with 3D CBCT and Tytron thermography adds an objective, measurable layer to this picture and helps clarify whether your upper cervical alignment is contributing to how you feel. If your symptoms point toward a structural CCI question, we help direct you to the right medical workup rather than trying to be everything at once. If you would like to understand a related symptom many of our patients describe, our article on why your head can feel too heavy to hold up explores that experience in more depth. If neck pain is a leading feature for you, our overview of neck pain and upper cervical care may also be helpful.
Serving Sarasota and Surrounding Communities
Lavender Family Chiropractic is proud to serve patients throughout Southwest Florida who are looking for careful, honest, low-force upper cervical care and help navigating complex craniocervical questions. From our office at the corner of University and Whitfield, we welcome people from Sarasota, Bradenton, Lakewood Ranch, Venice, Palmer Ranch, Osprey, Siesta Key, Longboat Key, Lido Key, University Park, Parrish, Ellenton, Myakka City, Punta Gorda, and St. Petersburg. Many of the people who find us have already been through several rounds of testing elsewhere, and they are looking for someone who will take the time to evaluate upper cervical alignment thoughtfully and be straightforward about what chiropractic care can and cannot answer. Wherever you are coming from in the region, we are glad to help you understand your situation and your next step.
Top 15 Questions About Diagnosing Craniocervical Instability
1. Can a normal standard MRI rule out craniocervical instability? Not reliably. A conventional MRI is taken lying flat and still, which removes the gravitational load and motion that reveal instability. A “normal” supine study does not rule out CCI. Specialists often need upright, flexion-extension, or rotational imaging to see instability that a static scan misses.
2. Can you diagnose craniocervical instability at your office? No, and we are careful to say so. We evaluate upper cervical alignment using 3D CBCT and Tytron thermography. The specialized diagnosis of structural CCI relies on upright and dynamic MRI plus craniometric measurements interpreted by physicians, radiologists, and neurosurgeons. Our role is to assess alignment and help guide you toward the appropriate medical workup.
3. What is the clivo-axial angle (CXA)? It is the angle between the clivus at the skull base and the axis (C2), essentially measuring how sharply the brainstem and cord bend as they pass from the head into the neck. Normal values are often cited around 145 to 160 degrees, and an angle below roughly 135 degrees is a commonly referenced pathological threshold. A specialist interprets it.
4. What is the Grabb-Oakes measurement (pB-C2)? It estimates how much tissue in front of the brainstem is crowding into the space the brainstem needs. A value greater than about 9 millimeters is the commonly cited abnormal threshold for ventral brainstem compression. It is one of several craniometrics specialists read together.
5. What is the basion-dens interval (BDI)? It measures the distance from the front of the foramen magnum (basion) to the tip of the odontoid (dens), a marker of vertical stability at the skull-to-spine junction. An enlarged BDI can indicate vertical instability or dissociation and is an important measurement in trauma imaging.
6. Why does upright MRI matter for CCI? Upright (weight-bearing) MRI restores gravity, putting the true weight of the head back onto the ligaments and joints of the upper neck. This can reveal shifts in position that vanish when you lie down, which is why it is often more informative than a supine study for a load-sensitive condition.
7. What does flexion-extension imaging show that a single scan does not? It captures the neck bent forward, neutral, and tipped back, then compares the craniometric measurements across positions. Instability often becomes visible only when the numbers change with movement — something a single snapshot cannot show.
8. Who actually diagnoses structural CCI? Physicians, radiologists, and neurosurgeons who specialize in the craniocervical junction. They order and interpret the specialized imaging and read the craniometric measurements. A diagnosis rests on combining the clinical syndrome with these dynamic, measured findings.
9. What causes craniocervical instability? Common contributors include hereditary connective tissue disorders such as the Ehlers-Danlos syndromes, trauma like whiplash or a fall, and sometimes inflammatory or degenerative processes that weaken the ligaments of the upper neck. Ligament laxity is central, which is why these tissues are the focus of the research.
10. What are the red-flag symptoms that mean I should go to the ER, not wait for an appointment? Progressive weakness in the arms or legs, new balance or walking difficulty, trouble swallowing or breathing, slurred speech, fainting, or a sudden severe change after trauma. These warrant emergency medical care. We will tell you directly if what you describe belongs in an emergency department.
11. How is your Knee Chest Upper Cervical technique different from a regular neck adjustment? It is a precise, low-force method guided by your imaging, not a high-velocity twisting manipulation. The forceful rotational maneuver many people picture is not what we do. Our approach is gentle and specific, which matters especially when the upper cervical region is involved.
12. Do you take insurance, and what does cash-pay mean here? We are a cash-pay, out-of-network practice. That means payment is handled directly rather than billed to insurance networks. We provide superbills you can submit to your insurance company for possible out-of-network reimbursement, depending on your individual plan. We are happy to explain how this works before you begin.
13. What is 3D CBCT, and how is it different from the MRI a neurosurgeon might order? Cone beam CT gives us a detailed three-dimensional view of upper cervical bony alignment. It is excellent for evaluating how your atlas and axis are positioned. It is an alignment tool, not a substitute for the upright and dynamic MRI and craniometric interpretation that a structural CCI diagnosis requires.
14. What is Tytron paraspinal thermography measuring? It is a radiation-free infrared scan that reads heat patterns along the spine as an indirect indicator of how the nervous system is regulating the paraspinal muscles and blood vessels. We use it alongside CBCT to track objective changes in your alignment and function over time.
15. If I already have imaging, should I bring it to my visit? Yes — bring the actual studies, not just the reports, along with a symptom timeline and any connective tissue history. This helps us evaluate your upper cervical alignment in context and, when appropriate, guide you toward the right specialist for a formal workup.
Closing
Craniocervical instability is hard to diagnose for reasons that make sense once you understand the mechanics: the condition is about motion and load, and the standard MRI removes both. The path to a clear answer usually runs through upright, flexion-extension, or rotational imaging and through craniometric measurements — the clivo-axial angle, Grabb-Oakes/pB-C2, and basion-dens interval — read by physicians who specialize in the craniocervical junction. Knowing what those measurements mean puts you in a stronger position to advocate for the right testing and to understand your own reports.
At Lavender Family Chiropractic in Sarasota, our part is focused and honest. We evaluate upper cervical alignment with 3D CBCT and Tytron thermography, we correct with the gentle, precise Knee Chest Upper Cervical technique, we build a customized care plan around your individual findings, and when your picture points toward a structural CCI question, we help guide you to the appropriate medical workup rather than overstate what we can do. That clarity is exactly the kind of care we would want for our own families.
If you would like an upper cervical alignment evaluation, or you simply want help making sense of your imaging and your next step, we are here. Call (941) 243-3729, book online through our new patient scheduling page, or visit us at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, at the corner of University and Whitfield. To reach us with a question first, use our contact page or call (941) 243-3729.
This article is for general educational purposes only and is not medical advice. It does not diagnose, treat, cure, or prevent any disease or condition. Craniocervical instability is a medical diagnosis made by qualified physicians. If you have red-flag neurological symptoms, seek urgent medical care.