
Orthostatic Hypotension: You stand up from the couch, the kitchen table, or the edge of the bed — and the room narrows. Your vision goes gray. You grab the wall. Your heart pounds. Sometimes you sit back down quickly. Sometimes you don’t make it, and you wake up on the floor wondering what just happened.
If that sounds familiar, you may be living with orthostatic hypotension — a condition where your blood pressure drops too far, too fast, when you change position. It is closely tied to POTS, dysautonomia, vasovagal syncope, and a whole family of autonomic nervous system problems that we see in our Sarasota and Lakewood Ranch office every single week.
If you have already read our deep-dive guide on Dysautonomia and POTS in Sarasota, think of this article as the companion piece — the missing chapter that focuses on the blood pressure side of the equation. POTS gets the attention because of the dramatic heart rate spike. Orthostatic hypotension is its quieter, more dangerous cousin — the one that drops you to the floor without warning.
At Lavender Family Chiropractic, Dr. Rusty Lavender and Dr. Jacob Temple have spent years helping patients with this exact problem. Our approach is gentle, precise, and rooted in the relationship between the top of your neck and the autonomic nervous system that runs your blood pressure. In the next several thousand words, we are going to walk you through what orthostatic hypotension really is, why it happens, why traditional treatments often fall short, and why so many patients in Sarasota, Bradenton, Lakewood Ranch, and Manatee County are finding lasting answers through upper cervical chiropractic care.
What Is Orthostatic Hypotension?
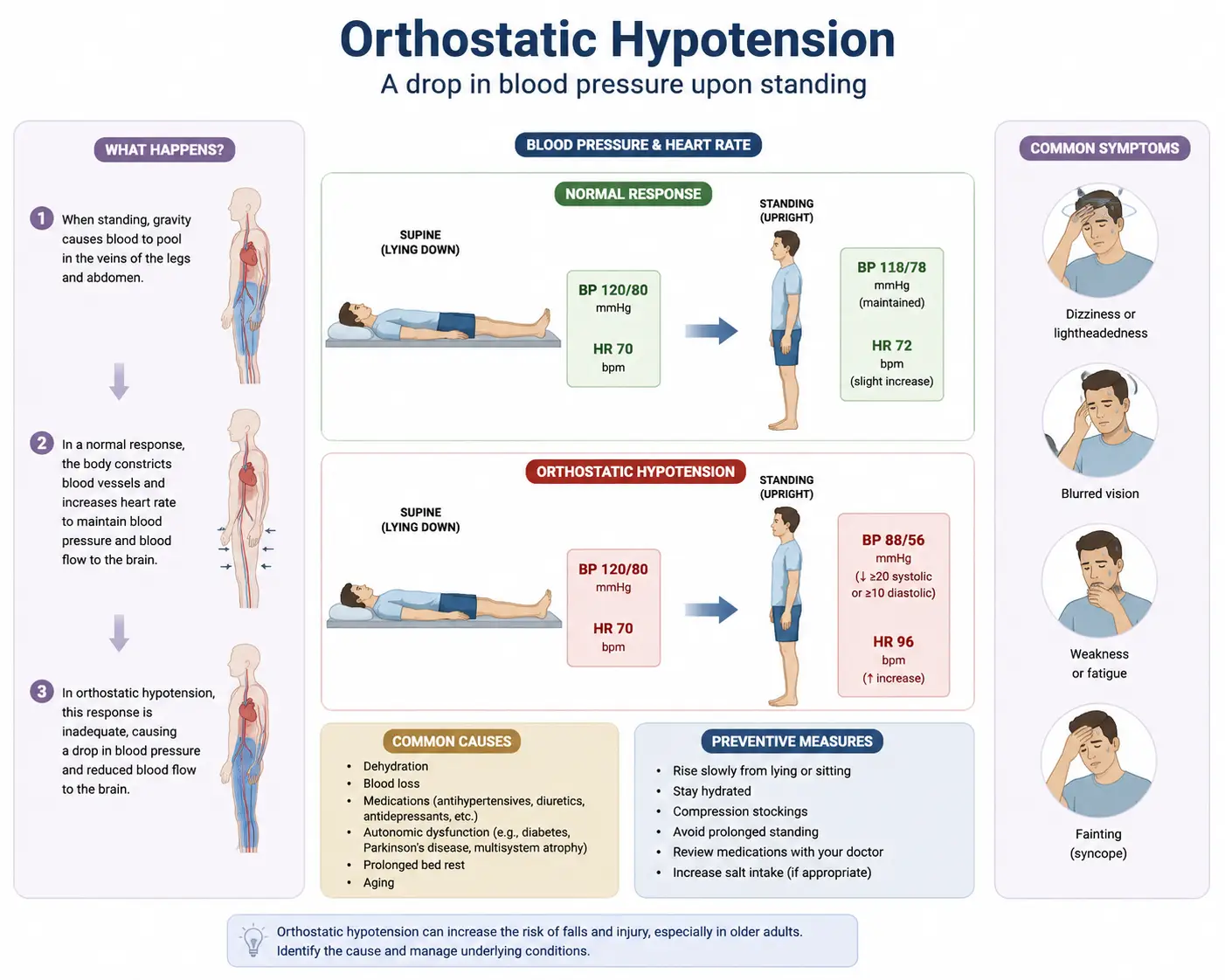
Orthostatic hypotension (OH), sometimes called postural hypotension, is defined as a drop in blood pressure that happens when you move from lying down or sitting to standing up. The clinical definition is specific: a fall of at least 20 mmHg in systolic blood pressure or 10 mmHg in diastolic blood pressure within three minutes of standing.
In plain English, gravity pulls 500 to 1,000 mL of blood downward into your legs and abdomen the moment you stand. A healthy autonomic nervous system reacts instantly — it constricts blood vessels in the lower body, increases heart rate slightly, and pushes blood back up to the brain. The whole compensation should happen within seconds, before you even notice it.
When that compensation fails or lags, blood pools below the waist. Your brain temporarily runs short on oxygen and glucose. The result is a cascade of symptoms that anyone with OH knows intimately:
- Dizziness or lightheadedness on standing
- Blurred or “tunnel” vision
- Graying out or near-fainting
- Actual fainting (syncope)
- Weakness in the legs
- Confusion or brain fog
- Nausea
- Headache (often felt at the base of the skull)
- Generalized fatigue throughout the day
- Sometimes — paradoxically — chest pain or palpitations as the heart tries to compensate
Some people only feel this in the morning when they first get out of bed. Others experience it every time they stand from a chair, get up from the toilet, or rise after a meal. Severe cases can lead to falls, fractures, head injuries, and a steady erosion of confidence in your own body.
Orthostatic Hypotension Is a Sign, Not a Disease
This is one of the most important things to understand, and one of the most overlooked. Orthostatic hypotension is not a disease in itself — it is a signal that something is wrong with the way your autonomic nervous system regulates blood pressure.
A landmark JACC State-of-the-Art Review published in the Journal of the American College of Cardiology makes this point clearly. The authors explain that orthostatic hypotension is due to impairment of baroreflex-mediated vasoconstriction of the skeletal muscle and splanchnic circulation and is caused by damage or dysfunction at central and/or peripheral sites in the baroreflex efferent pathway. They also note that nonpharmacological and pharmacological interventions may be implemented to ameliorate the symptoms of orthostatic intolerance and improve quality of life, with treatment typically progressing from education and lifestyle changes to volume repletion and finally sympathomimetic agents in more severe cases. PubMedPubMed
A second comprehensive review in Hellenic Journal of Cardiology echoes this, summarizing that orthostatic hypotension has been extensively studied and numerous prospective cohort studies support its association with adverse events, including coronary artery disease, heart failure, stroke, cognitive dysfunction, and, most importantly, mortality rates. In other words, OH is not just inconvenient — it is a marker of broader autonomic dysfunction with real long-term consequences if left unaddressed. PubMed
If you want to read the original research, both papers are open on PubMed:
- Orthostatic Hypotension: JACC State-of-the-Art Review (PMID 30190008)
- Orthostatic hypotension: From pathophysiology to clinical applications and therapeutic considerations (PMID 30900378)
This is why our office takes orthostatic hypotension seriously. We are not chasing the dizziness — we are looking for the underlying neurological reason your body cannot regulate blood pressure properly when you change position.
The Baroreflex: Your Body’s Built-In Blood Pressure Thermostat
To understand why orthostatic hypotension happens, you need to understand the baroreflex. This is one of the most elegant reflexes in the human body, and it is the system that fails when OH develops.
Inside the walls of your carotid arteries (in your neck) and your aortic arch (just above your heart), there are stretch receptors called baroreceptors. These tiny sensors monitor blood pressure continuously, hundreds of times a minute. When you stand up and blood pressure drops, the baroreceptors detect the change instantly and send signals up the vagus nerve and glossopharyngeal nerve into the brainstem — specifically into a region called the nucleus tractus solitarius (NTS).
From there, the brainstem orchestrates a beautifully coordinated response:
- Sympathetic activation — blood vessels in the legs and gut constrict to push blood upward.
- Parasympathetic withdrawal — the vagus nerve eases off the brakes on the heart so heart rate can rise.
- Hormonal support — norepinephrine, renin, and aldosterone get released to maintain volume and tone.
All of this happens in under three seconds in a healthy person. You barely notice you stood up.
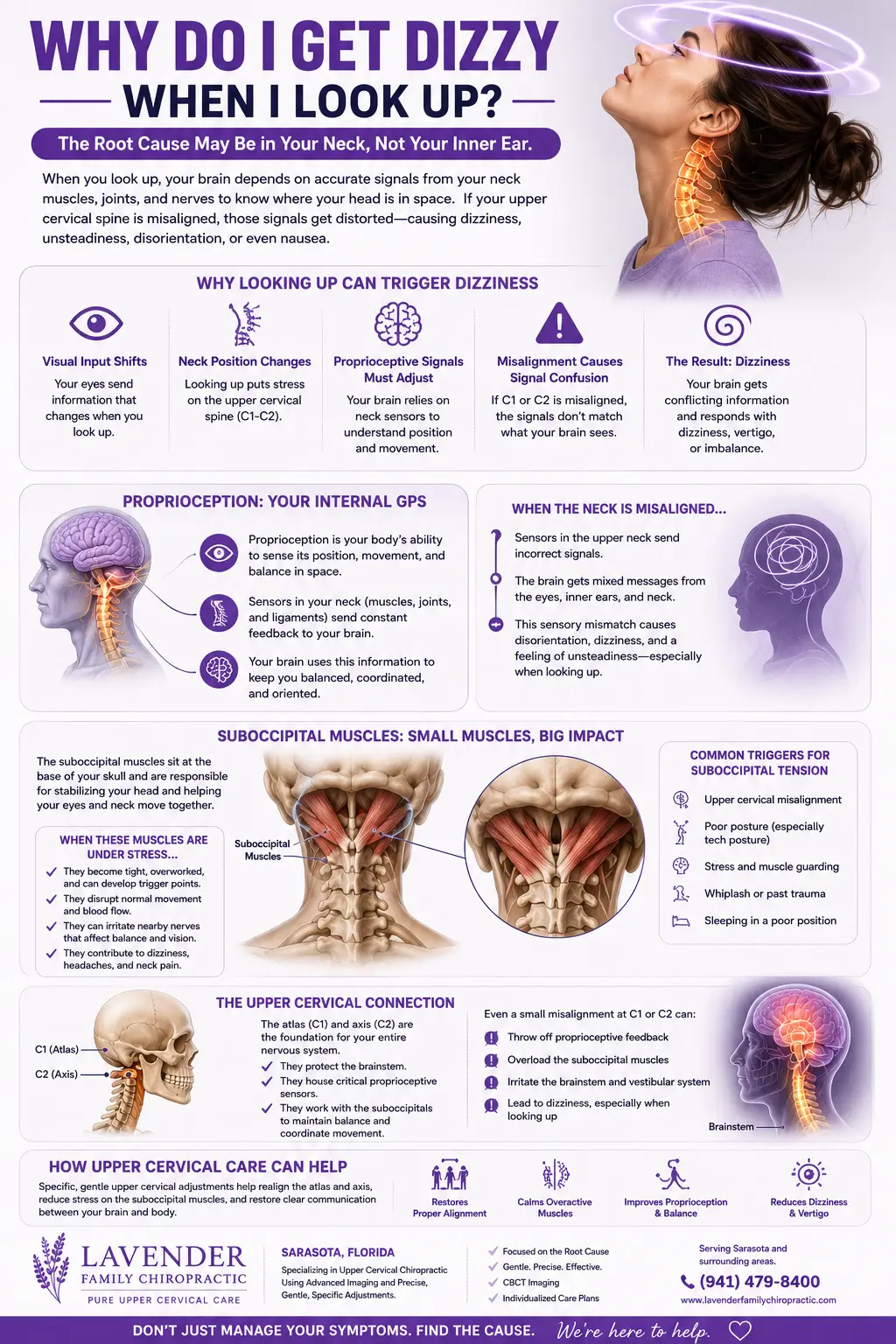
But notice where this reflex lives: the brainstem. The same brainstem that sits inside the protective ring of your atlas (C1) and axis (C2) vertebrae — the top two bones of your neck. If those bones are even slightly misaligned, the entire control circuit for your blood pressure can be operating at less than full capacity.
The Upper Cervical Spine and Autonomic Blood Pressure Regulation
Here is the part most patients with orthostatic hypotension have never heard about, and it is the part that often changes everything.
The atlas (C1) is a uniquely shaped vertebra that cradles the base of your skull. The axis (C2) sits just below it. Together, these two bones surround the lower brainstem — the exact region that contains the cardiovascular control centers, including the nucleus tractus solitarius, the nucleus ambiguus (which gives rise to the vagus nerve fibers that slow the heart), and the rostral ventrolateral medulla (which drives sympathetic tone to blood vessels).
The vagus nerve itself exits the skull through the jugular foramen, passes directly adjacent to the atlas, and travels down the neck wrapped in connective tissue that is mechanically linked to the upper cervical structures. The major arteries that supply blood to the brainstem — the vertebral arteries — pass through small openings in the atlas and axis called the foramina transversaria. Cerebrospinal fluid flow in and out of the skull is also dependent on free, symmetric motion at this junction.
When the atlas or axis is misaligned, even by a fraction of a millimeter, several things can happen:
- Mechanical irritation of the brainstem. Subtle pressure changes from a tilted atlas can alter how the brainstem processes incoming baroreceptor signals.
- Vagus nerve compromise. Tension or torsion at the craniocervical junction can reduce vagal tone — the very signal the baroreflex relies on to slow your heart and engage parasympathetic balance.
- Altered vertebral artery flow. When the head sits asymmetrically on the neck, blood flow to the brainstem can shift with head position. Standing up requires more brainstem blood flow, not less.
- Disrupted cerebrospinal fluid dynamics. CSF cushions and nourishes the brainstem. Restricted CSF flow can create chronic neural irritation that destabilizes autonomic output.
- Sympathetic over-drive, parasympathetic under-drive. The end result is a nervous system that lives with the gas pedal stuck on and the brake pedal weakened — exactly the imbalance seen in orthostatic hypotension, POTS, and dysautonomia.
You can read more about this whole-system relationship on our Upper Cervical Care in Sarasota and Lakewood Ranchpage, which explains in detail how we evaluate and correct this region using 3D CBCT imaging, thermography, and gentle, no-twist adjustments.
What Causes Orthostatic Hypotension in the First Place?
Conventional medicine recognizes several categories of orthostatic hypotension. Understanding these can help you make sense of where your symptoms are coming from — and why upper cervical care so often plays a role even when the diagnosis seems “purely medical.”
1. Neurogenic Orthostatic Hypotension
This is OH caused by failure of the autonomic nervous system itself. The body simply cannot generate the sympathetic response needed to keep blood pressure up when you stand. Causes include:
- Parkinson’s disease
- Multiple system atrophy (MSA)
- Pure autonomic failure
- Diabetic autonomic neuropathy
- Lewy body dementia
- Amyloidosis
- POTS and other forms of dysautonomia
- Post-viral autonomic dysfunction (including long COVID)
- Craniocervical instability and upper cervical injury
The common thread is dysfunction somewhere in the autonomic pathway — and for many patients, the upper cervical spine is the missing structural piece in that pathway.
2. Non-Neurogenic Orthostatic Hypotension
This is OH caused by something other than direct nervous system failure. Causes include:
- Dehydration
- Blood loss
- Anemia
- Heart conditions (bradycardia, valve problems, heart failure)
- Adrenal insufficiency
- Prolonged bed rest or deconditioning
3. Medication-Induced Orthostatic Hypotension
This is one of the most common — and most overlooked — causes. Many widely prescribed medications can drop blood pressure significantly on standing:
- Diuretics
- Alpha-blockers (often prescribed for prostate or blood pressure)
- Beta-blockers
- ACE inhibitors and ARBs
- Tricyclic antidepressants
- Some Parkinson’s medications
- Sedatives and opioids
If you developed orthostatic symptoms after starting a new medication, talk with your prescribing doctor. We never tell patients to stop a medication — that is between you and your physician — but recognizing the pattern matters.
4. Post-Trauma Orthostatic Dysfunction
This is the category we see most often at Lavender Family Chiropractic. Patients who have:
- Been in a car accident (even a low-speed fender-bender)
- Suffered a sports concussion
- Fallen and hit their head
- Had birth trauma or forceps delivery
- Experienced a whiplash event
- Had years of poor posture, forward head carriage, or repetitive strain
…can develop orthostatic hypotension months or years later. The mechanism is mechanical: the trauma disrupts the upper cervical alignment, the brainstem gets irritated, and autonomic regulation gradually deteriorates.
Why Standard Treatment Often Falls Short
If you have already been evaluated for orthostatic hypotension, you have likely received some combination of the following recommendations:
- “Drink more water.”
- “Eat more salt.”
- “Get up slowly.”
- “Wear compression stockings.”
- “Try midodrine.”
- “Try fludrocortisone.”
- “Try droxidopa.”
- “Sleep with the head of the bed elevated.”
These interventions can absolutely help, and we are not anti-medication. The pathophysiology review on PubMed describes the standard medical workflow well: the present review, we discuss the clinical applications associated with ΟΗ by outlining the current perspectives on ΟΗ definition, diagnosis, pathophysiology, prognostic role, and treatment. The reality is that even with optimal care, many patients remain symptomatic — because the treatments target the output (low blood pressure on standing) without ever asking why the baroreflex is malfunctioning in the first place. PubMed
That is the gap upper cervical chiropractic care is designed to fill.
How Upper Cervical Chiropractic Care Helps Orthostatic Hypotension
When patients with orthostatic hypotension come to our Sarasota office, we are not trying to replace their cardiologist, neurologist, or primary care doctor. We are trying to address a piece of the puzzle that the medical model rarely evaluates: the structural and neurological status of the craniocervical junction.
Here is what that looks like in practice.
Step 1: Listen to Your Story
Most patients with OH have been bounced between specialists for years. They have logs, tilt-table results, Holter monitors, MRIs, and a folder full of “everything looks fine.” We start by sitting down and actually hearing the timeline — when symptoms began, what events preceded them, what makes them worse, what makes them better. Triggers like head injuries, whiplash events, dental procedures, birth history, falls, and posture habits all matter.
Step 2: Functional Nervous System Scans
We use paraspinal infrared thermography (Tytron) to measure heat asymmetry along the spine, which reflects autonomic tone. We use surface EMG to assess muscle guarding around the upper cervical region. Together, these scans give us an objective, non-invasive picture of how your nervous system is functioning before we ever consider an adjustment.
Step 3: 3D CBCT Imaging (When Clinically Indicated)
Standard X-rays cannot reliably show the subtle joint geometry at C0–C1–C2. Cone Beam Computed Tomographygives us a true 3D view of how your atlas and axis are positioned relative to your skull and to each other. From those images, we can calculate exact correction vectors specific to your anatomy. This is precision care — not guesswork.
Step 4: Gentle, Precise Correction
This is where upper cervical chiropractic separates itself from everything else. There is no twisting, no popping, no cracking, no jerking. The correction is a low-force, mathematically calculated impulse delivered to a very specific point on the side of the neck, in a very specific direction, at a very specific angle. Most patients describe it as a light tap. Many patients fall asleep on the table afterward as their nervous system finally exhales.
Step 5: Monitoring and Stabilization
We track your response with follow-up thermography, symptom logs, and orthostatic vital signs over time. The goal is not to keep adjusting you forever — the goal is to restore alignment and then let it hold so your nervous system can rebuild stability on its own.
What Patients Notice as Care Progresses
Every nervous system heals at its own pace, and we never promise specific results. That said, here is what we commonly see in patients with orthostatic hypotension over weeks and months of care:
- Standing up no longer triggers an immediate gray-out
- Morning rise from bed becomes less alarming
- Brain fog clears, often dramatically
- Fewer near-fainting episodes
- Heart rate becomes more stable through position changes
- Energy returns through the afternoon, not just in the morning
- Headaches at the base of the skull soften
- GI function (digestion, motility, reflux) improves as vagal tone returns
- Sleep quality deepens
- Heat tolerance and exertion tolerance expand
- Confidence in daily activities — driving, shopping, walking the dog — comes back
These are not isolated benefits. They are all expressions of the same thing: an autonomic nervous system that is finally being allowed to do its job.
A Quick Word on What to Expect From Your First Visit
Many patients are nervous about chiropractic care, especially those with autonomic conditions who have been told to avoid “neck cracking.” We hear you. Upper cervical care at Lavender Family Chiropractic is not what people picture when they think of chiropractic. There is no full-spine twisting. There is no aggressive manipulation. There is no rough handling of your already-sensitive nervous system.
Your first visit is a conversation, an examination, scans, and (when indicated) imaging. You will not be adjusted on the first visit. We need to know exactly what we are doing before we touch your spine. That is the whole point of being specific.
If you would like to read more about how the craniocervical junction influences not just blood pressure but the entire parasympathetic system, our blog on Vagus Nerve Dysfunction and Upper Cervical Chiropractic Care goes deeper into the connection between brainstem irritation and chronic autonomic symptoms.
📞 Ready to find out if upper cervical care can help your orthostatic hypotension? Call Lavender Family Chiropractic in Sarasota at (941) 243-3729 or book your complimentary consultation online. No pressure, no commitment — just a real conversation with doctors who understand autonomic dysfunction.
The Research Behind the Connection
We want to be honest about where the science currently stands. Research specifically on upper cervical chiropractic care for orthostatic hypotension is still emerging — large randomized controlled trials don’t yet exist for this exact intervention. But the research on the pathophysiology of OH points squarely at the autonomic nervous system, and the autonomic nervous system is anatomically inseparable from the structures we work with.
The JACC State-of-the-Art Review summarizes that orthostatic hypotension is due to impairment of baroreflex-mediated vasoconstriction of the skeletal muscle and splanchnic circulation and is caused by damage or dysfunction at central and/or peripheral sites in the baroreflex efferent pathway. The central sites of that pathway are in the brainstem. The brainstem is housed inside the atlas and axis. When alignment and motion at the craniocervical junction are optimized, the central baroreflex circuitry has the best possible mechanical and vascular environment in which to function. PubMed
The broader pathophysiology review emphasizes that orthostatic hypotension has been extensively studied and numerous prospective cohort studies support its association with adverse events, including coronary artery disease, heart failure, stroke, cognitive dysfunction, and, most importantly, mortality rates. This is not a “nuisance” diagnosis — it is a marker of meaningful autonomic dysfunction with long-term consequences. Addressing the structural drivers of that dysfunction matters. PubMed
Lifestyle Strategies That Support Upper Cervical Care for OH
Care in our office is one piece of recovery. The rest is what you do between visits. Patients who combine upper cervical correction with thoughtful lifestyle adjustments tend to recover the fastest and stay the most stable.
Hydration and Electrolytes
Most OH patients are subtly dehydrated. Aim for 2.5–3 liters of fluid daily with a real electrolyte source (not just sugary “sports drinks”). Sodium is often friend, not foe, in OH — but discuss salt loading with your physician, especially if you have hypertension or kidney disease.
Slow Position Changes
Sit on the edge of the bed for 60 seconds before standing. Pump your calves a few times before rising. Cross your legs and squeeze when you feel symptoms coming on — this pushes blood back upward.
Compression Garments
Knee-high or thigh-high compression stockings (20–30 mmHg) and abdominal binders can reduce venous pooling. Many patients hate them initially and love them within two weeks.
Sleep Position
Slightly elevating the head of the bed (4–6 inches) reduces nighttime supine hypertension and trains the kidneys to retain more volume.
Movement Recovery
Gentle, gravity-respecting exercise — recumbent bike, swimming, supine resistance training — rebuilds cardiovascular tone without provoking symptoms. Avoid prolonged standing in the heat.
Posture and Screen Habits
Forward head carriage adds mechanical load to the very structures we are trying to stabilize. Keep screens at eye level. Take micro-breaks every 30–45 minutes.
For a complete deep dive into autonomic rehabilitation strategies and how they pair with upper cervical care, see our companion blog How to Resolve Dysautonomia: Real Answers and Proven Results from Upper Cervical Chiropractors in Sarasota.
Who We Serve in Sarasota, Manatee, and Beyond
Lavender Family Chiropractic is located at the corner of University and Whitfield in Sarasota, Florida, and we serve patients from across Southwest Florida — including Bradenton, Lakewood Ranch, Parrish, Ellenton, Venice, Osprey, Siesta Key, Longboat Key, Lido Key, Myakka City, Punta Gorda, and St. Petersburg. Patients also fly in from across the country for evaluation when local care has run out of answers.
Whether you are searching for “POTS doctor near me,” “chiropractor near me,” “upper cervical chiropractor near me,” “dysautonomia doctor near me,” or “orthostatic hypotension treatment near me” — you are in the right place.
Top 15 Frequently Asked Questions About Orthostatic Hypotension and Upper Cervical Care
1. What is the difference between orthostatic hypotension and POTS?
Both are forms of orthostatic intolerance. POTS is defined by a heart rate increase of 30+ beats per minute within 10 minutes of standing, usually without a big blood pressure drop. OH is defined by a blood pressure drop of 20 mmHg systolic (or 10 mmHg diastolic) within 3 minutes of standing. Many patients have features of both.
2. Can orthostatic hypotension be cured?
It depends entirely on the underlying cause. Medication-induced OH often resolves when medications are adjusted. Trauma-induced or autonomic dysregulation OH often responds dramatically to upper cervical correction. Neurodegenerative OH (Parkinson’s, MSA) is harder to reverse but symptoms can still be improved.
3. Is upper cervical chiropractic safe for someone with autonomic problems?
Yes — when done correctly. Upper cervical adjustments are low-force, image-guided, and specifically designed for fragile nervous systems. There is no twisting or popping. Patients with POTS, OH, EDS, and craniocervical instability tolerate this care extremely well.
4. How long until I feel a difference?
Some patients feel changes within the first few visits. Others take 4–12 weeks of consistent care to notice durable shifts. Severity, duration of symptoms, and overall health all play a role.
5. Do I need to stop my blood pressure medications?
Never adjust medications without your prescribing doctor. As care progresses and your nervous system regulates better, your physician may decide to adjust prescriptions. That decision is theirs, not ours.
6. Will insurance cover this?
We are out of network with insurance. We provide superbills you can submit for reimbursement, and we offer payment plans. Many patients find the investment more than worthwhile after years of failed conventional care.
7. Do you treat children with orthostatic problems?
Yes. Adolescent OH and POTS are increasingly common, often post-viral. Our care is gentle enough for children and seniors alike.
8. What if I have already had spinal surgery?
That does not disqualify you from care. We adapt our protocols based on imaging and clinical history. Many post-surgical patients still have upper cervical issues that were never addressed.
9. How is this different from regular chiropractic?
Regular chiropractic typically uses manual thrust adjustments across the full spine. Upper cervical care focuses exclusively on C1 and C2, uses precise imaging and measurement, and applies gentle, specific corrections without twisting or popping.
10. Can stress cause orthostatic hypotension?
Chronic stress can shift the autonomic balance toward sympathetic dominance and weaken vagal tone, which absolutely contributes to orthostatic instability. Care that calms the brainstem helps the whole system.
11. Do I need an MRI before being seen?
Not necessarily. We use 3D CBCT imaging in our office when clinically indicated. If your case requires an MRI for soft tissue evaluation, we can coordinate with your physician.
12. What if I have a connective tissue disorder like EDS?
Patients with Ehlers-Danlos Syndrome and hypermobility spectrum disorders are often the best candidates for upper cervical care precisely because they have craniocervical instability driving their autonomic symptoms. Our gentle approach is specifically suited for these cases.
13. Can long COVID cause orthostatic hypotension?
Yes. Post-viral autonomic dysfunction — including OH, POTS, and vagal nerve impairment — is one of the hallmarks of long COVID. We have seen meaningful improvements in this population.
14. How often will I need to come in?
Initial care is typically more frequent (1–3 times per week) and tapers as your alignment stabilizes. Many patients move to maintenance visits every 4–8 weeks once they hold their correction well.
15. What if I am not sure upper cervical care is right for me?
That is exactly what a complimentary consultation is for. We sit down with you, hear your story, look at your scans, and tell you honestly whether we think we can help. If we do not think you are a good candidate, we will tell you and refer you appropriately.
A Final Word — You Are Not Imagining This
If you have been living with orthostatic hypotension, you have probably been told some version of “your tests look normal” or “this is just anxiety” or “drink more water.” You know your body. You know something is wrong. And you are right.
Orthostatic hypotension is a real, measurable dysfunction of the autonomic nervous system — and the autonomic nervous system runs through the top of your neck. When that region is calm, aligned, and properly mobile, the whole baroreflex circuit has its best chance to work the way it was designed.
At Lavender Family Chiropractic, Dr. Rusty Lavender and Dr. Jacob Temple have spent thousands of hours becoming experts in upper cervical correction because we have watched it change lives — including the lives of patients who had given up hope. We would be honored to listen to your story too.
You don’t have to keep holding onto walls. You don’t have to keep dreading the moment you stand up. There is a path forward, and it often starts at the very top of your neck.
📞 Call us today at (941) 243-3729 or book your complimentary consultation online.
Lavender Family Chiropractic 5899 Whitfield Avenue, Suite 107 Sarasota, FL 34243 (corner of University and Whitfield)
Related Articles
- Dysautonomia and POTS in Sarasota: The Atlas–Vagus Connection and How Upper Cervical Chiropractic Can Resolve Symptoms Quickly
- Vagus Nerve Dysfunction, Craniocervical Instability, and Upper Cervical Chiropractic Care in Sarasota, Florida for Proven Results
- How to Resolve Dysautonomia: Real Answers and Proven Results from Upper Cervical Chiropractors in Sarasota
Related Posts
Popular Posts
