
Cervicogenic Dizziness: You stand up from the couch and the room takes an extra second to catch up. You turn your head to back out of the driveway and a wave of unsteadiness rolls through you. You spend an afternoon hunched over your laptop and by dinner the floor feels like it’s tilting. You wake up most mornings with a tight, achy neck and a foggy, off-balance feeling that follows you around for hours. Your MRI came back clean. Your inner ear test was “unremarkable.” Your blood work was perfect. And yet — you still feel like something is wrong.
If that sounds familiar, you are not imagining it. You may be dealing with a condition that millions of people live with, but very few doctors look for: cervicogenic dizziness. The word looks intimidating, but the meaning is simple. Cervico means neck. Genic means originating from. Dizziness, of course, means dizziness. Cervicogenic dizziness is dizziness, imbalance, and disorientation that comes from the neck — specifically the upper part of the neck, where the skull meets the spine.
At Lavender Family Chiropractic, located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — right at the corner of University and Whitfield — we see patients with cervicogenic dizziness every single week. They come to us from Sarasota, Bradenton, Lakewood Ranch, Parrish, Venice, Osprey, Siesta Key, Longboat Key, and beyond. They come from primary care offices, neurology consults, ENT specialists, physical therapy clinics, and emergency rooms. They come carrying folders of normal scans and frustration that has been building for months or years. And in many of these cases, the answer was hiding in plain sight at the very top of their spine the entire time.
This guide is a complete, plain-English look at cervicogenic dizziness — what it is, what causes it, why it gets missed so often, how it connects to the upper neck, what the research actually says, and what you can do about it. If you have been searching for “dizziness doctor near me,” “chiropractor for vertigo Sarasota,” “upper cervical chiropractor near me,” or simply “why am I dizzy all the time,” this article is written for you.
What Is Cervicogenic Dizziness?
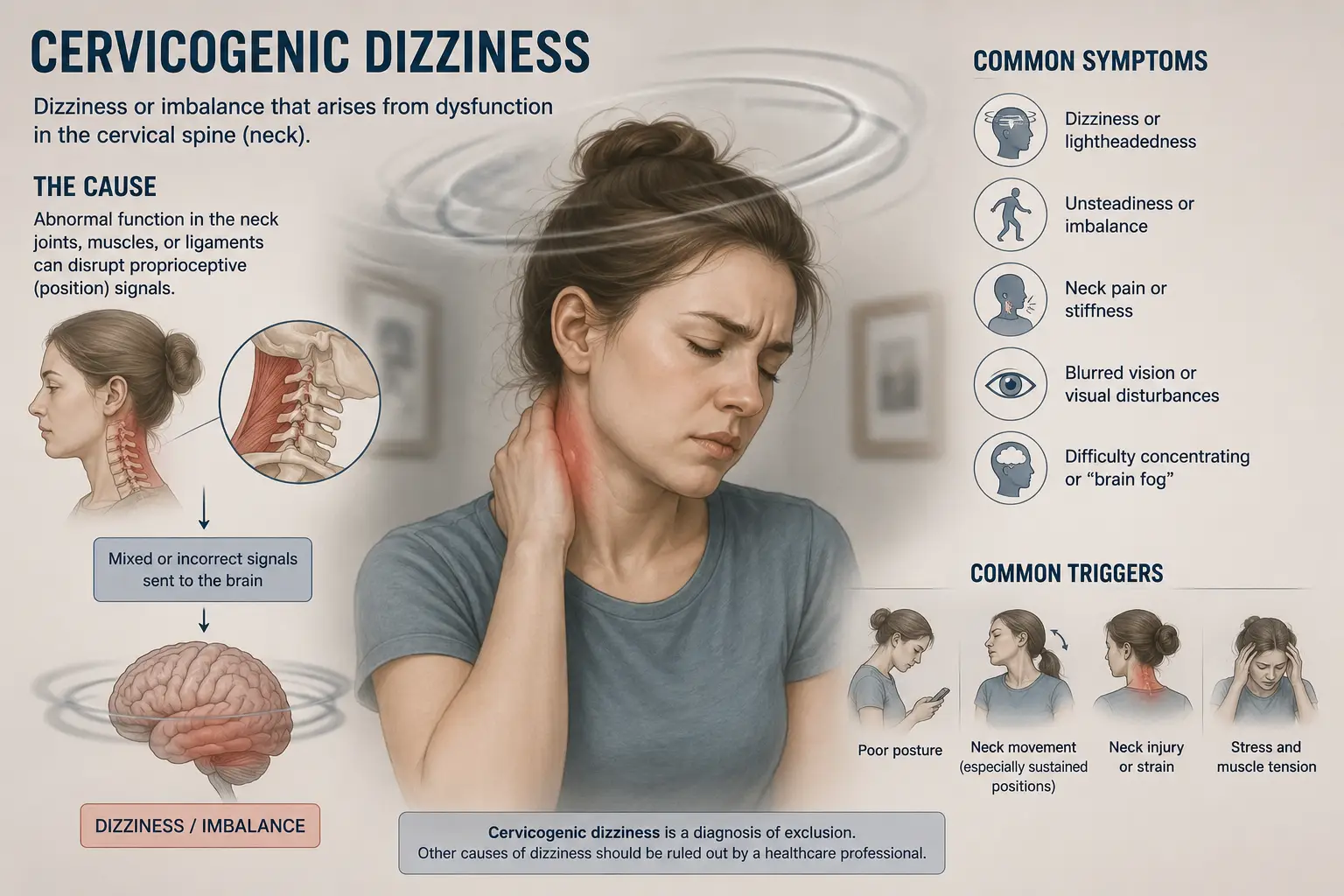
Cervicogenic dizziness is a condition in which faulty signals from the joints, muscles, and ligaments of the neck disrupt your sense of balance and spatial orientation. It typically shows up as a feeling of unsteadiness, lightheadedness, swaying, floating, or disorientation that is closely tied to neck pain, neck stiffness, or certain neck positions. Unlike true vertigo, where the room visibly spins, cervicogenic dizziness tends to feel more like the world is subtly off, like you are walking on a boat that is not quite still, or like your head is disconnected from your body. Symptoms usually last minutes to hours, often follow head or neck movements, and frequently improve when the neck pain improves.
Cervicogenic dizziness has also been called cervical vertigo, cervical dizziness, and proprioceptive vertigo. The modern medical literature has largely settled on cervicogenic dizziness because true spinning vertigo is not the dominant symptom in most cases. What you feel is more nuanced than the word “vertigo” captures. It is the sense that you are not quite in command of where your body ends and the room begins.
Cervicogenic dizziness is what doctors call a diagnosis of exclusion. That is a clinical way of saying there is no single test, scan, or lab value that proves you have it. Instead, your provider must carefully rule out other possible causes of dizziness — inner ear disorders, neurological conditions, cardiovascular issues, medication side effects, blood pressure problems, blood sugar swings — and then connect your remaining dizziness to clear, demonstrable dysfunction in your cervical spine. Because of this, many patients are bounced from specialist to specialist without ever getting a clear answer. They are told everything looks normal, even as their daily life shrinks around their symptoms.
That gap — where the testing ends and the suffering continues — is exactly where upper cervical chiropractic care fits.
How the Neck Talks to Your Balance System
To understand cervicogenic dizziness, you first have to understand how your balance system actually works. Most people assume balance lives in the inner ear. The inner ear is part of the story, but only part. Your sense of balance is the product of three streams of information that your brain constantly weighs against each other.
The first stream is visual. Your eyes tell your brain what is up, what is down, what is moving, and what is still. The second stream is vestibular. The semicircular canals and otolith organs of your inner ear sense head motion, head tilt, and acceleration. The third stream — and the one most people have never heard of — is cervical proprioception. The joints, muscles, ligaments, and tendons of your neck are packed with tiny sensors called mechanoreceptors. These sensors are constantly sending position and movement data to your brainstem. They tell your brain, in real time, where your head is in relation to your body, how fast your head is moving, and which way it is turning.
The upper cervical spine — the atlas (C1) and axis (C2) — is one of the most densely innervated regions of your entire body. The little muscles at the base of your skull, especially the suboccipital muscles, have a higher concentration of muscle spindles per gram of tissue than almost any other muscle in the human body. That is not an accident. Evolution wired your upper neck to be exquisitely sensitive because your brain absolutely needs to know where your head is at every moment.
When the upper cervical spine is functioning normally, all three streams — vision, vestibular, and cervical proprioception — agree with each other, and your brain produces a smooth, confident sense of orientation. When the upper cervical spine is not functioning normally, the cervical stream starts to send distorted, mismatched, or “noisy” signals. Your eyes say one thing. Your inner ear says another. Your neck says a third. Your brain cannot reconcile them, and the result is dizziness, unsteadiness, brain fog, visual sensitivity, and a feeling of being unmoored from the ground.
This sensory mismatch is the most widely accepted explanation for cervicogenic dizziness in the current research. Faulty cervical input feeds into the vestibular nuclei in the brainstem, into the cerebellum, and into the higher cortical regions that build your sense of spatial awareness. Even a small disruption at the top of the neck can ripple out into a much larger experience of imbalance.
The Upper Cervical Connection: Why C1 and C2 Are the Center of the Story
The upper cervical spine is unlike any other part of your skeleton. The atlas (C1) is a ring-shaped vertebra that cradles your skull. The axis (C2) sits beneath it and provides the pivot point that allows your head to rotate. Together, these two bones produce roughly half of all the rotation your neck can perform, while also protecting the most neurologically dense piece of real estate in your entire body — the brainstem and the upper spinal cord.
When the atlas and axis are aligned properly, the brainstem sits comfortably in its protective tunnel, blood flow through the vertebral arteries is unobstructed, cerebrospinal fluid drains freely, and the dense bed of proprioceptive sensors at the top of the neck sends clean, accurate signals to the brain. When the atlas or axis is misaligned — even by a fraction of a millimeter — several things can begin to go wrong at once.
First, the proprioceptive sensors in the upper neck begin to misfire. Tiny shifts in joint position translate into chronically distorted input, and the brain spends every waking minute trying to make sense of contradictory data. Second, the small muscles of the suboccipital region — the rectus capitis posterior major and minor, the obliquus capitis superior and inferior — become tight, guarded, and dysfunctional. These muscles are not only mechanically important; they are sensorially critical, and when they go into spasm, they generate a constant stream of noisy signals that the brain interprets as imbalance.
Third, the vertebral arteries, which thread up through small openings in the cervical vertebrae and supply blood to the brainstem and cerebellum, can experience altered flow dynamics. Fourth, the dural attachments between the upper cervical spine and the brainstem — including the small but important myodural bridges — can transmit mechanical tension upward into the membranes that surround your brain.
Add all of this together, and you have a system that is exquisitely vulnerable to disruption from a single area: the top two bones of your neck. This is why patients with whiplash, sports concussions, falls onto the head or tailbone, long-term forward head posture, motor vehicle accidents, or even traumatic births often develop dizziness symptoms that have nothing to do with their inner ear. The injury did not damage the vestibular apparatus. It scrambled the cervical input that the vestibular apparatus depends on.
Common Symptoms of Cervicogenic Dizziness
Cervicogenic dizziness can look different from person to person, but there are recognizable patterns. The most common complaints we hear at our Sarasota office include a constant or recurring sense of unsteadiness, swaying, or floating; lightheadedness that worsens when the neck is held in one position for too long; disorientation triggered by quick head turns, looking up, looking down, or driving; a feeling of being off-balance that follows or accompanies neck pain or stiffness; tension headaches or occipital headaches at the base of the skull; visual sensitivity in busy environments like grocery stores or crowded restaurants; difficulty focusing the eyes after head movement; brain fog and trouble concentrating; nausea without true spinning; fatigue from the constant effort of staying upright; and a worsening of symptoms with stress, poor sleep, or screen-heavy days.
A telltale feature of cervicogenic dizziness is that the dizziness and the neck symptoms tend to rise and fall together. When the neck is worse, the dizziness is worse. When the neck eases, the dizziness eases. Unlike benign paroxysmal positional vertigo, which produces brief, intense spinning when the head is moved into specific positions, cervicogenic dizziness is typically more diffuse, more persistent, and more closely tied to overall neck mechanics. Unlike Meniere’s disease, it does not cause hearing loss or ear fullness. Unlike vestibular neuritis, it does not produce dramatic spinning that lasts for days. Unlike persistent postural-perceptual dizziness, it is not primarily triggered by complex visual environments — although the two conditions can absolutely coexist and often do.
If you would like a deeper look at how the upper neck overlaps with persistent dizziness and visual sensitivity, our recent post The World Won’t Stop Spinning: PPPD, Persistent Dizziness, Sensory Overload, and Why the Answer May Be in Your Upper Neck explores that overlap in detail.
What Causes Cervicogenic Dizziness?
Cervicogenic dizziness almost always traces back to something that disrupted the normal mechanics of the upper cervical spine. The most common cause is trauma. Motor vehicle accidents, even low-speed rear-end collisions, are notorious for producing whiplash injuries that shift the atlas and axis subtly out of position. The dizziness may not appear immediately. Many patients report that the unsteadiness developed weeks, months, or even years after the original accident, often after a second, smaller stressor finally pushed the system over the edge.
Sports injuries are another major contributor. Football, hockey, soccer, gymnastics, equestrian sports, martial arts, cheerleading, and competitive cycling all carry significant risk of head and neck injury. Even a single concussion can leave upper cervical dysfunction in its wake — and post-concussion dizziness that lingers for months is very often cervicogenic in origin, even when imaging looks normal. Falls, especially falls onto the head, tailbone, or outstretched arms, can do the same. So can blunt trauma from hitting your head on a cabinet, a low doorway, or the bottom of a swimming pool.
Beyond clear traumatic events, there are slower, more cumulative causes. Forward head posture from long days at a computer or phone gradually adds load to the upper cervical region. Sleeping on a poor pillow night after night locks the suboccipital muscles into shortened positions. Chronic stress drives constant tension into the neck. Old, half-healed injuries from childhood — playground falls, bicycle wrecks, sports collisions long since forgotten — can leave residual misalignment that becomes symptomatic later in life when another stressor is added.
Surgical and dental events can play a role too. Long dental procedures with the head extended back, intubation for surgery, or prolonged time in an awkward position can all stress the upper cervical region. Hereditary factors such as connective tissue laxity, hypermobility, and Ehlers-Danlos syndrome can predispose a person to upper cervical instability and chronic dizziness.
Cervicogenic dizziness also frequently coexists with other vestibular and neurological conditions. It can ride alongside vestibular migraine, post-concussion syndrome, Mal de Débarquement Syndrome, BPPV, and dysautonomia. Treating one without addressing the other often produces only partial relief, which is part of why so many patients bounce between providers without ever feeling fully better.
How Cervicogenic Dizziness Is Diagnosed
Because there is no single test that proves cervicogenic dizziness, the diagnostic process relies on careful history-taking and the systematic elimination of other causes. A thorough workup typically includes a full medical and trauma history; an inner ear examination including tests like the Dix-Hallpike maneuver and head impulse test; a neurological exam to check coordination, eye movements, reflexes, and cranial nerve function; imaging when indicated; and a hands-on assessment of the cervical spine looking for restricted motion, joint tenderness, muscle guarding, and altered proprioception.
Several findings increase the likelihood that dizziness is cervicogenic in origin. Dizziness that begins or worsens with neck movement. Dizziness that is preceded by, accompanies, or fluctuates with neck pain. A history of head or neck trauma. Absence of true rotational vertigo with clear nystagmus. Normal inner ear and neurological findings. Demonstrable upper cervical joint dysfunction and asymmetry on examination. When these pieces line up, the diagnosis of cervicogenic dizziness becomes much more confident.
At Lavender Family Chiropractic, we take this process a step further. Many providers stop at the standard neurological and vestibular exam. We add advanced imaging and objective nervous system measurement so that we can see, rather than guess at, what is happening in your upper neck.
Upper Cervical Chiropractic Care at Lavender Family Chiropractic
Upper cervical chiropractic is a specialized branch of chiropractic that focuses almost entirely on the precise alignment of the atlas and axis. It is not the popping, twisting, cracking adjustment that most people picture when they hear the word “chiropractor.” It is a different discipline entirely, with its own analysis, its own imaging requirements, its own correction protocols, and its own measurable outcomes.
At our office, Dr. Rusty Lavender and Dr. Jacob Temple are both certified in the Advanced HIO Knee Chest Upper Cervical Technique, known as AHKC. This is one of the most precise and gentle forms of chiropractic care available. There is no twisting, no yanking, no popping, and no cracking. The correction is delivered while the patient is comfortable on a knee-chest table, using a small, specific contact at exactly the angle, depth, and direction that the imaging tells us is needed.
Before we ever attempt a correction, we build a complete picture of your upper cervical anatomy. We use 3D CBCT (cone beam computed tomography) imaging to capture your atlas and axis in three dimensions, down to a hundredth of a millimeter. We use paraspinal infrared thermography (Tytron scans) to objectively measure how your autonomic nervous system is functioning along your spine. We perform a detailed physical examination, posture analysis, and history review. Only then do we calculate the exact, individualized correction formula for your spine.
This level of precision matters. The upper cervical region is too important to guess at. A general adjustment delivered to the wrong joint, in the wrong direction, with the wrong vector, may produce a satisfying pop without correcting the underlying problem. A specific upper cervical correction, delivered to the right joint with the right vector, can release the proprioceptive logjam that has been driving your dizziness for months or years.
What to Expect at Your First Visit
If you have never been to an upper cervical office before, the experience is different from a standard chiropractic visit. Your first visit usually begins with a thorough consultation. We sit down with you and listen — really listen — to the full story of how your symptoms started, how they have changed, what makes them better, what makes them worse, what other providers have told you, and what you have already tried. We ask about old injuries that you may not have thought of in years, because the upper cervical spine has a long memory.
From there, we move to objective measurement. Posture analysis, range of motion testing, neurological screens, and the 3D CBCT scan and thermography scan happen on the first visit so that we have hard data to work from rather than impressions. On a follow-up report-of-findings visit, your doctor walks you through exactly what we found, what it means, whether we believe upper cervical care can help you, and what a care plan would look like if you choose to move forward. There is no high-pressure sales tactic and no scare tactics. You get clear information so you can make a clear decision.
When you receive your first correction, you will be surprised by how gentle it is. Most patients describe it as a light touch behind the ear with a quick, soft impulse. There is no sudden jerk, no audible crack, and very little sensation at all. After the correction, we have you rest for a period of time so that the nervous system can integrate the change. Many patients report a sense of warmth, relaxation, or subtle shift in their head position immediately afterward. Others feel changes gradually over the following days.
Ready to take the next step? You can book your complimentary consultation directly online at https://intake.chirohd.com/new-patient-scheduling/724/lavender-family-chiropractic. There is no obligation. We simply want to determine whether upper cervical care is a good fit for your situation, and if it is not, we will tell you that honestly and help point you in the right direction.
What the Research Says
Cervicogenic dizziness is a topic that has been actively studied for decades, and while the field still needs larger randomized controlled trials, the existing evidence is genuinely encouraging.
A foundational review published in the Journal of Orthopaedic and Sports Physical Therapy established cervicogenic dizziness as a real clinical entity characterized by dizziness and disequilibrium associated with neck pain in patients with cervical pathology. Subsequent narrative reviews have confirmed that manual therapy approaches targeting the cervical spine consistently reduce symptoms in this patient population.
A clinical study by L’Heureux-Lebeau and colleagues, published in 2014, demonstrated that cervical non-thrust techniques improve balance and proprioception in patients with cervicogenic dizziness. A randomized clinical trial published on ClinicalTrials.gov (NCT02772042) specifically examined the effectiveness of upper cervical traction manipulation in patients with cervicogenic dizziness and found that manual therapy targeting the upper cervical spine reduced symptoms in this population.
A retrospective case series published in 2023 in the Journal of Contemporary Chiropractic examined eight patients receiving upper cervical chiropractic care combined with individualized vestibular rehabilitation. The average improvement on the Dizziness Handicap Inventory was 67 percent over a thirty-day care period, and the protocol was reported as both safe and beneficial. A 2022 case report published in the Journal of Upper Cervical Chiropractic Research documented the complete resolution of cervicogenic dizziness and persistent upper cervical pain in a 49-year-old patient receiving Atlas Orthogonal upper cervical care after a traumatic fall.
A 2024 narrative review in the Journal of Upper Cervical Chiropractic Research examined atlas subluxation complex and dizziness improvement following specific upper cervical care, concluding that conceptual evidence, case reports, and theory provide a strong foundation suggesting that correction of atlas misalignment may produce favorable dizziness outcomes, and that further randomized trials are warranted.
The pattern across this literature is consistent. When the upper cervical spine is the source of the problem, addressing it with precise, evidence-informed care tends to help. Not every patient is a candidate, and not every patient responds equally, but the published improvement rates are real and meaningful.
Lifestyle Habits That Support Recovery
Care in our office is only one piece of the picture. What you do at home in between visits often determines how quickly and completely you recover. A few simple changes can dramatically support the upper cervical correction and the nervous system healing that follows it.
Sleep position matters more than most people realize. Sleeping on your back with a supportive cervical pillow, or on your side with a pillow that keeps your head level with your spine, protects your atlas-axis alignment. Stomach sleeping rotates the upper neck for hours at a time and is one of the most common posture habits we ask patients to change.
Screen ergonomics are critical. Bring your phone up to your eyes rather than dropping your eyes down to your phone. Raise your monitor so that the top of the screen sits at eye level. Take a posture break every twenty to thirty minutes. The cumulative load of forward head posture on a misaligned upper cervical spine is enormous.
Gentle daily movement helps the nervous system reorganize. Walking in nature, slow yoga, swimming, and balance work — like standing on one foot during routine tasks — all give your brain new, healthy proprioceptive input. Avoid aggressive neck stretching, especially deep rotation and extension, until your doctor clears you. Hydration, consistent sleep, and stress management all support nervous system recovery as well. The vagus nerve, which originates in the brainstem and is heavily influenced by upper cervical mechanics, responds beautifully to slow breathing, time outdoors, and reduced screen exposure.
If you have a history of motion sensitivity from cruises, flights, or long drives, you may find our recent post on Mal de Débarquement Syndrome useful as you sort out which of your symptoms belong to which condition. Many patients have more than one process going on at once, and untangling them is part of how we build a plan that works.
Serving Sarasota and the Surrounding Communities
Our office sits at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, at the corner of University and Whitfield. We are a short drive from neighborhoods all across the region, and patients travel to us from a wide circle of Florida communities. Locally, we serve Sarasota proper — including Desoto Lakes, Whitfield Estates, University Park, Palm Aire, Longwood Run, and the Bayshore Gardens area. We also see many patients from Bradenton, Lakewood Ranch, Parrish, Ellenton, Palmetto, Myakka City, Venice, Osprey, Nokomis, Siesta Key, Longboat Key, Lido Key, Anna Maria Island, and Holmes Beach. Patients regularly drive in from St. Petersburg, Tampa, Riverview, Ruskin, Punta Gorda, and Port Charlotte for care that they have not been able to find closer to home. If you would like a full list of the communities we serve, our Areas We Service page has the complete map.
Cervicogenic dizziness does not respect zip codes. Wherever you live, if you have been struggling with unexplained dizziness that has not responded to inner ear treatments, medications, vestibular rehab alone, or general chiropractic care, a precise look at your upper cervical spine may be the missing piece.
Top 15 FAQs About Cervicogenic Dizziness
1. What does cervicogenic dizziness feel like?
Most patients describe it as a constant or recurring feeling of unsteadiness, swaying, floating, or being slightly off-balance, rather than the dramatic spinning sensation of true vertigo. It often feels like walking on a boat that has not quite stopped moving, or like your head is disconnected from your body. The sensation is usually worse with certain neck positions, head turns, or after sustained postures like working at a computer.
2. How is cervicogenic dizziness different from vertigo?
True vertigo is the illusion that the room is spinning, and it is most commonly caused by inner ear conditions like benign paroxysmal positional vertigo (BPPV), Meniere’s disease, or vestibular neuritis. Cervicogenic dizziness is generated by the neck rather than the inner ear, tends to feel more like imbalance than spinning, and rises and falls along with neck pain and stiffness.
3. Can a neck problem really cause dizziness?
Yes. The upper cervical spine has one of the densest concentrations of proprioceptive sensors in the entire body. These sensors feed your brain real-time information about head position and movement. When the upper cervical spine is misaligned or dysfunctional, those signals get distorted, and your brain receives mismatched data from your eyes, inner ear, and neck. That sensory mismatch is what produces the dizziness.
4. What causes cervicogenic dizziness in the first place?
The most common causes are trauma-related: motor vehicle accidents, whiplash, concussions, falls, and sports injuries. Cumulative factors also play a role, including forward head posture, poor sleep position, chronic stress, old untreated injuries, and prolonged screen time. Connective tissue conditions like hypermobility and Ehlers-Danlos syndrome can also predispose someone to upper cervical instability and dizziness.
5. How is cervicogenic dizziness diagnosed?
It is what doctors call a diagnosis of exclusion. There is no single test that proves it, so providers must rule out other causes — inner ear disorders, neurological conditions, cardiovascular problems, blood pressure issues, and medication side effects — and then confirm that dizziness is closely tied to demonstrable cervical spine dysfunction. A thorough history, neurological exam, vestibular testing, and detailed cervical assessment are all part of the process.
6. Will an MRI or CT scan show cervicogenic dizziness?
Standard MRIs and CT scans usually look normal in patients with cervicogenic dizziness because the problem is functional rather than structural. The bones are not broken, the discs may not be herniated, and the soft tissues may look fine on imaging. That is why so many patients are told their scans are “normal” while they continue to struggle. A 3D CBCT scan, like the one we use in our Sarasota office, is much better at revealing subtle alignment issues at the upper cervical spine that standard imaging misses.
7. Is cervicogenic dizziness permanent?
In most cases, no. With appropriate care addressing the underlying cervical dysfunction, the majority of patients experience significant improvement or complete resolution of symptoms. Without treatment, however, symptoms can persist for years and may worsen over time, especially when stress, poor posture, or additional injuries are added on top.
8. How long does it take to see results with upper cervical care?
Every patient is different. Some notice changes within the first few visits, while others — especially those with long-standing symptoms or significant trauma history — take several weeks to months to experience meaningful improvement. The published case series and clinical reports we reviewed showed average improvements on the Dizziness Handicap Inventory of around 67 percent over a thirty-day care period when upper cervical care was combined with appropriate home support.
9. Is upper cervical chiropractic safe for cervicogenic dizziness?
When performed by a properly trained upper cervical specialist using imaging-guided precision, the Advanced HIO Knee Chest Upper Cervical Technique we use is one of the gentlest forms of chiropractic care available. There is no twisting, no yanking, no popping, and no cracking. The correction is a small, specific contact delivered with light force at exactly the angle the imaging tells us is needed.
10. Will I need to come in forever?
No. Our goal is to correct the underlying problem, stabilize the upper cervical spine, and then transition you to maintenance visits at whatever interval keeps you feeling your best. Some patients choose to continue periodic visits for ongoing nervous system support, while others come in only as needed. Care plans are individualized and discussed transparently at the report-of-findings visit.
11. Can I have cervicogenic dizziness along with another condition like vestibular migraine or BPPV?
Yes, and it happens often. Cervicogenic dizziness frequently coexists with vestibular migraine, BPPV, post-concussion syndrome, Mal de Débarquement Syndrome, persistent postural-perceptual dizziness, and dysautonomia. Addressing all the contributing pieces — rather than just one — is often what finally moves the needle for patients who have only had partial relief from previous treatments.
12. What if I have already tried physical therapy and it did not help?
Physical therapy can absolutely help some patients with cervicogenic dizziness, particularly when it is paired with vestibular rehabilitation. However, if the upper cervical spine is misaligned in a specific way, no amount of generalized stretching or strengthening will fully correct it. Many of our patients come to us after PT and find that adding precise upper cervical correction is what finally allows their nervous system to settle.
13. What if regular chiropractic adjustments have not helped?
General chiropractic and upper cervical chiropractic are two different disciplines. A standard adjustment is often a broad, manual manipulation that produces an audible release across a region of the spine. Upper cervical care is much more focused — it targets the atlas and axis specifically, uses 3D imaging to calculate the exact correction needed, and applies that correction with a precise, low-force contact. Patients who have not responded to general chiropractic care often do respond to upper cervical care because the target is different.
14. Do I need a referral from my medical doctor to come in?
No. Florida is a direct-access state, meaning you do not need a referral to see a chiropractor. You can call our office or book a complimentary consultation directly online. That said, we collaborate respectfully with primary care providers, neurologists, ENTs, and physical therapists, and we are always happy to communicate with your existing care team when that helps your overall plan.
15. How do I know if I am a good candidate for upper cervical care?
The best way to find out is to come in for a complimentary consultation. We will listen to your full history, perform a thorough examination, capture your 3D CBCT and thermography images, and review the findings with you in plain language. If we believe we can help, we will lay out exactly what care would look like. If we do not believe we are the right fit for your situation, we will tell you honestly and help guide you toward someone who is. You leave informed, either way.
You Don’t Have to Live This Way
There is a particular kind of exhaustion that comes from being dizzy for months or years. It is not just the physical drain of fighting gravity all day. It is the mental load of always tracking how you feel, always scanning for the next wave, always wondering whether you are safe to drive, exercise, go to the store, or pick up your kids. It is the slow, quiet narrowing of your life as you avoid the situations that make symptoms worse. And it is the deep frustration of having normal scans, normal labs, and normal exam findings while you feel anything but normal.
We see this exhaustion in our consultation room every week. We also see the other side of it — patients who finally find their answer, who finally get the right care, and who finally start living again. They report being able to drive without anxiety. They get back into the gym. They travel. They sleep through the night. They stop carrying a list of “safe” places to go because every place starts to feel safe again. The neck pain quiets. The headaches fade. The brain fog clears. The ground feels solid beneath their feet, sometimes for the first time in years.
This is what is possible when the right cause is matched with the right care. Cervicogenic dizziness is real, it is treatable, and it deserves more than another shrug, another prescription, or another “your tests look fine.” If your story sounds like the one we have described here, we would love to listen to it in full and help you figure out whether your upper neck is the missing piece.
Call our office at (941) 243-3729 or book your complimentary consultation online at https://intake.chirohd.com/new-patient-scheduling/724/lavender-family-chiropractic. Dr. Rusty Lavender, Dr. Jacob Temple, and our entire team at Lavender Family Chiropractic in Sarasota are ready to help you find solid ground again.
Related Articles
The World Won’t Stop Spinning: PPPD, Persistent Dizziness, Sensory Overload, and Why the Answer May Be in Your Upper Neck — https://chiropractorsarasotaflorida.com/the-world-wont-stop-spinning-pppd/
When You Step Off the Boat and the Boat Won’t Stop: A Sarasota Guide to Mal de Débarquement Syndrome (MdDS) — https://chiropractorsarasotaflorida.com/mal-de-debarquement-syndrome-2/
Vestibular Hypofunction: How to Resolve the Dizziness with Proven Results — https://chiropractorsarasotaflorida.com/vestibular-hypofunction/
Related Posts
Popular Posts
