By Dr. Rusty Lavender — Lavender Family Chiropractic, Sarasota, FL
Conservative care Options: If you have been told you may have craniocervical instability (CCI), or you suspect it because of a heavy-feeling head, unrelenting neck pain, dizziness, brain fog, or symptoms that flare when you hold your head upright for too long, one of the first questions you probably asked was some version of this: “Do I need surgery?” It is an understandable and important question, and it deserves an honest answer rather than a sales pitch. The truth is that craniocervical instability exists on a spectrum. Some people have severe, well-documented instability with progressive neurological signs, and for them, a surgical evaluation is essential and appropriate. Many others fall into milder or moderate categories where a thoughtful, physician-guided conservative program is the mainstay of care, and where surgery is neither recommended nor necessary at this time.
At Lavender Family Chiropractic in Sarasota, Florida, we work with people navigating this exact uncertainty. We are an upper cervical practice, which means we focus on the alignment relationship at the very top of the neck, where the head balances on the atlas and axis vertebrae. We use a precise, low-force method called the Knee Chest Upper Cervical technique, and we lean on objective tools such as 3D CBCT imaging and Tytron paraspinal infrared thermography to understand what is happening in your individual case. But we want to be very clear from the beginning: upper cervical care does not repair ligaments, it is not a substitute for a medical evaluation, and it should never replace the guidance of a physician or specialist when instability is significant. Our role, when it is appropriate at all, is to be one supportive, conservative option within a larger team.
This article is written to help you understand the landscape. We will walk through when surgery is genuinely considered versus when conservative care leads the way, what the recognized non-surgical options actually are, where careful upper cervical care may or may not fit, why the upper neck matters so much anatomically, and what the current research says. Our goal is not to convince you of anything. It is to give you clear, honest information so you can make good decisions with your medical team. If severe or progressive neurological symptoms are part of your picture, please treat that as urgent and seek immediate medical evaluation. Nothing in this article is a reason to delay that.
When Is Surgery Considered vs. Conservative Care?
Craniocervical instability is, at its core, a problem of too much motion or insufficient support at the junction where the skull meets the spine. The ligaments and structures that normally hold the head steady on the upper neck are, in some individuals, lax, injured, or genetically less robust. This is especially relevant for people living with heritable connective tissue disorders such as the Ehlers-Danlos syndromes (EDS), where ligament laxity is part of the underlying biology. It can also follow significant trauma. Because the range of severity is so wide, the decision between surgery and conservative management is highly individualized and belongs in the hands of physicians who can weigh imaging, neurological findings, and how symptoms are changing over time.
Surgery for craniocervical instability generally means occipito-cervical fusion, a procedure that stabilizes the skull to the upper cervical spine using hardware and bone grafting. It is a major operation, and precisely because it is major and irreversible, it is reserved for a specific subset of patients: those with severe, objectively documented instability, those with clear evidence of brainstem or spinal cord compression, and those with progressive neurological deficits that are not responding to conservative measures. When a surgeon recommends fusion, it is typically because the instability is threatening critical neurological structures and the risk of doing nothing outweighs the substantial risks of the operation. In the connective tissue disorder population, published surgical series describe meaningful symptom improvement in carefully selected patients, but they also underscore how important patient selection and thorough documentation are before anyone proceeds to the operating room.
Conservative care, by contrast, is the appropriate first path for a large number of people, particularly those with milder instability, without red-flag neurological findings, and whose symptoms are stable rather than rapidly worsening. Conservative management does not “cure” instability and does not repair damaged ligaments, but it can help many people manage symptoms, protect the region, improve muscular support, and maintain function while being monitored over time. It is important to understand that conservative management for CCI is typically physician-guided. This is not a do-it-yourself situation, and it is not something to improvise from social media videos. A physiatrist, neurosurgeon, neurologist, or other qualified physician usually oversees the plan, orders and interprets the appropriate imaging, and decides whether and when a surgical opinion is warranted.
So how do the two paths relate? Think of them as a continuum rather than an either/or. Most patients begin with conservative measures. A minority, based on the severity of their instability and their neurological status, move toward surgical evaluation. And there are people for whom conservative care is used to manage symptoms while a surgical decision is being weighed carefully over months. The key point, and one we return to often at our Sarasota practice, is that no honest provider can promise you that any conservative approach, including precise upper cervical care, will prevent surgery or reverse instability. What a good team can do is help you pursue reasonable, lower-risk options first, monitor you responsibly, and make sure that if surgery ever does become necessary, the decision is made with clear eyes and good information.
Conservative / Non-Surgical Options
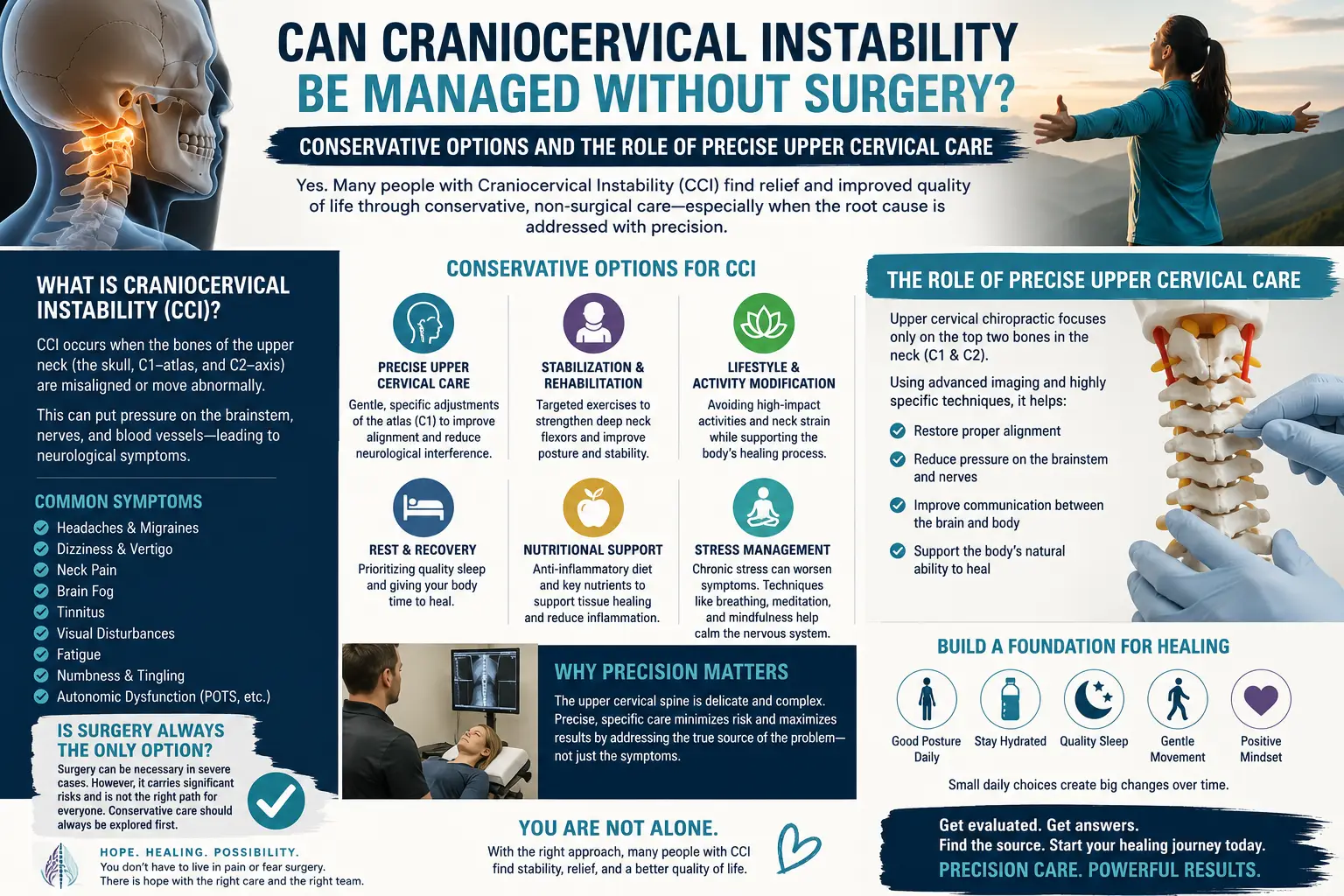
When people ask whether craniocervical instability can be managed without surgery, they are usually asking about this category: the collection of conservative, non-operative strategies that physicians and rehabilitation professionals use to help patients feel more stable and function better. None of these approaches repairs ligaments or reverses the underlying instability, but together they can form a meaningful management plan for appropriate patients. Here are the main pillars, all of which are best coordinated with your physician.
Activity modification. One of the simplest and most powerful tools is changing how you move through your day. That means learning which positions and movements provoke your symptoms and adjusting accordingly. For many people with upper cervical instability, prolonged forward head posture, heavy lifting, sudden or extreme neck movements, high-impact activities, and certain sleeping positions can aggravate the region. Modifying these does not fix the underlying laxity, but it reduces the repeated provocation that drives symptom flares. Learning to keep the head reasonably supported and balanced over the shoulders, taking breaks from screens, and being deliberate about transitions like getting out of bed can all matter.
Targeted, physician-guided strengthening of the deep neck and postural muscles. When the passive stabilizers of the neck (the ligaments) are compromised, the active stabilizers (the muscles) take on a larger share of the work. This is why carefully prescribed strengthening of the deep cervical flexors and the deep postural muscles of the neck and upper back is a cornerstone of conservative management. The idea is to improve the muscular support and the body’s position sense around a region that has lost some of its passive stability. This work must be done gently, progressively, and under professional supervision, because aggressive or poorly chosen exercises can aggravate an unstable segment. When it is guided appropriately by a physical therapist or physician, this kind of graded strengthening and proprioceptive retraining is one of the most evidence-supported components of non-surgical neck care.
Cervical collars and bracing, in some cases. For selected patients, particularly during acute flares or specific high-risk activities, a physician may recommend a cervical collar or brace to provide temporary external support. This is a nuanced decision. Bracing can offer relief and protection in the short term, but long-term or unnecessary reliance on a collar can lead to deconditioning of the very muscles you are trying to strengthen. That is exactly why this belongs with your physician rather than something to purchase and self-prescribe. When and how to use bracing is a clinical judgment based on your individual situation.
Symptom and autonomic management. Craniocervical instability can be associated with a broad constellation of symptoms, including headaches, dizziness, visual disturbances, difficulty concentrating, and features that overlap with autonomic nervous system dysregulation such as dysautonomia. Managing these symptoms is part of comprehensive conservative care. That can involve hydration and lifestyle strategies, addressing sleep, pacing activity, and sometimes medications or other interventions directed by a physician. Because the upper neck sits so close to the brainstem and the structures that help regulate autonomic function, symptom management in CCI is often multidisciplinary.
Avoiding provocative positions and aggressive self-cracking. This point deserves emphasis. People with neck symptoms often develop a habit of forcefully self-manipulating or “cracking” their own necks for temporary relief, and others seek out high-velocity twisting manipulation. For someone with actual or suspected craniocervical instability, forceful, high-velocity, end-range twisting of the neck is exactly the kind of provocation that a careful plan seeks to avoid. This is one of the reasons the distinction between forceful manipulation and precise, low-force upper cervical work matters so much, and we will return to it below. If you have suspected instability, please resist the urge to crack your own neck, and be cautious about any provider who wants to apply forceful rotational thrusts to your upper cervical spine.
Taken together, these conservative options represent a reasonable, lower-risk starting point for many people, especially those without red-flag neurological findings. They are not a guarantee of anything, and they are not a cure. But for appropriate patients, coordinated conservative care can be a genuinely helpful way to manage symptoms and support daily function while being monitored over time.
Where Precise Upper Cervical Care Fits
This is the part where we have to be especially careful and especially honest, because it is our own field, and because craniocervical instability is a serious topic. Let us start with what upper cervical care is not. It is not a repair for damaged or lax ligaments. It is not a substitute for a medical evaluation. It is not a treatment that reverses instability, and it is not a reason to skip or delay a needed surgical opinion. Anyone who tells you that a chiropractic approach can cure craniocervical instability or restore its lost stability is not being straight with you. We will not make that claim, because it is not true.
So what is the potential role? At Lavender Family Chiropractic, our focus is alignment at the top of the neck, the relationship between the head, the atlas (C1), and the axis (C2). Our method, the Knee Chest Upper Cervical technique, is a precise, low-force approach. This is a critical distinction. We do not perform high-velocity, twisting “manipulation” of the neck. Our correction is specific, gentle, and directed by objective measurements rather than by force. For a topic as sensitive as upper cervical instability, that difference between forceful rotational thrusting and a precise, low-force correction is not a marketing nuance; it is central to how we practice and to why we take a conservative, coordinated approach.
Objectivity is the foundation of what we do. Before any care is even considered, we want to understand your individual structure and physiology. We use 3D CBCT imaging, a cone-beam computed tomography technology that lets us view the upper cervical anatomy in three dimensions with fine detail. We also use Tytron paraspinal infrared thermography, a non-contact scan that measures patterns of heat along the spine as a window into how the nervous system is functioning. These tools help us decide whether upper cervical care is even appropriate for you, and they help us communicate clearly with your medical team. Importantly, our imaging is not a diagnostic substitute for the specialized flexion-extension studies, upright MRI, or other advanced instability workups that physicians use to formally evaluate CCI. When we see findings that suggest significant instability or that fall outside the scope of conservative chiropractic care, our job is to say so and to refer you appropriately.
Here is how we think about where we fit. For a patient with mild upper cervical dysfunction, no red-flag neurological findings, and a physician who is aware of and comfortable with a conservative plan, precise low-force alignment care may be one supportive component of a broader conservative strategy, alongside the physician-guided activity modification, strengthening, and symptom management described earlier. We build customized care plans around your specific situation rather than applying a one-size-fits-all protocol, and we coordinate with your medical team rather than working in isolation. You can learn more about our overall approach on our upper cervical chiropractic care page.
And here is the boundary, stated plainly. We cannot and do not promise that our care will help you avoid surgery, prevent progression, or reverse instability. For patients with severe, well-documented instability, progressive neurological symptoms, or connective tissue disorders driving significant laxity, the appropriate path runs through their physicians and surgeons, and our role is limited or may not be appropriate at all. Precise upper cervical care is a conservative, supportive option for the right person in the right context, coordinated with medical care. That is the honest scope, and we would rather be trusted for telling you the truth than be chosen for overpromising.
Why the Upper Neck (Atlas/Axis) Matters
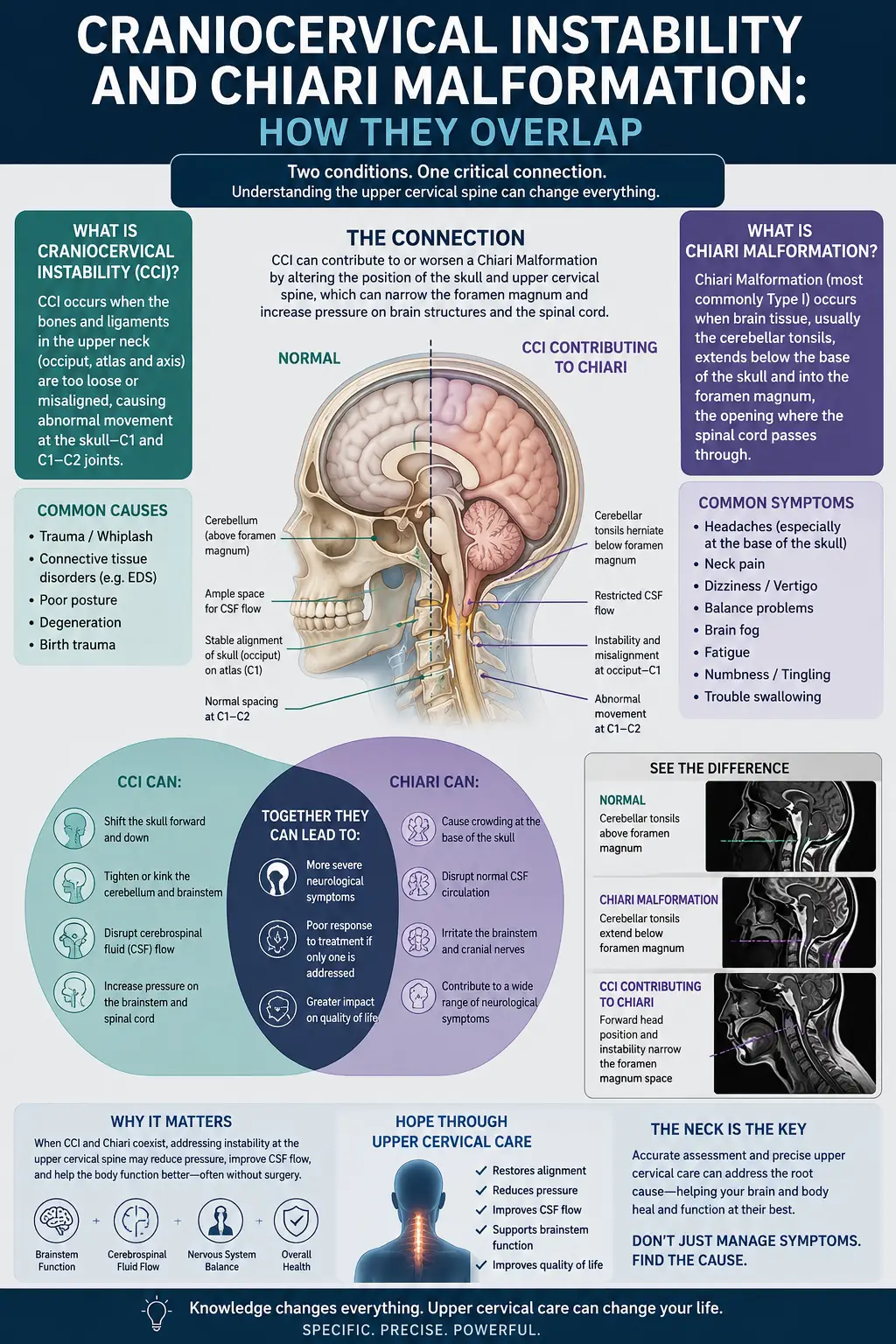
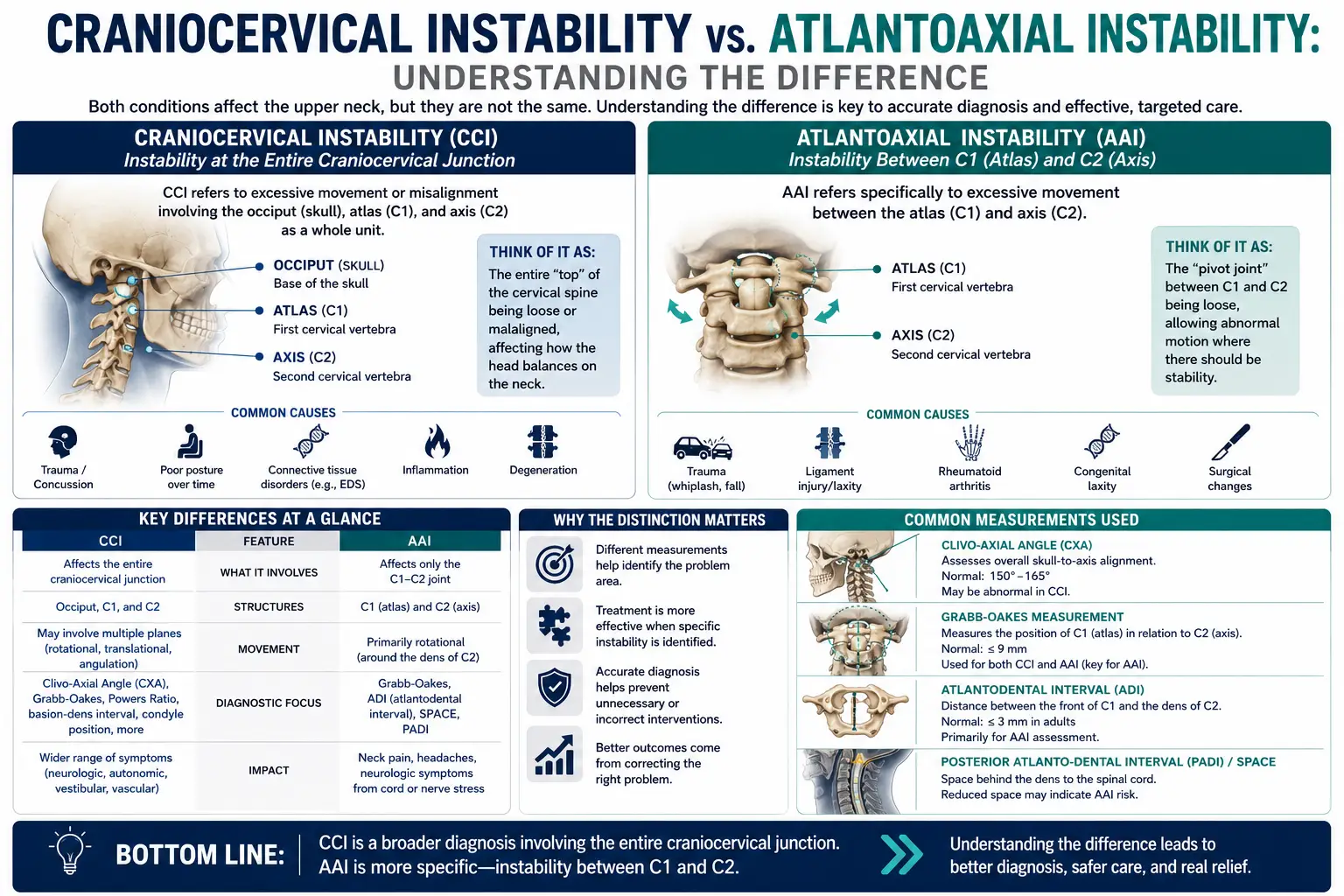
To understand why the top of the neck receives so much attention in conversations about craniocervical instability, it helps to appreciate the anatomy. The junction where the skull meets the spine is one of the most remarkable and vulnerable regions in the human body. The first cervical vertebra, the atlas (C1), is a ring-shaped bone that cradles the base of the skull and allows you to nod your head. The second vertebra, the axis (C2), features a bony peg called the dens, or odontoid process, around which the atlas rotates, allowing you to turn your head side to side. This design gives the head an extraordinary range of motion, which is wonderful for function but also means the region relies heavily on soft tissue for stability.
That stability comes primarily from a network of ligaments rather than from interlocking bone. Structures such as the transverse ligament, the alar ligaments, the tectorial membrane, and the surrounding capsular tissues hold the head steady on the upper spine and prevent excessive movement of the dens toward the brainstem and spinal cord. When these ligaments are lax, stretched, injured, or genetically less robust, as in heritable connective tissue disorders, the passive stability of the region can be compromised. That is the essence of craniocervical instability: the soft tissue restraints that should keep the head steady on the neck are not doing their job fully, and excessive motion results.
The stakes are high in this region because of what lies within and just beyond it. The brainstem, the transition into the spinal cord, the vertebral arteries, and critical cranial nerve pathways all pass through or near the craniocervical junction. This is why symptoms of upper cervical problems can be so wide-ranging and sometimes so strange: headaches at the base of the skull, a sensation that the head is too heavy to hold up, dizziness and vertigo, visual changes, difficulty swallowing, cognitive fog, and autonomic symptoms can all trace back to this area. It is also why significant instability is taken so seriously by physicians, and why progressive neurological signs are treated as urgent.
From an alignment standpoint, our interest at Lavender Family Chiropractic is in how well the head is balanced over the atlas and axis, and whether a precise, low-force correction can support better positioning and function in appropriate patients. We are not claiming to tighten ligaments or to restore lost passive stability. Ligaments are not something a chiropractic correction repairs. What we can do, for the right person, is focus carefully on the alignment relationship at this pivotal junction, measured objectively, and offer that as one conservative, supportive piece of a coordinated plan. Understanding the anatomy makes both the promise and the limits clearer: the upper neck matters enormously, which is exactly why it must be approached with precision, humility, and medical coordination.
Ready to Talk Through Your Situation?
If you are in Sarasota or the surrounding area and want a careful, honest conversation about whether precise upper cervical care might have a supportive role in your situation, we are here to help you think it through, not to oversell you. Call Lavender Family Chiropractic at (941) 243-3729, or book a new patient visit online. Our office is located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, at the corner of University and Whitfield. We will take the time to understand your history, review your objective findings, and be direct with you about what is and is not within the scope of conservative upper cervical care, including when we believe you should be working with a physician or specialist.
What the Research Says
We believe in pointing you toward the actual literature rather than asking you to take our word for anything. The research on craniocervical instability spans both surgical criteria and conservative rehabilitation, and reading across it helps explain why the surgery-versus-conservative decision is so individualized. Here are five peer-reviewed sources, described accurately.
- In a systematic review published in Global Spine Journal, Craniocervical Instability in Ehlers-Danlos Syndrome—A Systematic Review of Diagnostic and Surgical Treatment Criteria, the authors examine how CCI is diagnosed and when surgery is considered in patients with EDS. They highlight a genuine lack of consensus on imaging parameters and surgical indications, which underscores why careful, individualized decision-making with experienced physicians is so essential before proceeding to fusion.
- The study Cervical medullary syndrome secondary to craniocervical instability and ventral brainstem compression in hereditary hypermobility connective tissue disorders: 5-year follow-up after craniocervical reduction, fusion, and stabilization follows a carefully selected group of patients with connective tissue disorders and documented instability who underwent occipito-cervical fusion. It reports meaningful symptom improvement in this specific surgical population, illustrating both the potential value of surgery and how selective the criteria for it are.
- The review Anatomic, functional, and radiographic review of the ligaments of the craniocervical junction details the ligamentous anatomy that provides stability at the skull-neck junction, including the tectorial membrane, cruciform ligament, and alar and apical ligaments. It explains how injury to these structures can produce instability, reinforcing why this passive stability cannot simply be restored by any conservative treatment.
- The systematic review Effects of deep cervical flexor training on impaired physiological functions associated with chronic neck pain synthesizes randomized trials on training the deep stabilizing muscles of the neck. It supports the role of targeted, progressive strengthening of the deep neck flexors as a component of conservative neck care, which aligns with the physician-guided rehabilitation described earlier.
- The preliminary randomized clinical trial Effects of Two Exercise Programs on Neck Proprioception in Patients with Chronic Neck Pain compares exercise approaches aimed at improving neck position sense in people with chronic neck pain. It illustrates that proprioceptive and stabilization exercise can measurably influence how well the neck senses and controls its own position, which is exactly the kind of conservative, active support that matters when passive stability is compromised.
A note on interpretation: none of these studies suggests that a chiropractic correction repairs ligaments or reverses instability, and we do not present them that way. The surgical papers frame when an operation is genuinely warranted, the anatomy review explains why passive stability is a soft-tissue matter, and the rehabilitation studies support the active, conservative measures that make up so much of non-surgical management. Read together, they paint a picture of individualized, team-based care.
Daily Life and Self-Care Strategies
Beyond formal treatment, the way you live day to day can meaningfully influence how you feel when you are managing upper cervical symptoms. These strategies are general, supportive habits, not medical treatment, and if you have suspected or confirmed instability you should run any new routine by your physician first. With that said, here are approaches many patients find helpful.
Mind your posture, gently. Prolonged forward head posture places extra demand on an already sensitive region. Rather than forcing a rigid “perfect” posture, aim for frequent, easy resets: bring your head back over your shoulders, relax your jaw and shoulders, and change positions often. If you work at a desk, set your screen at eye level and take short breaks to avoid long stretches of looking down.
Support your head during sleep. Sleep position matters a great deal for the upper neck. Many people do best with a supportive pillow that keeps the neck in a neutral position rather than propped too high or too flat. Back and side sleeping are generally gentler on the upper cervical region than sleeping on the stomach, which tends to force the neck into rotation. Experiment carefully, and if a position provokes symptoms, avoid it.
Move deliberately, not forcefully. Sudden, jerky, or end-range neck movements can provoke symptoms in a sensitive upper neck. Turn your whole body rather than wrenching your head to look behind you, ease into and out of bed, and steer clear of high-impact or whiplash-risk activities without medical clearance. Above all, resist the temptation to forcefully crack your own neck, which is exactly the kind of provocation careful management seeks to avoid.
Manage the whole system. Hydration, steady sleep, stress regulation, and gentle pacing of activity can all influence symptoms, particularly when autonomic features like dizziness or brain fog are part of your picture. Simple nervous-system-friendly habits, breathing slowly, avoiding rapid position changes that trigger lightheadedness, and not pushing through severe symptoms, are reasonable supports.
Stay connected to your care team. Keep a simple log of your symptoms, note what provokes and relieves them, and share changes with your physician, especially anything that is new, worsening, or neurological. This kind of tracking helps your team make good decisions with you over time.
If you would like to go deeper on related topics, our article on neck pain offers additional context on how upper cervical alignment relates to persistent neck symptoms and how we approach evaluation and care. And if the sensation that your head feels too heavy to hold up resonates with you, our discussion of craniocervical instability and the heavy-head, vertigo experience explores that specific pattern in more detail.
Serving Sarasota and Surrounding Communities
Lavender Family Chiropractic is proud to serve patients from across the Suncoast and beyond. Our office sits at the corner of University and Whitfield, making us convenient to a wide swath of the region. We regularly welcome people traveling from Sarasota, Bradenton, Lakewood Ranch, Venice, Palmer Ranch, Osprey, Siesta Key, Longboat Key, Lido Key, University Park, Parrish, Ellenton, Myakka City, Punta Gorda, and St. Petersburg. Because our care is precise and individualized, and because upper cervical concerns often prompt people to seek out specialized attention, we frequently see patients who are willing to drive a bit farther for a thoughtful, objective, and honest approach. Wherever you are coming from on Florida’s Gulf Coast, we aim to make your experience clear, unhurried, and coordinated with the rest of your health care.
Top 15 Questions
1. Can craniocervical instability be managed without surgery? For many people, especially those with milder instability and no red-flag neurological findings, conservative, non-surgical management is the appropriate first path. It does not cure or reverse instability, but physician-guided activity modification, targeted strengthening, symptom management, and sometimes bracing can help many patients manage symptoms and function. Severe, progressive, or well-documented cases may still require surgical evaluation.
2. Will precise upper cervical care help me avoid surgery? We cannot promise that, and we will not. No honest provider can guarantee that any conservative approach will prevent surgery or reverse instability. What we can offer, for appropriate patients, is one supportive, conservative, low-force option coordinated with your medical team. Whether surgery is ever needed is a decision that belongs with your physicians, based on your imaging and neurological status.
3. Can you cure craniocervical instability? No. Upper cervical care does not cure craniocervical instability and does not repair or tighten ligaments. It is not a substitute for medical evaluation. Our focus is on precise, low-force alignment support at the top of the neck as one conservative piece of a broader, physician-coordinated plan, and we are always honest about those limits.
4. What symptoms suggest I should seek urgent medical care? Severe or progressive neurological symptoms are red flags. These can include worsening weakness or numbness in the arms or legs, problems with balance or walking, difficulty swallowing or speaking, loss of bladder or bowel control, severe or rapidly worsening headache, fainting, or new visual changes. If you experience symptoms like these, do not wait for a chiropractic visit; seek immediate medical or emergency care.
5. Is your correction the same as forceful neck “cracking”? No. We use the Knee Chest Upper Cervical technique, a precise, low-force correction. We do not perform high-velocity, twisting manipulation of the neck. For a sensitive topic like upper cervical instability, that distinction matters, and we would also caution you against forcefully cracking your own neck.
6. How do you decide whether upper cervical care is even appropriate for me? We start with objective assessment, including 3D CBCT imaging and Tytron paraspinal infrared thermography, along with a careful history. These help us understand your individual structure and function, decide whether care is appropriate, and identify findings that call for medical referral instead.
7. Do you work with my physician or specialist? Yes. We view precise upper cervical care as one conservative option within a coordinated team, not as a replacement for medical care. When instability is significant or symptoms are progressive, we refer and coordinate with physicians, and we can provide documentation to support that communication.
8. What conservative options do physicians typically use for CCI? Common physician-guided measures include activity modification, targeted strengthening of the deep neck and postural muscles, cervical collars or bracing in select cases, and symptom and autonomic management. These are usually overseen by a physiatrist, neurologist, neurosurgeon, or similar specialist.
9. I have Ehlers-Danlos syndrome. Is my situation different? It can be. Heritable connective tissue disorders such as EDS involve ligament laxity that can drive instability, and this population is discussed heavily in the surgical literature. If you have EDS or a related disorder, your care should be closely guided by physicians experienced with these conditions, and any conservative measures should be coordinated with them.
10. Does your imaging diagnose craniocervical instability? Our 3D CBCT imaging gives us detailed three-dimensional views of the upper cervical anatomy that guide our alignment focus, but it is not a substitute for the specialized instability workups physicians use, such as dynamic flexion-extension studies or upright MRI. When formal instability evaluation is needed, that belongs with your medical team.
11. Are you in-network with my insurance? We are a cash-pay, out-of-network practice. That means we are not contracted with insurance networks, which allows us to spend our time and attention on individualized care rather than on network constraints.
12. Can I still use my insurance benefits at all? We provide superbills, which are detailed receipts you can submit to your insurance company for possible out-of-network reimbursement, depending on your individual plan. We cannot guarantee reimbursement, since that is determined by your insurer, but many patients choose to submit superbills to seek partial reimbursement.
13. How are your care plans structured and priced? We build customized care plans based on your specific findings and goals rather than a generic protocol. We will explain your options and associated costs transparently before you commit to anything, so you can make an informed decision that fits your situation and budget.
14. Is precise, low-force upper cervical care risky for someone with instability? Our approach is precise and low-force by design, which is very different from forceful, high-velocity rotational manipulation. That said, for anyone with suspected or confirmed instability, care decisions must be made carefully and in coordination with your physician. If your situation falls outside the appropriate scope of conservative chiropractic care, we will tell you and refer you.
15. What should I do first if I suspect I have CCI? Start with a proper medical evaluation, especially if you have any neurological symptoms. A physician can order appropriate imaging and determine the severity of your situation. From there, a conservative plan may be built, and precise upper cervical care can be discussed as one possible supportive component where appropriate. If you would like an honest conversation about that, call us at (941) 243-3729 — we are glad to help you think it through.
Closing CTA
Craniocervical instability is a serious, individual, and often frightening topic, and you deserve straight answers as you navigate it. The honest summary is this: many milder cases are managed conservatively, some severe or progressive cases require surgical evaluation, and precise upper cervical care is, at most, one supportive conservative option for appropriate patients, coordinated with your medical team. It does not repair ligaments, reverse instability, or replace a medical evaluation, and severe or progressive neurological symptoms always warrant urgent medical attention.
If you would like a careful, no-pressure conversation about where you stand and whether our approach might have a supportive role, we would be honored to help. Call Lavender Family Chiropractic at (941) 243-3729, or schedule your visit online. You can also reach us through our contact page. Our office is at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, at the corner of University and Whitfield. Whether you are coming from Sarasota, Bradenton, Lakewood Ranch, Venice, or anywhere along the Gulf Coast, we look forward to giving you clear, honest information you can use with your care team. And if your symptoms are severe or worsening, please seek immediate medical care first, then let us know how we can support you afterward.
Related Articles
- Craniocervical Instability: The Complete Guide — Start here. Our comprehensive pillar resource on craniocervical instability covers what CCI is, how it is evaluated, the range of symptoms, and how conservative and medical care fit together. If you read only one companion article to this one, make it this pillar guide.
- Neck Pain — How upper cervical alignment relates to persistent neck pain, and how we evaluate and approach it with precise, low-force care.
- When Your Head Feels Too Heavy: Craniocervical Instability and Vertigo — A closer look at the heavy-head sensation, dizziness, and vertigo that often accompany upper cervical concerns.