

MRI for Dizziness: You stood up from your beach chair on Siesta Key and the world tilted. You turned your head to back out of the driveway on Clark Road and a wave of unsteadiness rolled through you. You woke up at 3 a.m. in your home off Lakewood Ranch Boulevard and the ceiling was spinning. You spent an afternoon hunched over your laptop at a Bradenton coffee shop and by dinner the floor felt soft beneath your feet. Now you cannot sleep because you keep replaying everything you have read online — brain tumor, stroke, multiple sclerosis, acoustic neuroma — and one question is repeating in your head on a loop:
Should I get an MRI?
It is one of the most common questions we hear at our office. Patients come into Lavender Family Chiropractic from Sarasota, Bradenton, Lakewood Ranch, Venice, Osprey, Parrish, Palmetto, and across the Suncoast every single week, scared, exhausted, and looking for answers about dizziness that no one has been able to explain. Some of them are holding a normal MRI report in their hand and feeling more confused than ever. Others have been told they “do not need imaging” but the dizziness will not let them rest. Almost all of them ask the same thing: Is this in my head — literally? Is something serious going on in my brain?
Here is the honest answer, supported by the best evidence in neurology and emergency medicine: in the overwhelming majority of cases, the answer is no — and the answer is also not in your inner ear. In the vast majority of chronic, recurring, or unexplained dizziness, the real driver is sitting an inch below your skull, at the top two bones of your neck — a place almost no MRI, no CT scan, no ENT workup, and no neurologist will ever specifically evaluate from a functional standpoint.
This article is a complete guide to when an MRI is genuinely indicated for dizziness, when it is not, what it can and cannot tell you, and why the upper neck and craniocervical junction are so often the missing piece. Let us walk through it together.
What Is Dizziness, Really? And Why the Word Itself Is Confusing
The word “dizziness” is a catch-all term that patients, doctors, and even researchers use to describe four very different sensations. Sorting out which one you are experiencing is the first and most important step in figuring out whether you need imaging — and what is actually causing the problem.
The four categories of dizziness are:
Vertigo — a false sensation of motion. The room spins, you spin, the floor tilts, you feel like you are on a boat. Vertigo is usually triggered or worsened by head movement and is the type of dizziness most likely to be tied to the vestibular system or upper neck.
Lightheadedness or presyncope — the feeling that you are about to faint. This is typically tied to blood pressure, blood sugar, hydration, or autonomic nervous system issues (like POTS or dysautonomia).
Disequilibrium — a feeling of being off-balance or unsteady on your feet, especially when walking. This often shows up in older adults, after concussions, or with neurological conditions.
Non-specific dizziness — a vague feeling of being “off,” foggy, swimmy, floaty, or simply not right. This is the most common type and the hardest to pin down.
The reason this matters is that most MRIs are ordered when patients say the single word “dizzy” — but the most appropriate workup depends entirely on which type of dizziness you actually have. And the type that is most often driven by the upper neck and most commonly misdiagnosed is true vertigo and non-specific dizziness.
When Is an MRI Actually Indicated for Dizziness?
According to Johns Hopkins Medicine’s imaging guidelines, MRI of the brain and internal auditory canal (with and without IV contrast) is the imaging test of choice when imaging is genuinely needed — because it is superior to CT for visualizing the posterior fossa, which is where most dangerous central causes of vertigo originate. However — and this is the part most patients are never told — most dizziness does not require imaging at all. Imaging is meant to rule out specific, serious pathology, not to diagnose the cause of routine dizziness.
The accepted “red flags” that should prompt an MRI for dizziness are:
Sudden, severe vertigo or dizziness that does not match a typical positional pattern, especially if it appears with headache, weakness, visual disturbance, hearing loss, or facial numbness.
Neurological red flags on examination — problems with coordination, balance, walking, eye movements, speech, swallowing, facial sensation, or other cranial nerve functions.
Persistent or progressive dizziness that does not improve over weeks despite conservative care.
Asymmetric hearing loss, ringing in one ear, or persistent unilateral aural fullness — these can be signs of a vestibular schwannoma (acoustic neuroma).
Cases where the standard examination and positional tests for BPPV do not explain the symptoms.
A history of significant head or neck trauma with new neurological symptoms.
The HINTS exam findings or pattern that suggests central rather than peripheral cause — this is a specialized bedside neurological exam that, in experienced hands, is actually more sensitive than early MRI for posterior circulation stroke.
In other words, if you have any of the classic red flags — sudden onset, neurological deficits, severe and unexplained symptoms, suspicion of stroke or tumor, or progressive worsening — you need to be evaluated in an emergency setting and you may absolutely need an MRI. We tell every patient who comes through our doors: if you have these red flags, the right next step is the emergency department, not a chiropractor.
What an MRI Can and Cannot Tell You
Here is what is important to understand about MRI for dizziness: when imaging is indicated, MRI is genuinely a powerful tool. It can identify or rule out:
Acute and chronic ischemic disease including posterior circulation strokes (although early small strokes can be missed even on MRI in the first 24 to 48 hours).
Cerebellopontine angle tumors such as vestibular schwannomas and meningiomas.
Multiple sclerosis and other demyelinating diseases.
Brain tumors, cysts, or mass lesions near the brainstem or cerebellum.
Structural inner ear abnormalities including some causes of hearing loss and tinnitus.
Vertebral or basilar artery dissection (when combined with MRA).
These are real, important, sometimes life-threatening conditions, and ruling them out matters. We are not anti-MRI. We are very pro-finding the actual cause of your dizziness — and that often starts with the right testing.
But here is the part patients are rarely told: a normal MRI does not mean nothing is wrong. It means specific, structural, gross pathology is not present. Multiple high-quality studies have shown that even patients with eventual confirmed posterior circulation stroke can have negative early MRI scans. A study published in clinical research from Pusan National University found that among more than 1,800 patients with posterior circulation stroke, a meaningful subset had initial negative MRI-DWI scans despite acute symptoms. That is to say: MRI is helpful when positive, but a clean scan does not always rule out a problem — it especially does not rule out functional, mechanical, or neurological dysfunction that does not produce visible lesions.
This is the critical point: the most common cause of chronic dizziness in our patient population — and in the general population — is not visible on MRI at all.
Why Most Dizziness Comes from the Neck, Not the Brain
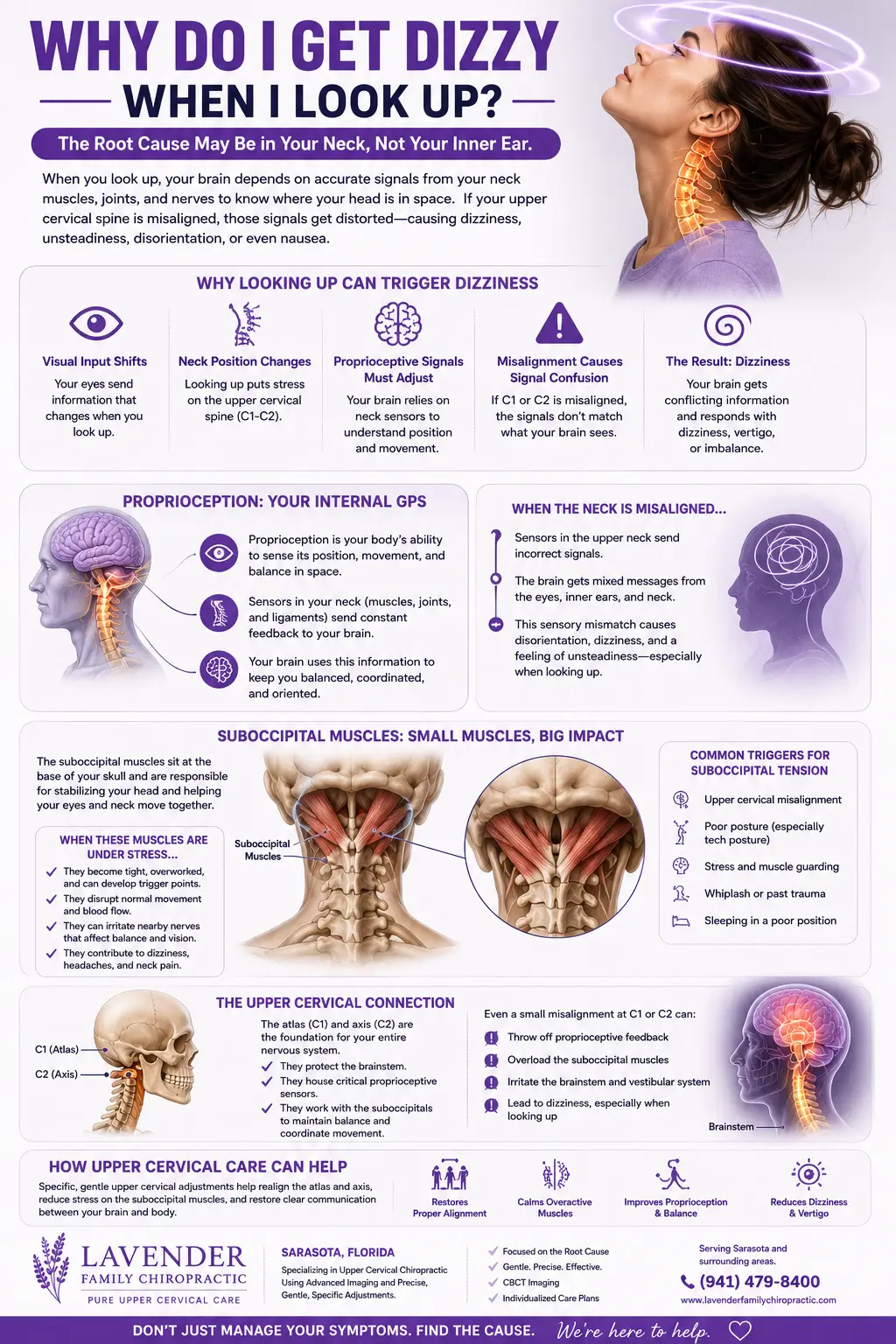
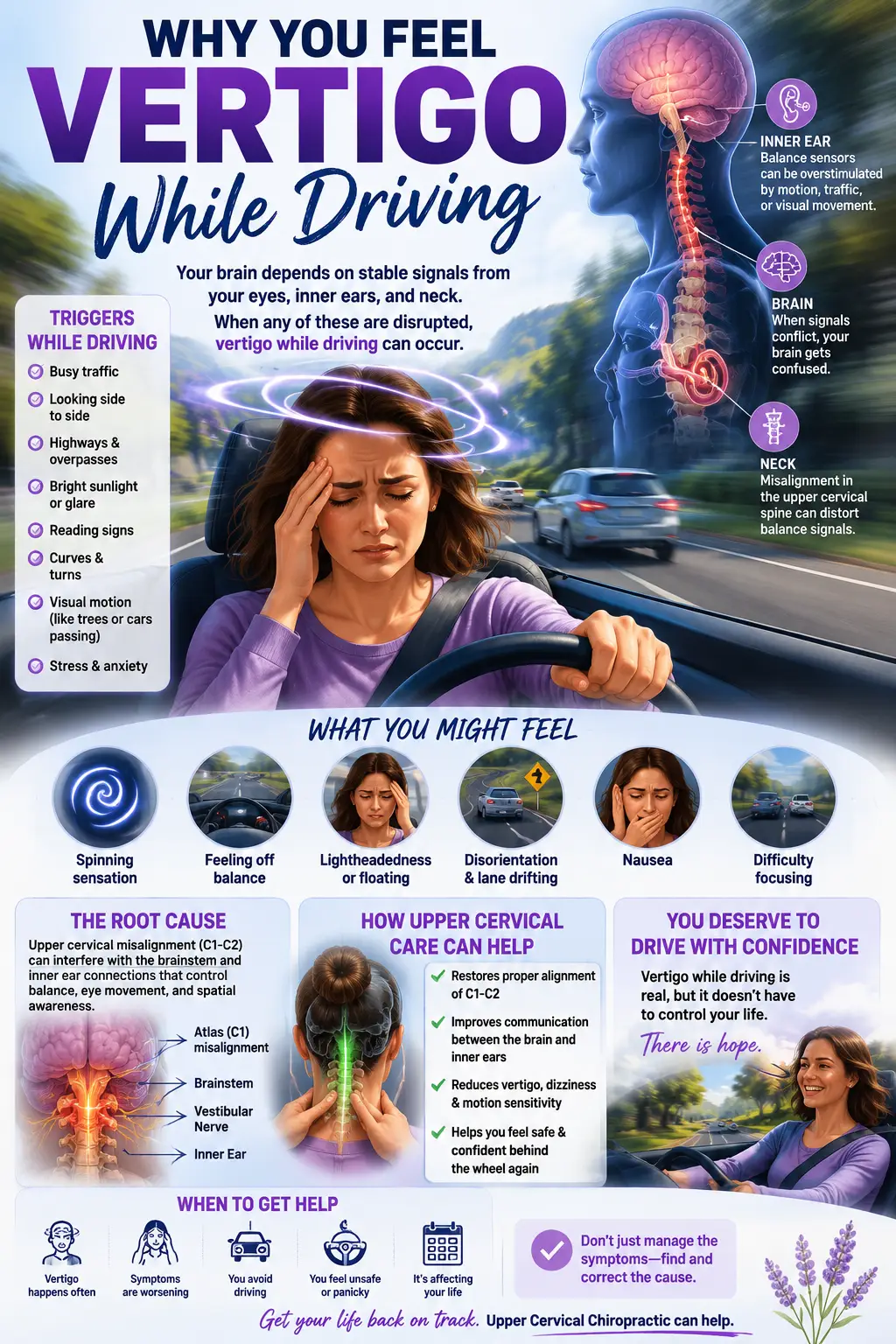
Here is what is rarely explained to patients: your sense of balance is not produced by your inner ears alone. It is the result of three sensory systems constantly feeding information to your brainstem:
The vestibular system — your inner ears, which sense head motion and orientation through the semicircular canals and otolith organs.
The visual system — your eyes, which provide information about the horizon and your environment.
The proprioceptive system — your joints, muscles, and ligaments, which tell your brain where your body is in space.
Of those three, your upper neck — specifically the joints, muscles, and ligaments of the top two cervical vertebrae (the atlas, C1, and axis, C2) — contains one of the highest concentrations of proprioceptive sensors anywhere in the human body. In fact, research has shown that even tiny positional changes in the upper cervical spine — as small as 0.4 degrees — are enough to produce a significant change in the afferent signals being sent to the brain.
When the upper cervical spine is misaligned, irritated, or mechanically dysfunctional from trauma, posture, repetitive strain, or old injuries, those proprioceptive signals become noisy and inaccurate. The brain then receives a mismatched picture: the eyes say one thing, the inner ear says another, and the neck says something different again. The brain tries to reconcile the conflict — and the conscious experience of that conflict is dizziness, vertigo, brain fog, motion sensitivity, unsteadiness, or that vague “off” feeling so many of our patients describe.
This phenomenon has a name: cervicogenic dizziness. A 2025 perspective paper published in a peer-reviewed journal defined cervicogenic dizziness as “a nonspecific sensation of altered orientation in space and disequilibrium originating from abnormal afferent activity from the neck,” noting that it is thought to be caused primarily by disorders in the upper cervical spine. The same paper noted that dizziness and vertigo affect up to 20 percent of adults annually — and that a significant portion of those cases are driven by sensory mismatch arising from the neck.
You can review more about how this works in our detailed article on upper cervical chiropractic care.
The Craniocervical Junction: The Most Important Inch in Your Body
The craniocervical junction — the meeting point between the base of your skull and the top of your spine — is one of the most neurologically dense, mechanically complex, and clinically overlooked areas in the entire human body. This small region houses:
The lower brainstem, including the vestibular nuclei that process and integrate balance information from your inner ears, eyes, and neck.
The trigeminocervical nucleus, a convergence hub where nerves from the face, head, and upper neck communicate — which is why upper neck dysfunction so often produces headaches, facial pain, and visual motion sensitivity.
The vertebral arteries, which travel through bony canals in the C1 and C2 vertebrae before entering the skull to supply the brainstem and cerebellum.
The vagus nerve and other cranial nerves that influence everything from heart rate and digestion to vocal cord function.
The flow of cerebrospinal fluid (CSF) through the foramen magnum.
When any of these structures are irritated, compressed, or functionally stressed by upper cervical misalignment, the consequences can show up as dizziness, vertigo, headache, brain fog, ear pressure, tinnitus, neck pain, autonomic symptoms — or all of the above simultaneously. A retrospective case series published in the Journal of Contemporary Chiropractic specifically described how a malpositioned craniocervical junction can generate improper cervical proprioceptive afferents that do not match input from the otolith organs and semicircular canals — producing exactly the kind of sensory mismatch that causes chronic dizziness.
Here is the part that makes this so frustrating for patients: a standard MRI of the brain looks at the brain, not at the function of the upper neck. An MRI of the cervical spine looks for disc herniations, stenosis, and gross structural pathology, not at the precise positional and functional relationship of C1 to the skull or C2. The vast majority of upper cervical misalignments cannot be seen on a standard MRI at all — they require specialized 3D imaging (such as cone beam CT) measured with millimeter-level precision.
Why Traditional Care Often Misses This
If most chronic dizziness is being driven by the upper neck, why does almost no one find it? Because the conventional pathway is not designed to look there. A typical dizziness workup goes something like this:
You see your primary care doctor → they prescribe meclizine and refer you to ENT → ENT does hearing tests and a videonystagmography (VNG) → results are inconclusive or show a “mild abnormality” → you are referred to a neurologist → the neurologist orders an MRI of the brain → the MRI is normal → you are told it is “probably vestibular migraine” or “PPPD” or “anxiety” or “BPPV” and sent home with medications, vestibular rehab exercises, or both.
Every step of this process is reasonable. Every step is also missing the upper neck. ENTs do not examine the function of the atlas and axis. Neurologists do not measure the precise positional alignment of C1. MRIs are not designed to detect functional craniocervical misalignment. Vestibular rehab assumes that the incoming sensory data is accurate — but if the neck is sending noisy signals, retraining the brain on bad data only goes so far.
This is why so many of our patients arrive at Lavender Family Chiropractic having been everywhere else first. As we wrote in our companion guide on what doctor to see when you are dizzy, many patients with persistent dizziness have completely normal imaging of the brain and ears — and yet the dizziness is real, debilitating, and traceable to a structural problem in the upper neck that simply does not show up on the tests they have been running.
Upper Cervical Chiropractic Care: A Different Approach to Dizziness
Upper cervical chiropractic care is a specialty within chiropractic that focuses exclusively on the precise correction of the atlas (C1) and axis (C2). It is not the kind of chiropractic care most people picture. There is no twisting, no popping, no cracking of the neck. The corrections are gentle, specific, and measured to the millimeter — guided by 3D imaging and based on the unique anatomy of each individual patient.
At our office, we use Cone Beam CT (CBCT) imaging to create a precise three-dimensional map of your upper cervical alignment, and Tytron functional nervous system scans to objectively measure how your autonomic nervous system is responding before and after corrections. This means our care is data-driven from the first visit — we are not guessing, we are measuring.
What to Expect at Lavender Family Chiropractic
When you come in for your first visit at Lavender Family Chiropractic, the process is thorough but unhurried. We start with a detailed conversation about your health history — every accident, every fall, every concussion, every episode of dizziness, every previous diagnosis, every imaging study you have had done. We want the whole picture, not just the symptom of the moment.
From there, we perform a careful neurological examination, postural and gait analysis, and functional nervous system scanning with our Tytron infrared technology. If clinically indicated, we then perform 3D CBCT imaging so we can see exactly what is happening at your craniocervical junction. Most patients are amazed at the level of detail — they can see their own atlas, axis, and skull in three dimensions, often for the first time in their lives.
Our doctors — Dr. Rusty Lavender and Dr. Jacob Temple — then sit down with you, walk through your findings in plain language, and explain whether you are a good candidate for care. If you are, we design a specific correction protocol based on your unique measurements. The actual adjustments take seconds, involve no force, and most patients describe them as feeling like a gentle pressure. There is no cracking, no twisting, no popping.
You can learn more about our process on our What to Expect page.
Ready to find out if your dizziness is coming from your neck? We offer complimentary consultations to help you decide if upper cervical care is right for you. Schedule your visit at Lavender Family Chiropractic — call (941) 243-3729 or book online.
The Research Behind Upper Cervical Care for Dizziness
The evidence base for the connection between the upper cervical spine and dizziness has been quietly growing for decades. Some of the most relevant findings include:
A retrospective case series published in the Journal of Contemporary Chiropractic documented improvement in dizziness following upper cervical chiropractic technique combined with individualized vestibular rehabilitation, describing the mechanism by which craniocervical malposition can generate the cervical proprioceptive mismatch responsible for cervicogenic dizziness.
A randomized controlled trial registered at ClinicalTrials.gov (NCT02772042) investigated the effectiveness of traction manipulation of the upper cervical spine on cervicogenic dizziness, measuring changes in dizziness intensity, cervical range of motion, and quality of life — and finding meaningful improvements in patients receiving upper cervical intervention.
A 2024 case report published in Cureus by Trager and colleagues described conservative management of cervicogenic dizziness associated with upper cervical instability and postural orthostatic tachycardia syndrome (POTS), in which a 27-year-old woman with a six-year history of dizziness, neck pain, and incapacitating dizzy spells substantially improved over eight months of gentle manual therapies and cervical stability work — after years of failed conventional treatment.
Imaging research using upright MRI has demonstrated that upper cervical misalignment can affect cerebrospinal fluid flow dynamics at the craniocervical junction, providing a plausible mechanism for the dizziness, head pressure, and motion sensitivity so frequently reported by patients with upper cervical dysfunction.
Studies on cervical proprioception have repeatedly shown that the upper cervical spine contains one of the densest concentrations of mechanoreceptors in the body, with direct neural connections to the vestibular nuclei in the brainstem — establishing the anatomical and physiological basis for cervicogenic dizziness.
The picture that emerges from this body of research is clear: the upper neck is a major, often dominant, contributor to chronic dizziness — and addressing it through precise, gentle upper cervical care produces measurable clinical improvement in patients who have failed other approaches.
Lifestyle Factors That Complement Upper Cervical Care
While correcting the underlying structural and neurological dysfunction at the upper neck is the cornerstone of lasting relief from dizziness, your daily habits play a significant supporting role. The patients who do best in our office are those who pair their corrections with simple, sustainable lifestyle adjustments that support the nervous system and reduce the load on the vestibular system.
Sleep position matters more than people realize. Sleeping on a pillow that is too tall, sleeping with your head twisted, or sleeping on your stomach can all place sustained mechanical stress on the upper cervical region. We generally recommend a back or side-sleeping position with a pillow that keeps the head level with the spine.
Hydration directly affects vestibular function. Florida heat is unforgiving, and even mild dehydration can amplify dizziness, lightheadedness, and motion sensitivity. Most adults need significantly more water than they think — especially on the Gulf Coast.
Screen ergonomics and posture matter. Long hours spent looking down at a phone or hunched over a laptop create chronic upper cervical strain that can perpetuate cervicogenic dizziness. Raising your monitor to eye level, taking frequent breaks, and being intentional about your head posture throughout the day makes a real difference.
Caffeine, alcohol, and dietary triggers can amplify vestibular symptoms, particularly in patients with vestibular migraine or motion sensitivity. Many of our patients find that reducing these — even temporarily — speeds their recovery.
Stress and autonomic regulation play a much larger role in chronic dizziness than most patients realize. Many people with persistent dizziness are also dealing with chronic nervous system dysregulation — they are stuck in fight-or-flight mode. Gentle breathing work, time in nature, daily walks, and steady sleep routines all support the parasympathetic nervous system and accelerate healing. If you suspect autonomic involvement, you may also benefit from reading our deeper guide on the vagus nerve and upper cervical care.
These are not magic fixes, but combined with proper upper cervical correction, they create the conditions in which the nervous system can finally heal.
Serving Sarasota, Bradenton, Lakewood Ranch, and the Surrounding Gulf Coast
Lavender Family Chiropractic is located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — right at the corner of University Parkway and Whitfield Avenue, easily accessible from anywhere on the Suncoast. We are proud to serve patients from:
Sarasota, Bradenton, Lakewood Ranch, Palmer Ranch, Siesta Key, Longboat Key, Lido Key, Anna Maria Island, Holmes Beach, Bradenton Beach, Venice, North Port, Port Charlotte, Punta Gorda, Osprey, Nokomis, Parrish, Palmetto, Ellenton, Myakka City, University Park, Tara, and Lakewood Ranch surrounding communities. Whether you are coming from a high-rise condo on the bayfront, a ranch out east, or a quiet street in a Bradenton neighborhood, we make it easy to access care.
For a full list of communities we serve and directions to our office, please visit our Areas We Service page.
Top 15 Frequently Asked Questions About MRI, Dizziness, and Upper Cervical Care
1. Do I need an MRI if I have dizziness?
Not necessarily. Most cases of dizziness do not require imaging. An MRI is generally indicated when there are neurological red flags, sudden severe onset, asymmetric hearing loss, suspicion of stroke, persistent unexplained symptoms, or signs of a structural lesion.
2. My MRI came back normal — why am I still dizzy?
This is one of the most common scenarios we see. A normal MRI rules out gross structural disease but does not evaluate the functional mechanics of your upper neck, which is the most common driver of chronic dizziness.
3. Can the upper neck really cause dizziness?
Yes. The upper cervical spine has one of the highest concentrations of proprioceptive sensors in the body, and those sensors feed directly into the vestibular nuclei in the brainstem. When the upper neck is misaligned or dysfunctional, the brain receives mismatched balance signals — which is experienced as dizziness or vertigo.
4. What is cervicogenic dizziness?
Cervicogenic dizziness is dizziness arising from abnormal afferent signals from the upper neck. It is typically associated with neck pain, stiffness, or a history of neck injury, and is aggravated by certain head positions or movements.
5. How is upper cervical chiropractic different from regular chiropractic?
Upper cervical care is a specialty focused exclusively on the precise correction of C1 and C2 using 3D imaging and gentle, measured techniques. There is no twisting, cracking, or popping of the neck.
6. Is upper cervical care safe for vertigo and dizziness?
Yes, it is one of the gentlest forms of chiropractic care. The corrections are low-force, specific, and based on individual measurements taken from your imaging.
7. Can upper cervical care help if I have already tried vestibular rehab?
Yes. Vestibular rehab works best when the underlying sensory input is accurate. If your upper neck is sending noisy signals, addressing that structural issue often allows vestibular rehab to finally produce lasting results.
8. How long does it take to feel better?
This varies depending on how long the dizziness has been present, what is driving it, and your individual response. Many patients notice changes within the first few corrections, while more chronic cases may take weeks to months of consistent care.
9. What if my dizziness started after a car accident or concussion?
Post-traumatic dizziness is one of the conditions we see most often respond well to upper cervical care, because trauma is one of the most common causes of upper cervical misalignment.
10. Do I need to keep coming forever?
No. Our goal is to correct the underlying problem and then transition you to a maintenance schedule that holds your correction long-term. Most patients move from active care into much less frequent visits as their nervous system stabilizes.
11. Will insurance cover this?
Coverage varies by plan. We will be transparent with you about cost and options during your initial consultation.
12. Can children or older adults benefit from upper cervical care?
Yes. The corrections are scaled to each individual’s body, tissue sensitivity, and age. We see pediatric patients and seniors regularly.
13. What if I have already been diagnosed with BPPV, vestibular migraine, or Meniere’s?
Many patients carry these diagnoses while also having upper cervical involvement. Addressing the upper neck often dramatically reduces symptom frequency and severity, even when one of those conditions is also present.
14. Is upper cervical care a substitute for emergency medical care?
Absolutely not. If you have neurological red flags — sudden severe onset, weakness, facial drooping, speech problems, double vision, severe headache — go to the emergency department. Upper cervical care is for chronic, recurring, or unexplained dizziness once serious pathology has been ruled out.
15. How do I know if I am a good candidate?
The best way to find out is to come in for a complimentary consultation. We will review your history, perform our exam and scans, and tell you honestly whether we believe we can help — or whether you would be better served by a different provider.
You Do Not Have to Live with Dizziness — and You Do Not Have to Guess
If you have been struggling with dizziness, vertigo, brain fog, motion sensitivity, or that constant feeling of being “off” — and you have been wondering whether you need an MRI, whether something is seriously wrong, or whether anyone is actually going to help you find an answer — please know this: most dizziness is not caused by something dangerous, most dizziness is not visible on imaging, and most dizziness is treatable.
The right MRI at the right time can rule out the serious things you may be worried about. But once those serious things have been ruled out — and they usually are — the next question is not “what is wrong with my brain?” The next question is “what is wrong with my neck?” And in our experience, after thousands of patient visits, the answer is almost always sitting an inch below the skull, waiting to be measured, corrected, and finally addressed.
Lavender Family Chiropractic is here for you. Our doctors — Dr. Rusty Lavender and Dr. Jacob Temple — have built this practice around helping the people who have been everywhere else first and are ready for real answers.
Call us at (941) 243-3729, or schedule your complimentary consultation online here. We are located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, and we serve patients across Sarasota, Bradenton, Lakewood Ranch, and the entire Suncoast.
Your steady ground is waiting.
Related Articles
- Our #1 Recommendation to Fix Vertigo: The Missing Link to Fixing Vertigo and Dizziness at Its Root Cause
- When Your Head Feels Too Heavy: Craniocervical Instability, Vertigo, Neck Pain, and Migraines
- Vestibular Hypofunction: How to Resolve the Dizziness — Proven Results
This blog is for informational purposes only and does not constitute medical advice. Please consult a qualified healthcare provider for diagnosis and treatment of any health condition. Lavender Family Chiropractic | 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 |
Related Posts
Popular Posts
