By Dr. Rusty Lavender and Dr. Jacob Temple — Lavender Family Chiropractic, Sarasota, FL
Chiari Malformation: If you have spent time researching your own headaches, dizziness, brain fog, or that unsettling sense that your head feels heavy and unsupported on your neck, you have probably come across two terms that seem to circle each other again and again: craniocervical instability (CCI) and Chiari malformation. They show up on the same forums, in the same patient stories, and sometimes on the same MRI report. For many people, the confusion is deeply personal. They want to understand whether they have one condition, both, or neither — and they want to know who can actually help.
At Lavender Family Chiropractic in Sarasota, Florida, we work with the upper neck every day. That region, where the skull meets the top of the spine, is one of the most anatomically dense and mechanically important areas in the entire body. It is also the exact place where craniocervical instability and Chiari malformation meet. Because our focus is upper cervical alignment, patients often arrive asking us to sort out how these two conditions relate, what their symptoms have in common, and where careful, precise chiropractic attention might fit into a broader plan.
We want to be honest and clear from the very first paragraph, because honesty is the foundation of trust. Chiari malformation is a structural condition of the brain and skull base that is diagnosed and managed by neurologists and neurosurgeons using MRI. Upper cervical chiropractic care does not treat or correct Chiari malformation, and it is not a substitute for neurosurgical evaluation. What we can offer is thoughtful, low-force attention to how the upper neck is aligned, provided you are an appropriate candidate and your medical team is on board. This article is written to educate, to reduce fear through understanding, and to help you ask better questions of the right specialists.
What Is Chiari Malformation?
Chiari malformation is a structural abnormality at the base of the skull, in the region where the brain transitions into the spinal cord. To understand it, you first need to picture the foramen magnum. The foramen magnum is the large opening at the bottom of the skull through which the brainstem passes on its way to becoming the spinal cord. It is essentially the doorway between the head and the neck. Cerebrospinal fluid, the clear fluid that cushions and nourishes the brain and spinal cord, also flows back and forth through this opening with every heartbeat and breath.
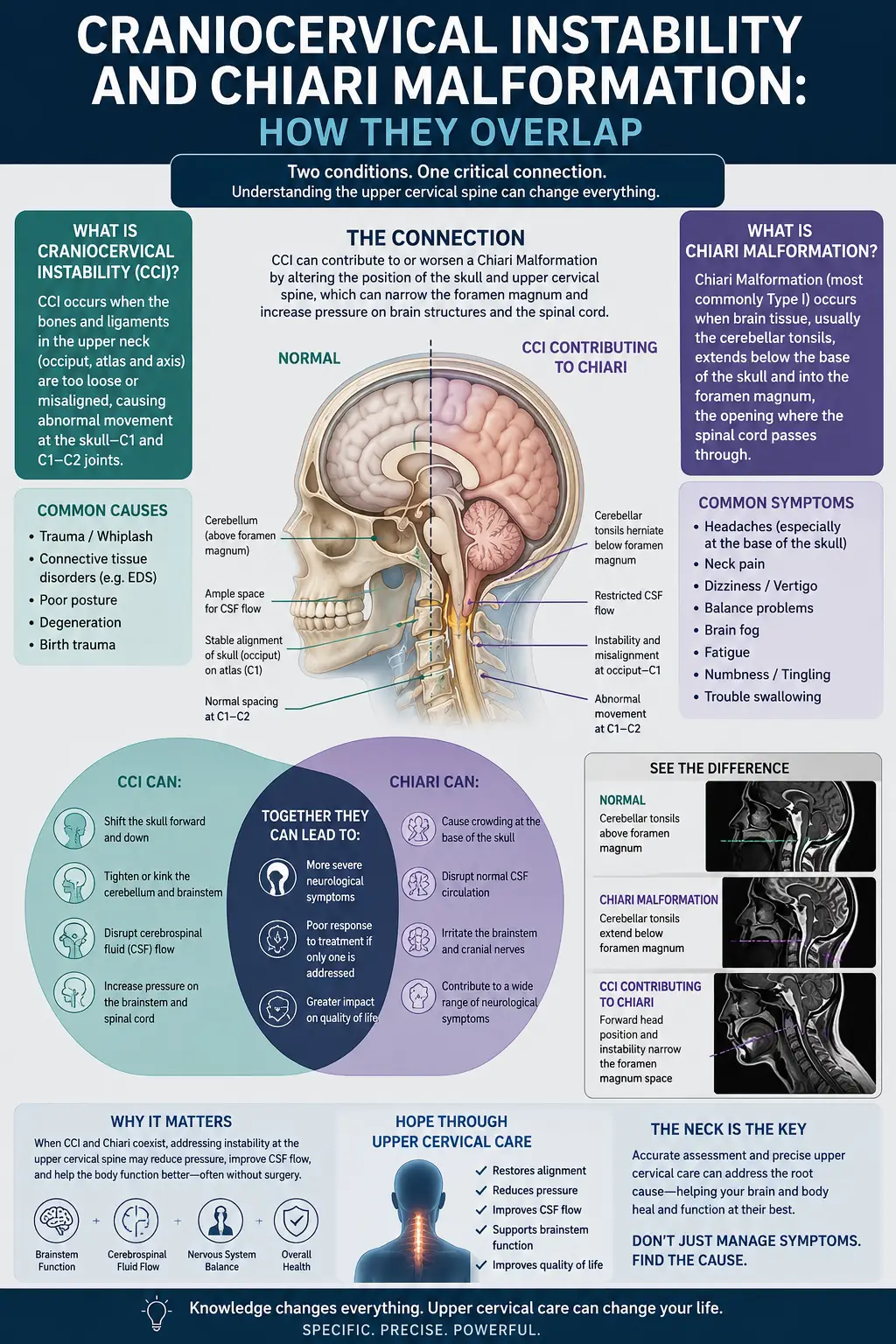
The most commonly discussed form is Chiari malformation type I, often written as Chiari I or CM-I. In Chiari I, the lower portion of the cerebellum — specifically the cerebellar tonsils — extends downward below the foramen magnum into the upper spinal canal. Radiologists generally describe this cerebellar tonsillar descent as being five millimeters or more below a reference line drawn across the base of the skull. When the tonsils sit lower than they should, they can crowd the space at the craniocervical junction, the anatomical meeting point of the skull and the top two vertebrae of the neck.
This crowding matters because the area is not designed to have extra tissue occupying it. The brainstem, the upper spinal cord, and the pathways for cerebrospinal fluid all share this narrow passage. When the cerebellar tonsils descend, they can partially obstruct the normal, rhythmic flow of cerebrospinal fluid through the foramen magnum and place pressure on the neural structures nearby. Over time, this altered fluid dynamic is thought to contribute to a range of symptoms and, in some people, to the formation of a fluid-filled cavity within the spinal cord called a syrinx, a condition known as syringomyelia.
The symptoms of Chiari malformation vary widely from person to person, which is part of why it can be so difficult to identify. Many people describe a headache that begins at the back of the head and upper neck and worsens with coughing, sneezing, laughing, or straining — anything that resembles a Valsalva maneuver. Other commonly reported experiences include neck pain, dizziness, balance problems, ringing in the ears, difficulty swallowing, visual disturbances, numbness or tingling in the hands, and a general feeling of pressure at the base of the skull. Some people have a noticeable Chiari malformation on imaging yet experience few or no symptoms, while others have significant symptoms that shape their daily lives.
Here is the point we cannot emphasize enough: Chiari malformation is diagnosed and managed medically. It is identified on MRI, and it is evaluated and treated by neurologists and neurosurgeons. When intervention is needed, the treatment is medical or surgical — for example, a procedure called posterior fossa decompression that creates more room at the base of the skull. No chiropractic technique, including ours, moves the cerebellar tonsils or changes the structure of the skull base. Understanding this clearly is the first step toward getting the right care from the right professionals.
What Is Craniocervical Instability, and How Do They Overlap?
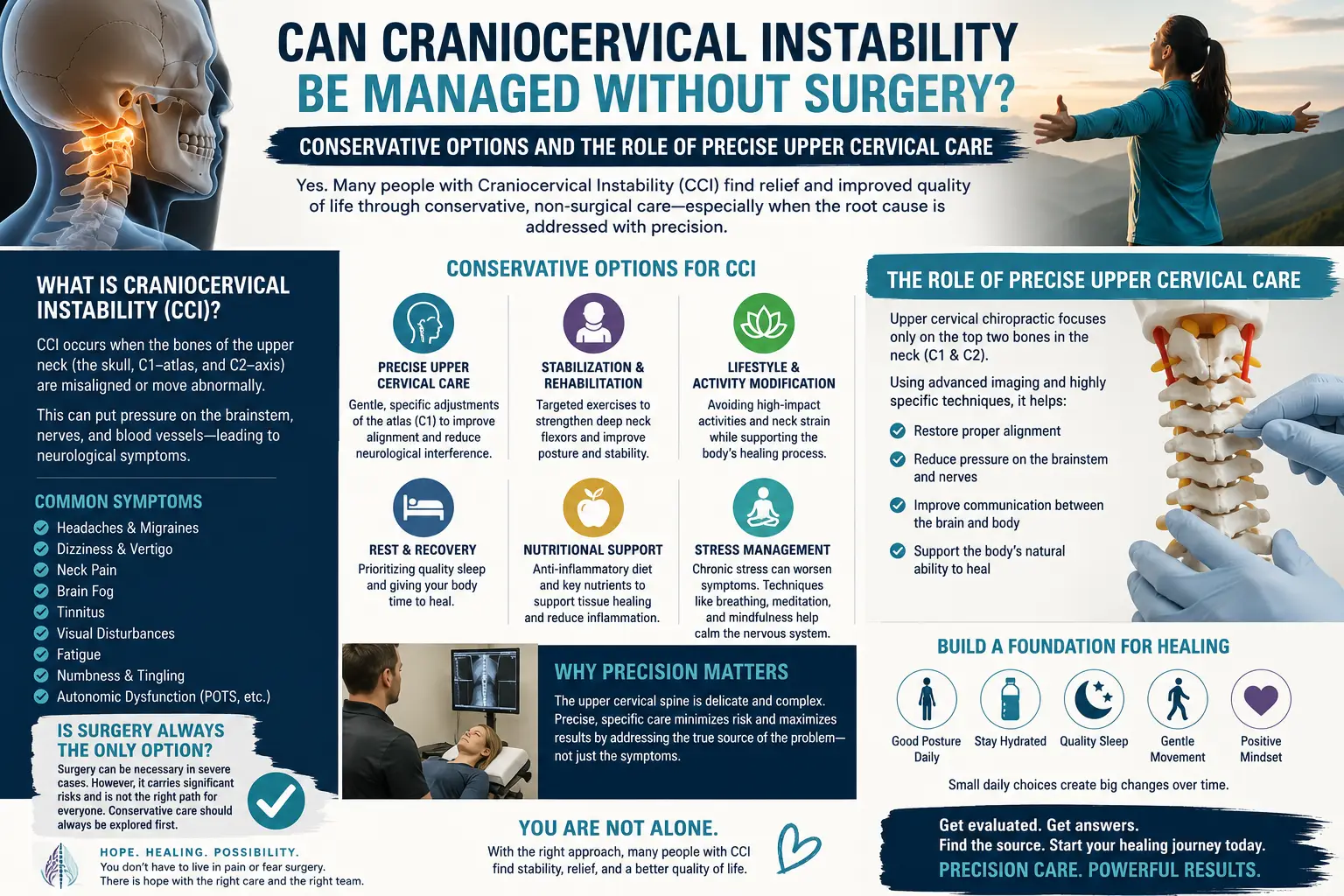
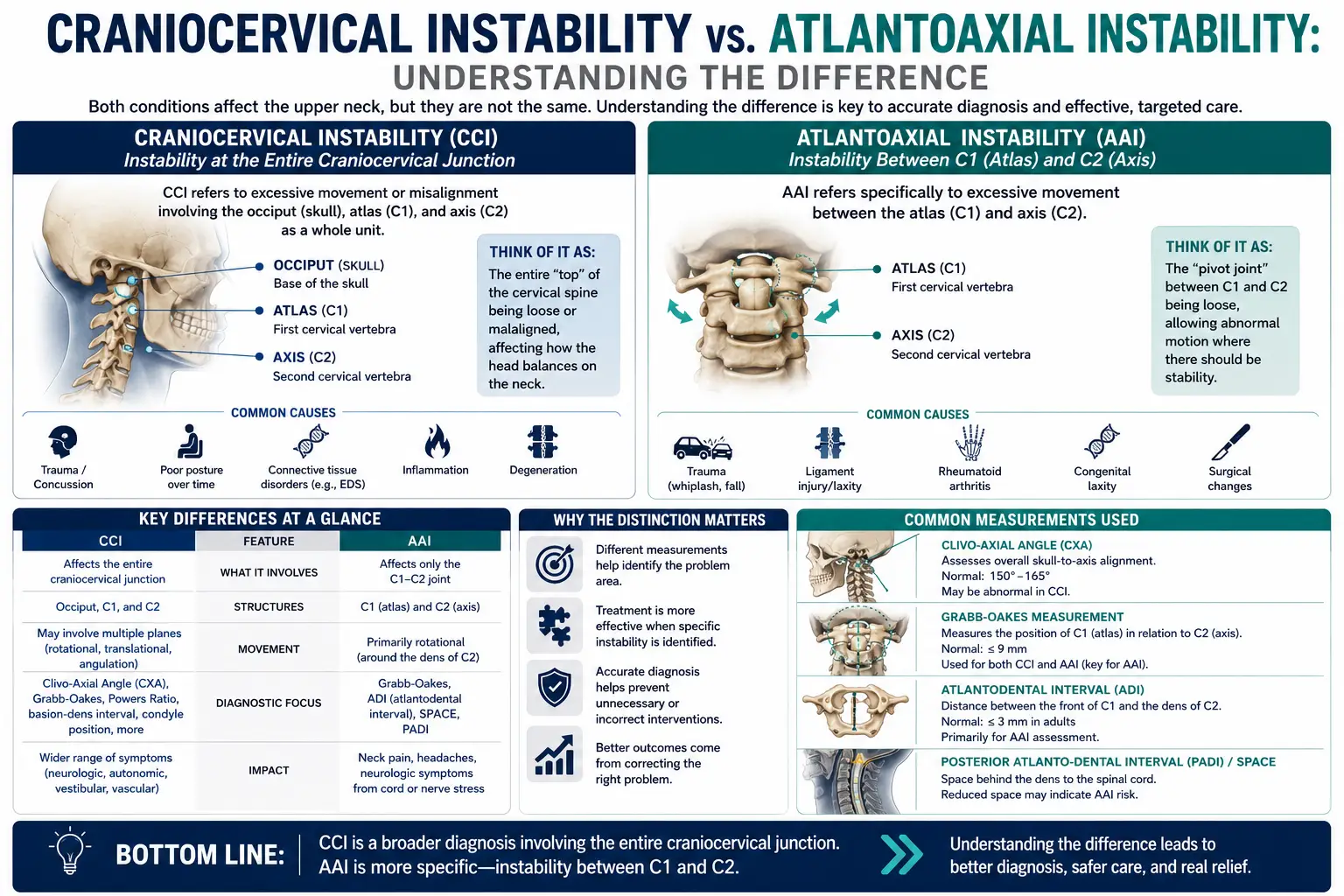
Craniocervical instability, or CCI, describes a condition in which the ligaments that connect the skull to the top of the cervical spine allow more movement between those structures than is considered normal or safe. The craniocervical junction is stabilized by a network of strong ligaments that hold the head in proper relationship to the first two vertebrae, the atlas and the axis. When those ligaments are lax, injured, or stretched, the head can shift excessively relative to the neck, and this abnormal motion can, in some cases, place strain on the brainstem and upper spinal cord.
CCI is more than a mechanical curiosity. When the connection between the skull and spine is unstable, the delicate neural structures passing through that region may be intermittently stressed, particularly with certain head and neck positions. People with CCI often describe a distinct and memorable symptom: their head feels too heavy for their neck to support, as though they need to hold it up with their hands, especially as the day goes on. This heavy-head sensation, along with headaches, dizziness, visual changes, and cognitive fog, is part of what draws so many people down the research rabbit hole in the first place.
Now for the overlap, which is the heart of this article. Craniocervical instability and Chiari malformation share the same real estate — the craniocervical junction — and they share a striking number of symptoms. Headaches at the base of the skull, dizziness and imbalance, visual disturbances, difficulty with fine motor tasks, brain fog, and neck pain appear on both lists. Because the symptom pictures overlap so heavily, it is genuinely difficult for a patient, and sometimes even for clinicians early in the process, to tell which condition is driving which symptom, or whether both are contributing.
The two conditions can also physically co-occur, and this is where the relationship becomes clinically important. In some people, the cerebellar tonsils descend below the foramen magnum (a Chiari picture) at the same time that the ligaments of the craniocervical junction are lax (a CCI picture). When crowding from tonsillar descent combines with instability from ligamentous laxity, the craniocervical junction may be stressed from two directions at once. Neurosurgical literature sometimes refers to this more layered presentation as a complex Chiari, in which instability or brainstem compression is present alongside the tonsillar descent, and both must be considered together during evaluation.
This co-occurrence is not random. It appears with notable frequency in people who have heritable connective tissue disorders, most commonly the Ehlers-Danlos syndromes. Connective tissue is the body’s structural glue, and ligaments are made of it. When a person’s connective tissue is more elastic and less supportive than average — as it is in many forms of Ehlers-Danlos syndrome — the ligaments throughout the body, including those crucial stabilizers at the skull base, may be more prone to laxity. That same underlying biology can be associated with both craniocervical instability and, in some individuals, Chiari-type crowding at the foramen magnum. This is why so many patients who research one of these conditions quickly find themselves reading about the other, and about connective tissue disorders as well.
The Mechanisms at the Craniocervical Junction
To really understand why craniocervical instability and Chiari malformation produce such similar symptoms, it helps to walk through what actually lives at the craniocervical junction and what can go wrong there. This is a small space doing an enormous amount of work.
First, consider the brainstem and upper spinal cord. The brainstem is the control center for many of the body’s most automatic and vital functions, including aspects of heart rate, breathing, blood pressure regulation, balance, and the coordination of many cranial nerves. As the brainstem passes through the foramen magnum and becomes the spinal cord, it runs directly through the craniocervical junction. Anything that crowds this space, such as descended cerebellar tonsils, or anything that allows abnormal motion in this space, such as ligamentous instability, has the potential to irritate or place pressure on these structures. Because the brainstem influences so many systems, irritation here can produce a scattered, hard-to-pin-down collection of symptoms rather than one clean, obvious sign.
Second, consider cerebrospinal fluid flow. Cerebrospinal fluid does not sit still; it pulses back and forth through the foramen magnum in rhythm with the cardiac cycle, cushioning the brain and spinal cord and helping regulate pressure. In Chiari malformation, the descended tonsils partially obstruct this passage, and the smooth, pulsatile flow becomes turbulent or reduced, particularly during the systolic phase of the heartbeat. Researchers studying this phenomenon with specialized phase-contrast MRI have documented impaired fluid flow just below the foramen magnum in people with Chiari I, along with changes in that flow after decompression surgery. Disrupted fluid dynamics are thought to contribute to headaches and pressure symptoms and, over time, to the development of a syrinx within the cord.
Third, consider the ligaments themselves. The craniocervical junction is held together by a set of specialized ligaments — including the alar ligaments and the tectorial membrane, among others — that allow the head to nod and rotate while still keeping the skull anchored securely to the spine. These ligaments are the guardrails of the junction. When they are healthy, they permit generous, controlled movement. When they are lax or injured, the guardrails loosen, and the head can move too far relative to the neck. That excessive motion is the essence of craniocervical instability, and it can intermittently narrow the space available for the brainstem and cord and disturb the same fluid pathways affected in Chiari.
Now you can see why the symptoms overlap so much. Whether the space at the foramen magnum is compromised by crowding (Chiari) or by abnormal motion (CCI), or by both at once, the structures at risk are the same: the brainstem, the upper cord, and the cerebrospinal fluid pathways. The body does not always distinguish neatly between these mechanisms in the symptoms it produces. A person with pure Chiari, a person with pure CCI, and a person with both may all describe occipital headaches, dizziness, visual disturbance, and cognitive fog. This is precisely why careful medical imaging and specialist evaluation are so important, and why guessing is not good enough.
It is also why the ligaments of the craniocervical junction have been the subject of detailed anatomical and radiographic study. Understanding exactly which ligaments stabilize the junction, how they appear on MRI, and how injury or laxity manifests helps physicians distinguish instability from other causes of craniocervical symptoms and decide who might benefit from which intervention. This is careful, evidence-based medicine, and it is the terrain of neurologists, neurosurgeons, and radiologists.
Where the Upper Neck and Precise Upper Cervical Care May Fit — and Where It Does Not
This is the section where we have to be the most careful and the most honest, because it is the section where patients most want a simple answer and where a simple answer would be misleading.
Let us begin with what we do not do. We do not treat Chiari malformation. Upper cervical chiropractic care does not move the cerebellar tonsils, does not enlarge the foramen magnum, and does not change the structure of the skull base. Chiari malformation is a structural, neurosurgical condition, and it is evaluated and managed by neurologists and neurosurgeons using MRI. Likewise, our care does not repair or tighten ligaments. If the ligaments of the craniocervical junction are lax or injured, no chiropractic adjustment restores them to their original strength. We want you to hear this plainly, because any practitioner who tells you otherwise is not being straight with you. Our care is not a substitute for medical or surgical evaluation, and it is not a treatment for the underlying structural conditions themselves.
So where might careful upper cervical attention fit at all? For appropriately selected patients — and only in coordination with their physicians — supportive attention to upper cervical alignment may be part of a broader, medically supervised plan. The upper neck is a region we work in with a great deal of specificity, and some people with craniocervical symptoms have alignment considerations in the upper cervical spine that are separate from, though related to, their diagnosed structural condition. When a patient’s medical team agrees that gentle, precise care is reasonable, our role is to offer that supportive attention thoughtfully, never as a cure and never as a replacement for the medical management they need.
The way we work matters enormously here, and this is a crucial point of distinction. Our method is the Knee Chest Upper Cervical technique, a precise, low-force approach to the upper cervical spine. This is not high-velocity twisting or forceful manipulation of the neck. It is a specific, gentle correction based on careful measurement and analysis. For a region as sensitive as the craniocervical junction, that precision and low force are exactly why patients with complex upper-neck concerns seek out this style of care rather than aggressive manual techniques. You can learn more about our overall approach on our upper cervical chiropractic care page.
Precision begins with measurement, not assumption. Before any care, we use 3D CBCT imaging to see the individual anatomy of your upper cervical spine in three dimensions, and Tytron paraspinal infrared thermography to assess patterns in the nervous system objectively over time. These tools help us understand your specific structure and decide whether upper cervical care is even appropriate for you. Importantly, if your history, symptoms, or imaging raise concern for a structural condition like Chiari malformation or significant instability, our role is to encourage and support the medical evaluation you need — not to proceed as though alignment care were the answer to a structural problem.
We also believe strongly in individualized care rather than one-size-fits-all programs. Our customized care plans are built around your particular situation, your medical diagnoses, and the guidance of your physicians. For patients navigating conditions as serious as Chiari malformation and craniocervical instability, coordination is everything. The best outcomes come from a team in which neurologists and neurosurgeons lead the diagnosis and management of the structural conditions, and supportive practitioners like us contribute only within the boundaries that make sense for that individual.
Finally, a word about red flags, because it belongs right here. Certain symptoms are signals to seek urgent medical care rather than any form of routine outpatient treatment. Sudden or severe headache unlike any you have had before, new weakness in the arms or legs, difficulty swallowing or speaking, loss of coordination, fainting, changes in vision, difficulty breathing, or loss of bowel or bladder control are all reasons to contact your physician immediately or go to the emergency room. Precise upper cervical care is not the appropriate response to red-flag neurological symptoms. We will always tell you so, and we will help you get to the right level of care.
Ready to Talk With an Upper Cervical Team in Sarasota?
If you are living with upper neck symptoms and want to understand how careful, low-force upper cervical care might fit alongside your medical management, we are here to talk it through honestly. Call Lavender Family Chiropractic at (941) 243-3729, or book directly through our new patient scheduling page. Our office is located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, at the corner of University and Whitfield. We will listen carefully, review your history, and be straightforward about whether and how we may be able to help — including when the right answer is to point you toward the medical specialists you need.
What the Research Says
The relationship between craniocervical instability, Chiari malformation, connective tissue disorders, and cerebrospinal fluid flow is an active area of medical research. Below are five peer-reviewed sources that inform the general concepts discussed in this article. These are provided for education and are not a substitute for evaluation by a qualified physician.
- Henderson FC, et al. Cervical medullary syndrome secondary to craniocervical instability and ventral brainstem compression in hereditary hypermobility connective tissue disorders: 5-year follow-up after craniocervical reduction, fusion, and stabilization (Neurosurgical Review, 2019). This study examined patients who had both Chiari malformation and craniocervical instability in the setting of hereditary connective tissue disorders, illustrating how instability, brainstem compression, and tonsillar descent can occur together in the same individuals.
- Henderson FC, et al. Craniocervical Instability in Ehlers-Danlos Syndrome—A Systematic Review of Diagnostic and Surgical Treatment Criteria (Global Spine Journal, 2023). This systematic review analyzes how craniocervical instability is diagnosed and surgically managed in people with Ehlers-Danlos syndrome, highlighting the connective tissue link and the current lack of consensus on imaging thresholds.
- Alhosani MS, Gachechiladze S. Chiari Malformation Type I: A Review of Pathophysiology, Cerebrospinal Fluid Flow Dynamics, Diagnosis, Surgical Management, and Its Relationship to Syringomyelia (Cureus, 2026). This narrative review defines Chiari I as tonsillar herniation through the foramen magnum and explains how the resulting obstruction of cerebrospinal fluid flow and brainstem compression relate to symptoms and syrinx formation.
- Trimarchi F, et al. Insights on the Hydrodynamics of Chiari Malformation (Journal of Clinical Medicine, 2022). Using phase-contrast MRI before and after surgery, this study quantifies cerebrospinal fluid and blood flow to show how neurofluid dynamics at the craniocervical junction are affected by Chiari malformation and its treatment.
- Fiester P, et al. Anatomic, functional, and radiographic review of the ligaments of the craniocervical junction(Journal of Craniovertebral Junction and Spine, 2021). This review details the stabilizing ligaments of the craniocervical junction, including the alar ligaments, and how they appear on MRI, providing anatomical context for how ligamentous injury or laxity contributes to instability.
Living With These Conditions: Self-Care Considerations
Living with craniocervical instability, Chiari malformation, or both can be exhausting, and much of daily life becomes an exercise in managing your energy and protecting a sensitive region. While self-care never replaces medical management, many patients find that thoughtful daily habits help them feel more stable and less overwhelmed. Always run new strategies by your physician first, especially if you have a diagnosed structural condition, because what helps one person may not be appropriate for another.
Posture and head support are often the first place people focus. Because so many patients describe the sensation that their head feels too heavy for their neck, positioning matters. Being mindful about how long you spend with your head tipped forward over a phone or laptop, arranging screens at eye level, and using supportive pillows that keep the neck in a neutral position at night can reduce the constant low-grade strain on the craniocervical junction. Some people find that a period of intentional rest with the head well supported eases their symptoms after a demanding day. If you want to read more about that specific heavy-head experience and the upper neck, we discuss it in our article on why your head can feel too heavy for your neck.
Avoiding provocative movements is another common theme. Many people with these conditions learn, through trial and error, that certain positions or activities reliably trigger their symptoms — sudden neck extension, heavy lifting with a held breath, high-impact exercise, or roller coasters and other rides that whip the head around. Learning your personal triggers and steering around them is not weakness; it is intelligent self-protection. Because forceful strain can matter here, this is also why our own care is precise and low-force rather than aggressive.
Pacing and stress management deserve attention too. The nervous system connections that run through the craniocervical junction include pathways that influence the body’s automatic functions, and many patients notice that fatigue, stress, and poor sleep amplify their symptoms. Gentle, physician-approved movement, hydration, consistent sleep, and stress-reduction practices such as slow breathing can support overall nervous system regulation. Some patients are also interested in how the vagus nerve, which passes near this region, relates to symptoms like digestive changes, heart rate variability, and that wired-but-tired feeling; we explore that topic in our article on vagus nerve dysfunction.
Finally, build a good team and keep good records. Track your symptoms, note what makes them better or worse, and bring that information to your appointments. Keep your neurologist and neurosurgeon informed, and make sure any supportive practitioner you see, including a chiropractor, understands your full diagnosis and coordinates with your physicians. The people who tend to do best with complex craniocervical conditions are the ones who assemble a communicative, honest care team and stay in the driver’s seat of their own health.
Serving Sarasota and Surrounding Communities
Lavender Family Chiropractic is proud to serve patients throughout Southwest Florida from our office at the corner of University and Whitfield. While Chiari malformation and craniocervical instability are managed medically, patients who want honest, precise, low-force upper cervical care as a supportive part of their broader plan travel to us from across the region. We welcome patients from Sarasota, Bradenton, Lakewood Ranch, Venice, Palmer Ranch, Osprey, Siesta Key, Longboat Key, Lido Key, University Park, Parrish, Ellenton, Myakka City, Punta Gorda, and St. Petersburg.
Whether you live minutes away in Sarasota or drive in from Venice, Punta Gorda, or St. Petersburg, our commitment is the same: a careful, individualized evaluation, straightforward communication about what upper cervical care can and cannot do, and coordination with your medical team. If you are unsure whether we are the right fit for your situation, we would rather have that honest conversation up front than make promises we cannot keep. You can always reach us through our contact page or by phone.
Top 15 Questions
- Can chiropractic treat or correct Chiari malformation? No. This is important, so we want to be completely clear: chiropractic care, including our precise upper cervical technique, does not treat or correct Chiari malformation. Chiari is a structural condition diagnosed on MRI and managed by neurologists and neurosurgeons. We do not move the cerebellar tonsils or change the skull base. Our care is not a substitute for neurosurgical evaluation.
- What is the difference between Chiari malformation and craniocervical instability? Chiari malformation involves the cerebellar tonsils descending below the foramen magnum, crowding the craniocervical junction. Craniocervical instability involves lax or injured ligaments allowing excessive motion between the skull and upper spine. They are different mechanisms that can produce overlapping symptoms, and they sometimes occur together in the same person.
- Why do these two conditions cause such similar symptoms? Both affect the same crowded space at the craniocervical junction, where the brainstem, upper spinal cord, and cerebrospinal fluid pathways all pass. Whether the space is compromised by crowding or by abnormal motion, the structures at risk are the same, so the symptoms — headaches, dizziness, visual changes, brain fog — overlap heavily.
- Are these conditions related to Ehlers-Danlos syndrome? They can be. Heritable connective tissue disorders such as the Ehlers-Danlos syndromes are associated with more elastic, less supportive ligaments, which can predispose a person to craniocervical instability and, in some cases, to Chiari-type crowding as well. Many patients researching one topic quickly encounter the others.
- How are these conditions diagnosed? Through medical imaging and specialist evaluation. Chiari malformation is diagnosed on MRI. Instability is assessed by physicians using imaging, sometimes including positional or dynamic studies, along with clinical examination. Diagnosis is the domain of neurologists, neurosurgeons, and radiologists.
- Does your chiropractic care repair ligaments? No. Our care does not repair, tighten, or restore injured or lax ligaments. If ligamentous instability is present, that is a medical matter. We are honest about this because your trust depends on it.
- What technique do you use, and is it forceful? We use the Knee Chest Upper Cervical technique, which is a precise, low-force approach. It is not high-velocity twisting or forceful neck manipulation. For a sensitive region like the upper neck, that precision and gentleness are exactly the point.
- What imaging do you use in your office? We use 3D CBCT imaging to view your upper cervical anatomy in three dimensions and Tytron paraspinal infrared thermography to assess nervous system patterns objectively over time. These tools help us understand your structure and decide whether upper cervical care is appropriate for you.
- Do you take insurance? We are a cash-pay, out-of-network practice. This allows us to focus on individualized care rather than insurance restrictions. We provide superbills you can submit to your insurance company for possible reimbursement, depending on your specific plan and benefits.
- What is a superbill and how does it work? A superbill is an itemized receipt of the care you received, including the necessary codes, that you can submit to your insurance company on your own. Whether you are reimbursed depends on your individual out-of-network benefits. We are happy to provide superbills for you to submit.
- Do you offer customized care plans? Yes. We build individualized care plans around your specific situation, your medical diagnoses, and the guidance of your physicians. We do not use one-size-fits-all programs, and our plans are designed with your particular needs and medical team in mind.
- When should I go to the emergency room instead of seeking chiropractic care? Seek urgent medical care right away for red-flag symptoms such as a sudden or severe headache unlike any before, new weakness in the arms or legs, difficulty swallowing or speaking, loss of coordination, fainting, sudden vision changes, difficulty breathing, or loss of bowel or bladder control. These require emergency evaluation, not routine outpatient care.
- Can upper cervical care help with my symptoms if I have Chiari or CCI? Only in certain situations, and only in coordination with your physicians. For appropriately selected patients whose medical team agrees it is reasonable, supportive attention to upper cervical alignment may be one part of a broader, medically led plan. It is never a cure and never a replacement for medical or surgical management.
- Will you coordinate with my neurologist or neurosurgeon? Yes, and we encourage it. For complex craniocervical conditions, communication among your providers is essential. We see our role as supportive and bounded, with your medical specialists leading the diagnosis and management of the structural conditions.
- How do I get started or ask more questions? Call us at (941) 243-3729 or use our online scheduling page. We will review your history, talk honestly about whether upper cervical care fits your situation, and, when appropriate, encourage the medical evaluation you may need. Being straightforward with you is more important to us than filling our schedule.
Closing CTA
Craniocervical instability and Chiari malformation are serious, overlapping conditions that deserve careful medical evaluation and a coordinated team. At Lavender Family Chiropractic, our contribution is honest, precise, low-force upper cervical care for appropriate patients, offered only alongside the neurological and neurosurgical care these conditions require. If you would like a straightforward conversation about your upper neck and where careful chiropractic attention may or may not fit, we would be glad to help.
Call us at (941) 243-3729, book through our new patient scheduling page, or visit us at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, at the corner of University and Whitfield. Dr. Rusty Lavender and Dr. Jacob Temple look forward to listening to your story and helping you find your next right step.
Related Articles
- Craniocervical Instability: The Complete Guide — Start here. Our comprehensive pillar article on craniocervical instability explains the condition in depth and connects to the full library of related topics, including this one.
- Why Your Head Feels Too Heavy for Your Neck — A closer look at the heavy-head sensation, dizziness, and vertigo that so often accompany upper cervical concerns.
- Vagus Nerve Dysfunction — How the vagus nerve, which passes near the craniocervical junction, relates to symptoms like digestive changes, heart rate, and that wired-but-tired feeling.