
Vasovagal Syncope: You’re standing in line at Publix on University Parkway. The room gets warm. Your vision starts to gray at the edges. You feel sweaty, nauseous, and suddenly your knees feel like they belong to someone else. The next thing you know, you’re on the floor with strangers standing over you, asking if you’re okay.
If that scenario sounds familiar — or if you’ve ever fainted at the sight of blood, during a blood draw, after standing too long in the Florida heat, or right after a stressful moment — you’ve likely experienced vasovagal syncope. It is the most common cause of fainting in the world, and the people who deal with it know it isn’t “no big deal.” Recurrent episodes erode confidence. Falls cause real injuries. Driving, exercise, and even simple errands start to feel risky.
At Lavender Family Chiropractic in Sarasota and Lakewood Ranch, we meet patients every week whose fainting spells, near-faints (presyncope), and dizziness have been brushed off as “just vasovagal.” They’ve often had a normal EKG, a normal tilt table, normal bloodwork, and a polite shrug from their doctor. What rarely gets investigated is the structure that physically protects and surrounds the vagus nerve and brainstem — the upper cervical spine.
This guide walks through what vasovagal syncope actually is, why it happens at the level of the nervous system, how the upper neck plays a role that’s often missed, and how the precise, gentle care offered by our Sarasota team — Dr. Rusty Lavender and Dr. Jacob Temple — fits into a real recovery plan.
What Is Vasovagal Syncope?
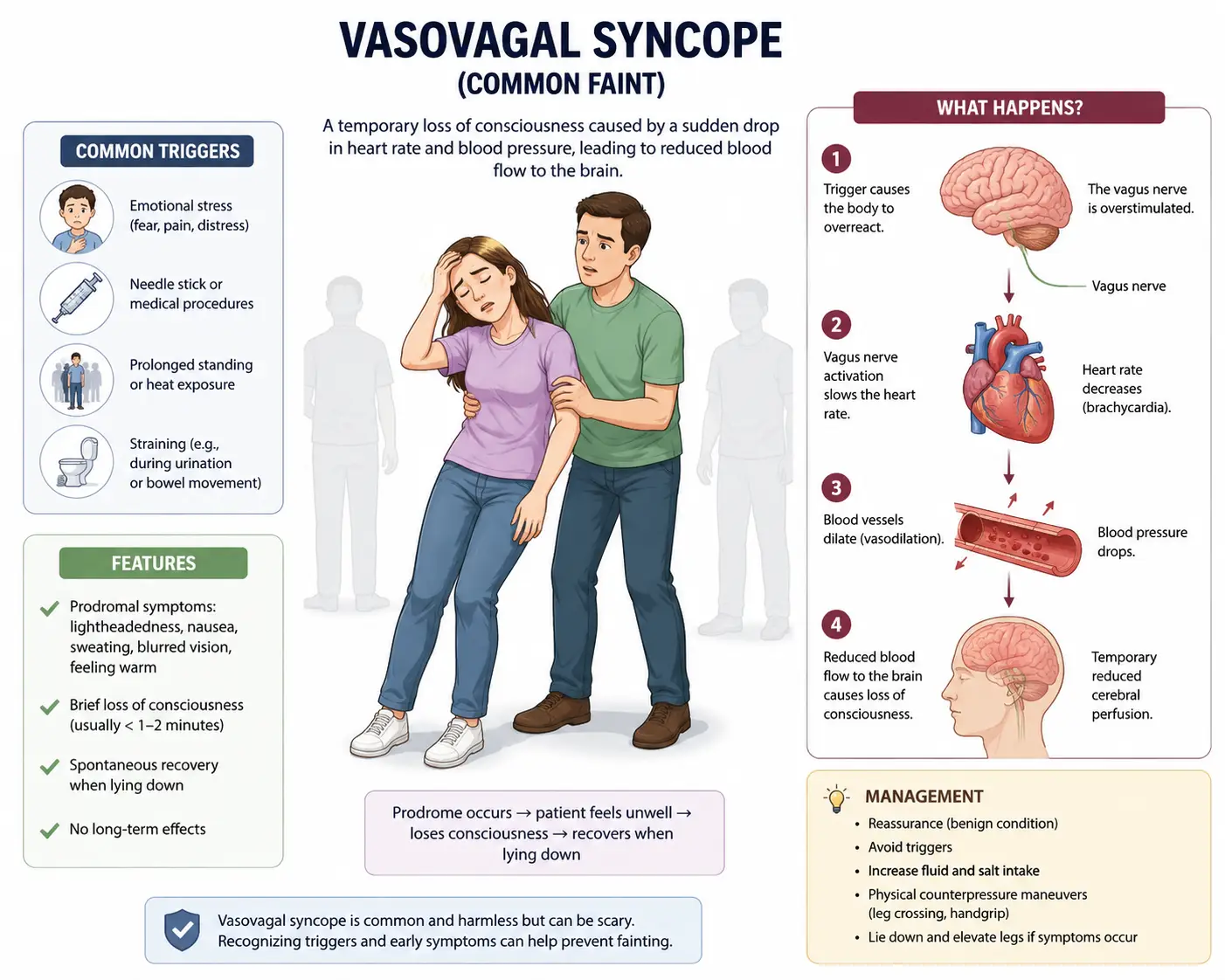
Vasovagal syncope is a brief loss of consciousness caused by a sudden drop in heart rate and blood pressure, which reduces blood flow to the brain. It’s also called neurocardiogenic syncope or reflex syncope, and according to Wikipedia, it occurs in more than 1 per 1,000 people per year and is by far the most common form of fainting (Reflex syncope — Wikipedia).
The episode itself is usually short — seconds to a couple of minutes — but the lead-up (the prodrome) is what most patients remember:
- Lightheadedness or feeling “off”
- Sweating, often cold and clammy
- Nausea
- Tunnel vision, blurred vision, or graying out
- Ringing in the ears (tinnitus)
- Pale skin
- A sense of warmth or dread
- Weakness in the legs
Common triggers include prolonged standing, heat, dehydration, the sight of blood, pain, emotional stress, needles or medical procedures, straining on the toilet, coughing fits, or even a long hot shower. In Southwest Florida, where summer humidity is its own challenge, heat and standing are huge triggers — we see this pattern often in patients coming in from Lakewood Ranch, Bradenton, Parrish, Venice, and Sarasota.
While vasovagal syncope itself is rarely life-threatening, it isn’t harmless. The fall that comes with it can be. And the recurrent pattern — episode, fear of another episode, restricted lifestyle — is a quality-of-life problem that deserves a real solution, not just “avoid your triggers.”
What Happens in the Nervous System and Blood Vessels During a Faint
To understand why upper cervical chiropractic care matters here, it helps to understand the actual mechanism of a vasovagal episode. Two systems are doing a complicated dance: the autonomic nervous system and your cardiovascular system.
Your autonomic nervous system has two main branches:
- Sympathetic — your “fight or flight” accelerator. Speeds heart rate, raises blood pressure, narrows blood vessels.
- Parasympathetic — your “rest and digest” brake. Slows heart rate, lowers blood pressure, widens blood vessels. The vagus nerve is the dominant carrier of this signal.
In a typical vasovagal episode, the sympathetic system fires hard first — heart rate climbs, the heart contracts vigorously while underfilled (often because you’re standing and blood has pooled in the legs). Pressure receptors (C-fiber afferents) inside the heart wall misinterpret this state and trigger an overcorrection from the brainstem.
A peer-reviewed PubMed review describes this sequence well: orthostatic vasovagal syncope starts with venous pooling and a drop in stroke volume, followed by cardioinhibition (a sudden slowing of heart rate) that accelerates the falling blood pressure. The authors describe four distinct phases — early stabilization, circulatory instability, terminal hypotension, and recovery — and emphasize that hormonal, respiratory, and psychological factors all modulate the response (Pathophysiology of vasovagal syncope: Novel insights — PubMed).
A second PubMed-indexed review goes further, explaining that vasovagal syncope is ultimately caused by an increase in sympathetic tone combined with an underfilled left ventricle, which stimulates cardiac afferent C fibers and triggers profound bradycardia and vasodilation. That combination reduces venous return and cerebral perfusion — and you faint (The Pathophysiology of Vasovagal Syncope and New Approaches to its Pharmacological Treatment — PubMed).
The key player throughout all of this is the vagus nerve — the tenth cranial nerve and the longest nerve of the autonomic nervous system. It travels from the brainstem, through the jugular foramen at the base of the skull, down through the carotid sheath in the neck, and on to the heart, lungs, and digestive tract. The vagus nerve is the master regulator of the parasympathetic “rest and digest” response and is the dominant control over heart rate, blood pressure variability, and digestion (Vagus nerve — Wikipedia).
When the vagus nerve fires too hard or too inappropriately — what’s often called “vagal hypertonia” — heart rate plummets and blood vessels dilate at exactly the wrong time. The result is the cascade described above: not enough oxygenated blood reaching the brain, and the lights go out.
So vasovagal syncope is, at its core, a miscommunication between the brainstem, the vagus nerve, and the cardiovascular system. Anything that irritates or destabilizes this circuit — including mechanical stress at the very top of the neck — can theoretically lower the threshold at which a vasovagal response gets triggered.
Why the Upper Cervical Spine Matters in Vasovagal Syncope
Here’s what doesn’t get discussed enough in standard syncope workups: the physical neighborhood of the vagus nerve and brainstem.
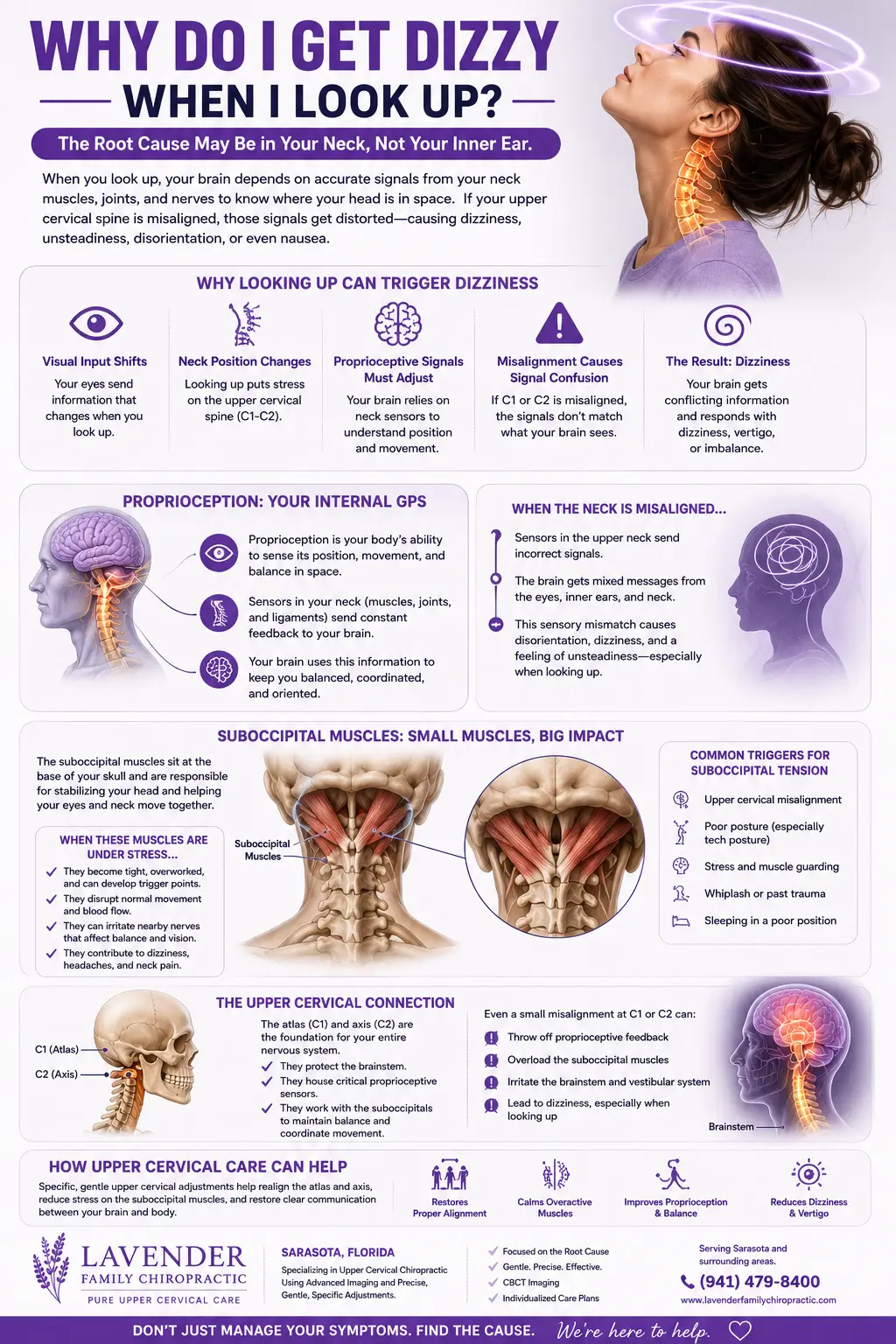
The brainstem sits inside the foramen magnum and is cradled by the top two vertebrae of the neck — the atlas (C1) and axis (C2). Just below the skull, the vagus nerve exits through the jugular foramen and runs down the front of the neck right next to the internal carotid artery and internal jugular vein. The vertebral arteries, which supply the back of the brain and brainstem, climb up through small holes (transverse foramina) in the upper cervical vertebrae before entering the skull.
That’s an extraordinary amount of vital plumbing and wiring concentrated into one small region.
When the atlas or axis sits out of optimal alignment — whether from an old whiplash, a sports impact, a difficult birth, a fall, repeated micro-stress from poor posture, or even a single hard hit — three things can happen at once:
- Mechanical irritation of the brainstem and vagus nerve area. Subtle tension on the dural attachments and soft tissue around the jugular foramen can alter how the vagus signals to the heart and blood vessels. This is the same mechanism we explore in detail in our blog on vagus nerve dysfunction and craniocervical instability.
- Disrupted vascular flow. Misalignment near the vertebral arteries and jugular veins can subtly compromise blood delivery to and venous drainage from the brain. Even small changes in cerebral perfusion lower the threshold for a syncope episode.
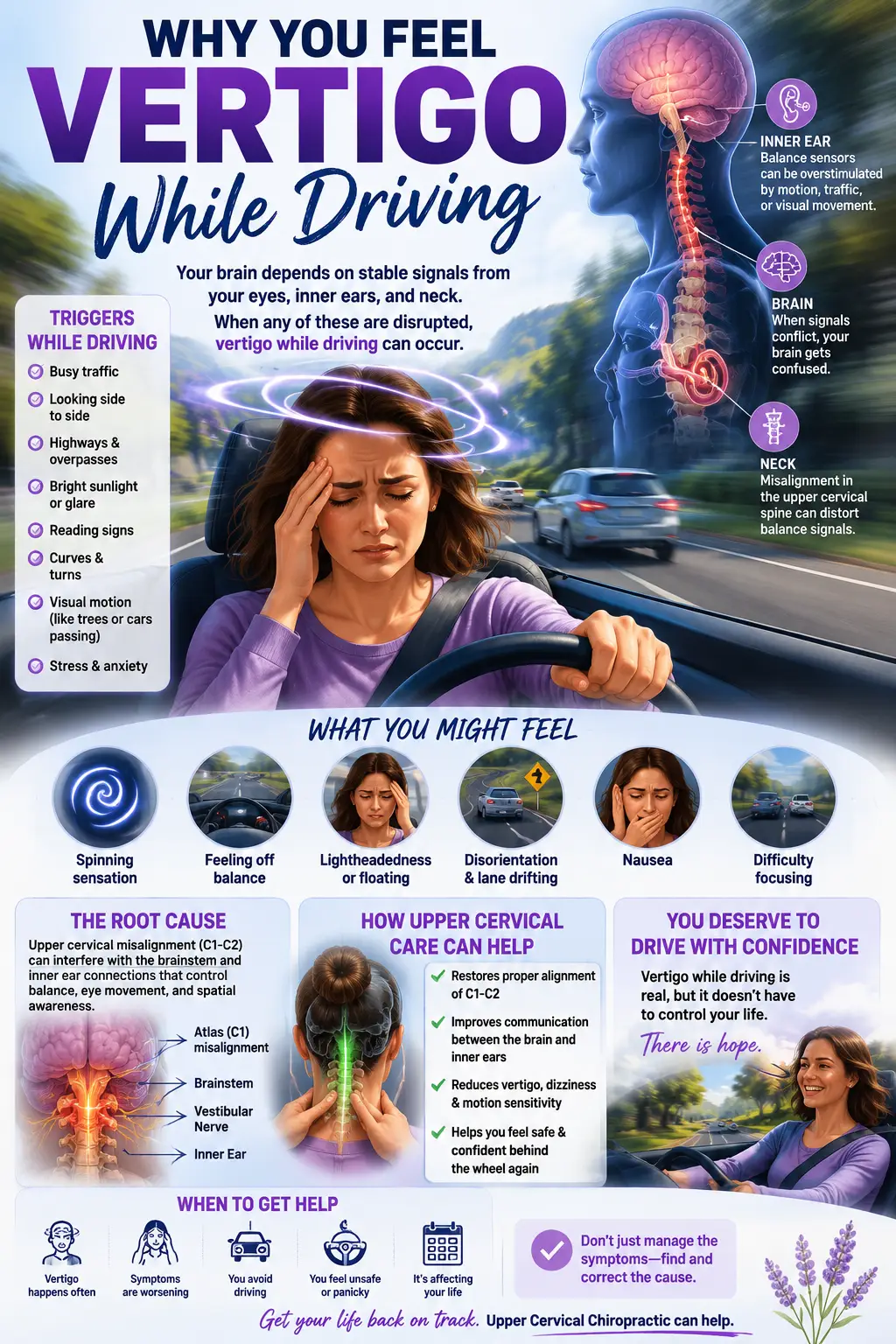
- Faulty proprioceptive input. The upper cervical spine is dense with proprioceptors — sensors that tell your brain where your head is in space. When that input is noisy or wrong, the brainstem’s regulation of balance, eye stabilization, and cardiovascular reflexes (including the baroreflex that protects against fainting) gets degraded.
This is why patients with chronic vasovagal episodes often also report:
- Dizziness or near-faints that aren’t full syncope
- Headaches or migraines
- Brain fog and difficulty concentrating
- Neck stiffness, especially at the base of the skull
- Anxiety, particularly anticipatory anxiety about the next episode
- POTS-like symptoms (racing heart on standing)
- Digestive issues — bloating, reflux, constipation
- Light sensitivity and motion sensitivity
If that cluster sounds like more than coincidence, that’s because it is. These are all systems regulated by — or sitting right next to — the upper cervical spine.
How Upper Cervical Chiropractic Care Works at Lavender Family Chiropractic
Upper cervical chiropractic is not the cracking, twisting, popping kind of chiropractic that most people picture. It’s a precision discipline focused entirely on restoring the proper position of the atlas (C1) and axis (C2) so the brainstem, vagus nerve, blood vessels, and cerebrospinal fluid can all do their jobs without mechanical interference.
You can read a full overview on our Upper Cervical Chiropractic Care page, but here’s how care at Lavender Family Chiropractic actually unfolds for someone dealing with vasovagal syncope.
What to Expect at Your First Visit
1. A real consultation. Dr. Rusty Lavender or Dr. Jacob Temple will sit down with you and listen — actually listen — to the full story. When did the episodes start? What triggers them? How often? Any history of concussion, whiplash, a car accident, a sports injury, a hard fall, or a difficult birth? Any other autonomic symptoms (POTS-like, dizziness, GI, migraines, anxiety)? This is the most important data we collect.
2. 3D CBCT imaging. We use cone beam computed tomography to capture a true three-dimensional image of your upper cervical spine. Standard 2D X-rays simply can’t show the subtle three-plane misalignments that matter at C1 and C2. CBCT lets us measure your spine down to fractions of a millimeter and design a correction unique to your anatomy.
3. Functional nervous system scans. Tytron infrared thermography assesses autonomic patterns along your spine, giving us objective data on how your nervous system is functioning and a baseline to compare future visits to.
4. A precise, gentle correction. No twisting. No cracking. No popping. The adjustment uses only as much force as is needed to nudge the atlas back into its optimal position — often less pressure than checking a pulse. Most patients describe it as anticlimactic in the best possible way.
5. Post-correction checks. We re-scan, reassess, and track how your body is holding the correction over time. Stability — not constant adjusting — is the goal.
Why This Helps Vasovagal Syncope Specifically
When the atlas and axis return to a healthy, neutral position:
- Mechanical tension around the brainstem and vagus nerve eases.
- Vascular flow through the vertebral arteries and jugular veins normalizes.
- Proprioceptive input from the upper neck stops “lying” to the brainstem.
- The baroreflex — the body’s main defense against orthostatic blood pressure drops — can recalibrate.
- Sympathetic and parasympathetic tone start to rebalance.
The result, for many patients, is a reduction in the frequency and severity of episodes, fewer near-faints, less anticipatory anxiety, and a nervous system that handles heat, standing, stress, and other classic triggers without crashing.
Ready to see if upper cervical care can help your fainting episodes? Call us at (941) 243-3729 or schedule a complimentary consultation online: https://intake.chirohd.com/new-patient-scheduling/724/lavender-family-chiropractic. We are at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield, easy to reach from anywhere in Sarasota, Lakewood Ranch, or Bradenton.
What the Research Says About Vasovagal Syncope, the Vagus Nerve, and the Upper Cervical Spine
The body of research on vasovagal syncope is substantial, and the picture that emerges is consistent with what we observe clinically.
A landmark review on the pathophysiology of the vasovagal response describes the syncope event as a four-phase progression — early stabilization, circulatory instability, terminal hypotension, and recovery — driven by a combination of falling cardiac output and inappropriate vasodilation. The authors note that older models overstated vasodilation as the dominant mechanism; modern continuous monitoring shows that a steep fall in cardiac output is actually a primary driver in many patients (Pathophysiology of vasovagal syncope — PubMed).
A second peer-reviewed review focused on new pharmacological treatment approaches describes the central role of cardiac C-fiber afferents, abnormal sympathetic-parasympathetic crosstalk, and the role of neurotransmitters like serotonin in vasovagal episodes. It also acknowledges that existing pharmacological treatments (beta-blockers, midodrine, fludrocortisone, SSRIs) have inconsistent efficacy and that the search for better treatments continues (Pathophysiology of Vasovagal Syncope and New Approaches to its Pharmacological Treatment — PubMed).
That’s an important admission: standard medical care doesn’t have a reliable solution for recurrent vasovagal syncope. Beta-blockers help some patients but not others. SSRIs sometimes help. Pacemakers are reserved for severe cardioinhibitory cases. Lifestyle counseling (“drink more water, avoid triggers, do leg crossing maneuvers”) is the most universally recommended advice — and it’s helpful, but it doesn’t address the underlying neurological irritability that lets these episodes happen so easily in the first place.
This is exactly the gap upper cervical chiropractic care addresses. By targeting the mechanical environment around the brainstem and vagus nerve — the very structures whose dysfunction drives vasovagal episodes — we work with the root contributors rather than only managing symptoms.
While large randomized trials specifically on upper cervical chiropractic and vasovagal syncope are still limited, the supporting science around upper cervical alignment, vagus nerve function, baroreflex regulation, and cerebral perfusion is robust. The Wikipedia article on the vagus nerve and on reflex syncope both make it clear that the vagus nerve’s parasympathetic outflow is the primary mediator of vasovagal events, and the vagus nerve’s anatomy runs directly through the upper cervical region.
If your nervous system is the orchestra and the vagus nerve is the conductor’s baton, the upper cervical spine is the stage. When the stage tilts, the music falls apart.
Lifestyle and Daily Habits That Support Your Recovery
Upper cervical care does the heavy lifting at the structural and neurological level — but what you do between visits matters. These are the lifestyle anchors we recommend for vasovagal patients in Sarasota and Lakewood Ranch:
Hydration. Florida heat is brutal on blood volume. Aim for half your body weight in ounces of water daily as a baseline, more if you’re outdoors. Adding electrolytes (sodium especially — 2 to 3 grams above your normal intake unless you have blood pressure or kidney concerns) helps the body hold onto fluid and keep blood pressure stable on standing.
Salt intake. Counterintuitive but well-supported. Most vasovagal patients run on the low end of normal blood pressure, and modest sodium loading helps. Talk to your provider first if you have hypertension or kidney issues.
Compression. Knee-high or thigh-high compression socks reduce venous pooling in the legs — the same pooling that triggers many vasovagal episodes. Game-changer for nurses, teachers, retail workers, hairstylists, and anyone who stands all day.
Physical counter-pressure maneuvers. When you feel the prodrome (warmth, nausea, gray vision), cross your legs and squeeze, clench your fists, tense your arm muscles, or sit/squat immediately. These maneuvers push blood back to the brain and can abort an episode.
Sleep and stress. Sympathetic-dominant nervous systems are more prone to vasovagal events. Prioritize sleep, daily walks, breathwork, and stress reduction. The vagus nerve responds to slow, deep, diaphragmatic breathing.
Exercise — carefully. Recumbent biking, swimming, and rowing build cardiovascular tolerance without the orthostatic challenge of running. Gradually reintroduce upright exercise as your tolerance grows.
Watch your triggers. Heat, dehydration, alcohol, skipped meals, prolonged standing, hot showers, and emotionally overwhelming situations are the usual suspects. Awareness lowers risk.
Address the autonomic picture as a whole. Vasovagal syncope rarely lives alone. Many of our patients also deal with POTS-like symptoms, dizziness, migraines, brain fog, or GI issues. If that sounds like you, our deep dive into dysautonomia and POTS and the atlas-vagus connection is worth reading — it’s the same autonomic system that drives all of these symptoms.
These habits don’t replace addressing the structural cause. They support it. Patients who combine lifestyle work with consistent upper cervical care tend to see the biggest, most durable changes.
Serving Sarasota, Lakewood Ranch, and the Surrounding Communities
Lavender Family Chiropractic is located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — right at the corner of University and Whitfield, just minutes from both Sarasota and Lakewood Ranch. We’re a quick drive whether you’re coming from downtown Sarasota, UTC, west Bradenton, Parrish, or further out.
We proudly serve patients from Sarasota, Lakewood Ranch, Bradenton, Parrish, Ellenton, Venice, Osprey, Punta Gorda, St. Petersburg, Siesta Key, Longboat Key, Lido Key, and Myakka City. Many patients drive an hour or more for this style of care because precision upper cervical work is rare — there are only a handful of practices nationwide trained at this level of specificity.
Whether you’ve searched “vasovagal syncope specialist near me,” “fainting doctor Sarasota,” “vagus nerve chiropractor Lakewood Ranch,” or “upper cervical chiropractor near me,” you’ve landed in the right place. Our two-doctor team — Dr. Rusty Lavender and Dr. Jacob Temple — has helped hundreds of patients in Southwest Florida find relief from fainting episodes, dizziness, POTS, vertigo, migraines, and the broader autonomic dysregulation that often comes with them.
Top 15 Frequently Asked Questions About Vasovagal Syncope and Upper Cervical Chiropractic
1. Is vasovagal syncope dangerous?
The fainting episode itself is rarely life-threatening, but the fall that comes with it can cause serious injuries — concussions, fractures, lacerations. And the cumulative impact on quality of life, driving, exercise, and confidence is significant. Recurrent syncope is worth taking seriously, even if your medical workup has been “normal.”
2. How is vasovagal syncope diagnosed?
It’s usually a clinical diagnosis based on your history. Your cardiologist may run an EKG, echocardiogram, Holter monitor, tilt table test, and bloodwork primarily to rule out more dangerous causes of fainting (arrhythmias, structural heart disease, seizures, hypoglycemia). When all of that comes back normal and the pattern fits, vasovagal syncope is the diagnosis.
3. What’s the difference between vasovagal syncope and POTS?
POTS (Postural Orthostatic Tachycardia Syndrome) is a sustained, exaggerated heart rate rise on standing, usually without full fainting. Vasovagal syncope is a sudden, brief episode of fainting triggered by specific stimuli. They share underlying autonomic dysregulation and frequently coexist. Our POTS doctor in Sarasota guide goes deep on this connection.
4. Can upper cervical chiropractic actually help vasovagal syncope?
It addresses the structural and neurological environment around the brainstem and vagus nerve — the exact circuit involved in vasovagal episodes. We’ve seen patients go from multiple monthly episodes to none, but every nervous system is different. Our complimentary consultation is the right way to find out if you’re a good candidate.
5. Will I have to get my neck “cracked”?
No. Upper cervical chiropractic at Lavender Family Chiropractic uses precise, gentle corrections with no twisting, popping, or cracking. Many patients describe it as so gentle they’re surprised anything happened — until they start to feel different.
6. How long until I notice a change?
It varies. Some patients feel different within a few visits; others notice changes over weeks to a few months. Recurrent vasovagal episodes generally reflect a nervous system that’s been irritable for a long time, and giving the system time to settle is part of the process.
7. Do I need to keep coming in forever?
No. The goal is stability — your spine holding alignment longer and longer without needing correction. Most patients move from a more frequent corrective phase into spaced-out wellness visits as their nervous system stabilizes.
8. Is upper cervical care safe?
Yes, when performed by a trained, certified upper cervical doctor with proper imaging. The forces used are very low. There’s no high-velocity manipulation of the neck. Dr. Lavender and Dr. Temple are both rigorously trained and use 3D CBCT imaging to ensure every correction is precise.
9. What if I’ve had a whiplash or concussion in the past?
This is one of the most common patterns we see with vasovagal patients. A whiplash injury, a sports concussion, a hard fall — these events can destabilize the upper cervical spine and set up the nervous system for years of dysfunction. CBCT imaging often reveals the structural legacy of these injuries.
10. Do I need a referral?
No. You can schedule a complimentary consultation directly with our office.
11. Will my insurance cover this?
Lavender Family Chiropractic is out of network with insurance. We’ve found this lets us spend the time and use the technology that this kind of precision care requires. We’re happy to discuss costs transparently at your consultation.
12. Can children or teens with vasovagal syncope be helped?
Yes. Vasovagal syncope often shows up first in adolescence and tends to run in clusters across someone’s life. Our care is gentle enough for kids and teens, and addressing it early can change the trajectory.
13. What if I also have anxiety about fainting?
Anticipatory anxiety is part of the vasovagal pattern for many patients — and the anxiety itself becomes a trigger. As the underlying autonomic balance improves with care, that anxious loop tends to quiet down too.
14. Should I stop my medications?
No — never stop or change prescribed medications without talking to your prescribing doctor. Upper cervical care complements medical care. As you stabilize, your physician may decide to adjust medications based on your improving picture.
15. How do I get started?
Call (941) 243-3729 or book online at https://intake.chirohd.com/new-patient-scheduling/724/lavender-family-chiropractic. Your first consultation is complimentary — it’s a no-pressure conversation about whether this care is right for you.
Take the Next Step
Living with vasovagal syncope shouldn’t mean rearranging your entire life around the next episode. If you’ve been told everything looks normal, that you just need to drink more water and avoid your triggers, and you’re still fainting, still anxious, still planning your days around the fear of the next near-faint — there is more that can be looked at.
The upper cervical spine is one of the most overlooked structures in the standard syncope workup, and yet it sits at the exact junction of every system involved in a vasovagal episode: the brainstem, the vagus nerve, the baroreflex circuit, and the major blood vessels feeding the brain. Restoring proper alignment there gives your nervous system a real chance to settle.
At Lavender Family Chiropractic in Sarasota and Lakewood Ranch, Dr. Rusty Lavender and Dr. Jacob Temple offer a complimentary consultation so you can ask your questions, share your story, and find out whether upper cervical care is a fit for you. No pressure, no commitment — just a conversation and an honest assessment.
Lavender Family Chiropractic 5899 Whitfield Avenue, Suite 107 Sarasota, FL 34243 (corner of University and Whitfield) Phone: (941) 243-3729 Book online: https://intake.chirohd.com/new-patient-scheduling/724/lavender-family-chiropractic
You don’t have to keep living one episode away from the floor. Real answers are possible — and they often start at the top of your neck.
Related Articles
- Vagus Nerve Dysfunction, Craniocervical Instability, and Upper Cervical Chiropractic Care in Sarasota, Florida
- Dysautonomia and POTS in Sarasota: The Atlas–Vagus Connection and How Upper Cervical Chiropractic Can Resolve Symptoms Quickly
- How to Resolve Dysautonomia: Real Answers and Proven Results from Upper Cervical Chiropractors in Sarasota
By the team at Lavender Family Chiropractic — Dr. Rusty Lavender and Dr. Jacob Temple — 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243
Related Posts
Popular Posts
