By Dr. Rusty Lavender
Mast Cell Activation Syndrome: If you have ended up reading about mast cell activation syndrome, chances are you have been on a long, frustrating road. You have been told you have allergies that do not test as allergies. You react to foods, smells, medications, weather changes, temperature shifts, alcohol, stress, exercise, hormones — and sometimes for no reason you can identify at all. Your symptoms jump between systems and seem to make no sense — flushing one week, gastrointestinal storms the next, brain fog and palpitations and skin reactions and migraines and full-body fatigue that no test seems to explain. You have probably been told that it is anxiety, that it is in your head, that you are overreacting. You have probably also been told, by someone in a Facebook group or by a functional medicine practitioner, that you might have MCAS.
At Lavender Family Chiropractic in Sarasota, Florida, we see patients with diagnosed and suspected MCAS regularly. These patients are some of the most complex, sensitive, and undertreated in modern medicine, and many of them also carry diagnoses of POTS, hypermobility spectrum disorder, Ehlers-Danlos syndrome, chronic fatigue, fibromyalgia, or simply a long list of unexplained symptoms that nobody has been able to organize into a coherent picture. What most of them have not been told is that the upper cervical spine — and specifically the relationship between the atlas, the brainstem, and the vagus nerve — plays a meaningful role in the autonomic and immune dysregulation that drives mast cell instability, and that addressing that relationship can change the trajectory of their condition.
This guide is for anyone in Sarasota, Bradenton, Lakewood Ranch, or the surrounding areas who has been diagnosed with MCAS, suspects they have MCAS, or has been told they have a “histamine intolerance” or “idiopathic” reactions that nobody can quite explain. Through the precise, gentle Knee Chest Upper Cervical technique used by Dr. Rusty Lavender and Dr. Jacob Temple, we work to support the autonomic regulation that influences mast cell behavior — an angle that almost no other provider in your medical workup has considered.
What Is Mast Cell Activation Syndrome?
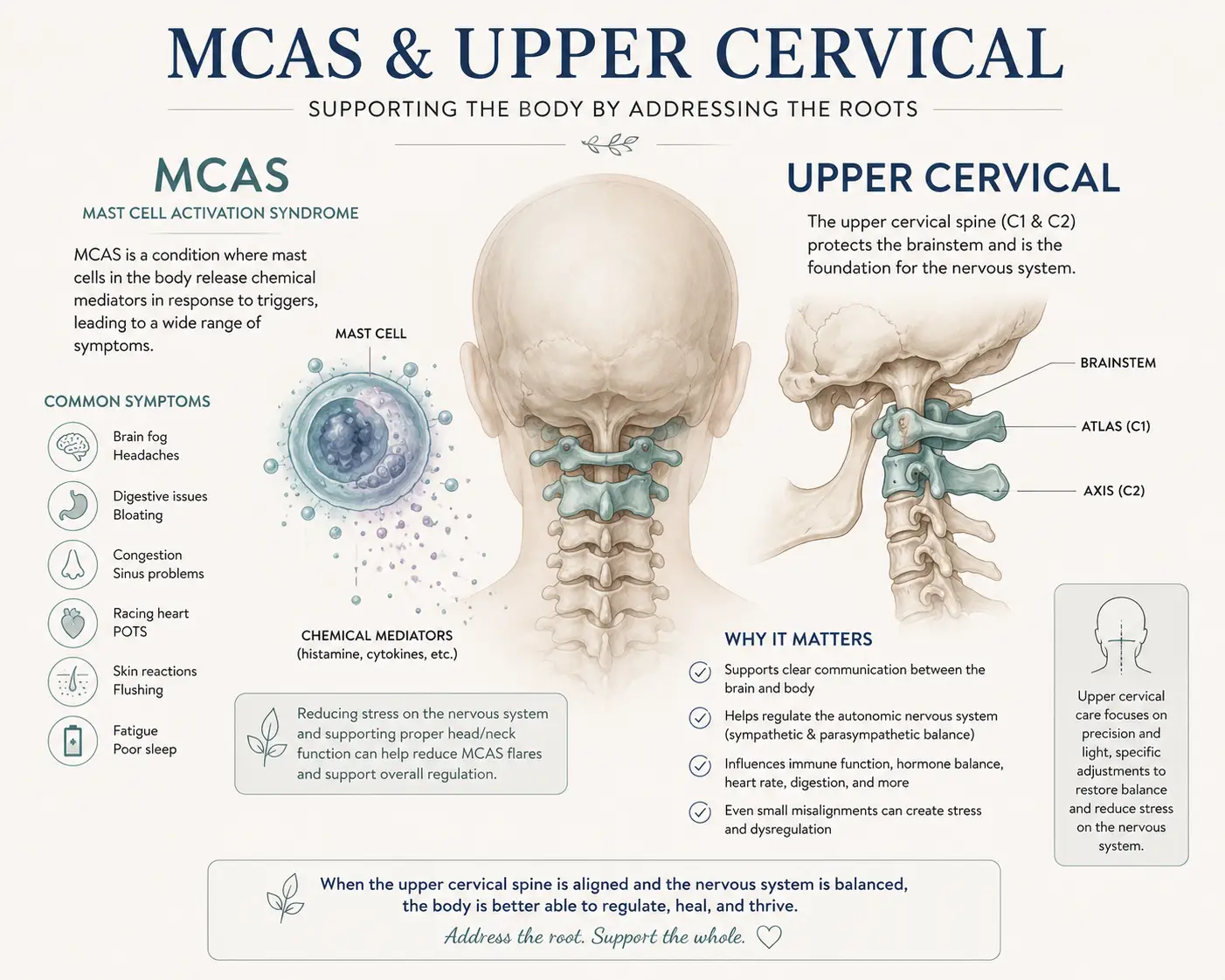
Mast cell activation syndrome is a condition in which mast cells — a type of immune cell found throughout the body’s connective tissues, particularly at the interfaces between the body and the outside world (skin, gut, lungs, sinuses) — become inappropriately reactive and release excessive amounts of inflammatory mediators in response to triggers that should not provoke a significant immune response.
Mast cells are normally one of the body’s frontline defenders. They are loaded with granules containing histamine, tryptase, prostaglandins, leukotrienes, cytokines, heparin, and dozens of other signaling molecules that, when released appropriately, mount a fast and effective response to allergens, parasites, and injury. The problem in MCAS is not that mast cells exist or that they release mediators — it is that they release them in response to triggers that should not be perceived as threats, in volumes that produce systemic symptoms, and in patterns that affect multiple organ systems simultaneously.
The current consensus diagnostic criteria for MCAS, updated in 2022 and detailed in a 2024 review in the Journal of Allergy and Clinical Immunology, require three conditions to be met: recurrent severe systemic symptoms involving at least two organ systems, a measurable transient increase in a validated marker of mast cell activation during an episode (typically serum tryptase), and a clinical response to medications that target mast cells or their mediators. The diagnostic process is difficult, the testing window is narrow, and most patients with suspected MCAS do not formally meet these strict criteria — which is part of why this condition is so contentious in mainstream medicine and so frustrating for patients.
The symptom picture is famously wide. Patients may experience skin symptoms (flushing, hives, dermatographism, itching), gastrointestinal symptoms (nausea, abdominal pain, bloating, diarrhea, food reactions), respiratory symptoms (nasal congestion, throat tightness, wheezing, shortness of breath), cardiovascular symptoms (palpitations, dizziness on standing, blood pressure swings), neurological symptoms (brain fog, anxiety, migraines, sensory sensitivities), and constitutional symptoms (fatigue, temperature dysregulation, sleep disturbance). Episodes can be triggered by foods, medications, heat, cold, exercise, stress, hormonal shifts, scents, mold exposure, infections, or no identifiable trigger at all.
How common is MCAS? This is one of the most contested questions in the field. Suggested prevalence figures have ranged as high as 17% of the population, but a rigorous 2024 Swedish cohort study of 703 patients referred for suspected MCAS found that only 4.4% met strict criteria for idiopathic MCAS, with the average time to diagnosis exceeding four years. A separate German study of 100 patients with suspected MCAS confirmed the diagnosis in only 2%. What this tells us is that many people are suspected to have MCAS and most of those people do not formally meet strict criteria — but the symptoms they experience are still real, the multi-system involvement is still real, and the absence of a strict diagnostic match does not mean there is nothing happening in their immune and autonomic systems.
For our purposes at Lavender Family Chiropractic, the diagnostic debate matters less than the clinical reality. Whether your situation meets formal MCAS criteria or sits in a related territory of histamine intolerance, dysautonomia-driven flares, or what is sometimes called “mast cell activation disease” more broadly, the upper cervical and autonomic angle we work on is relevant to the underlying physiology either way.
The MCAS-POTS-EDS Triad: Why These Conditions Travel Together
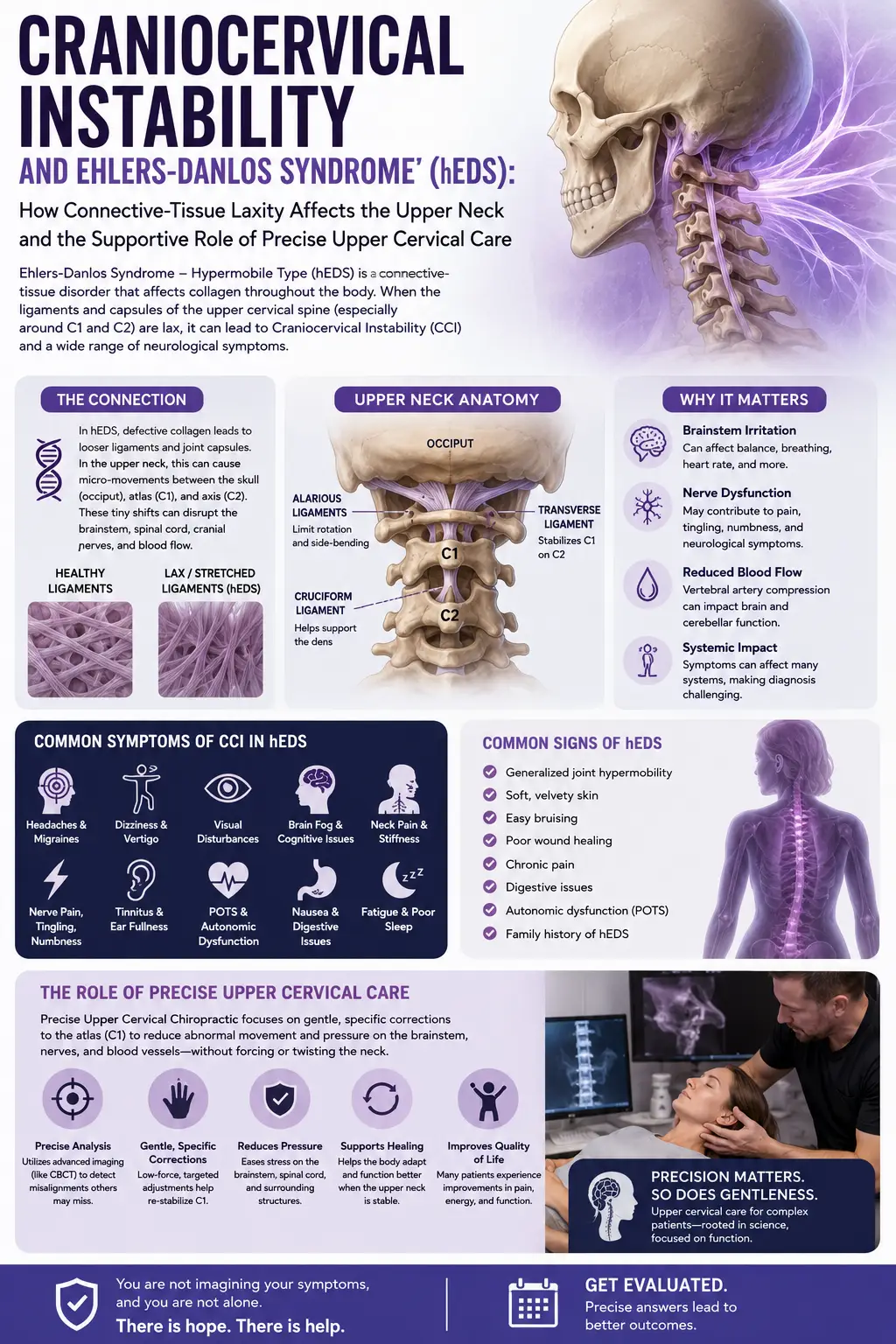
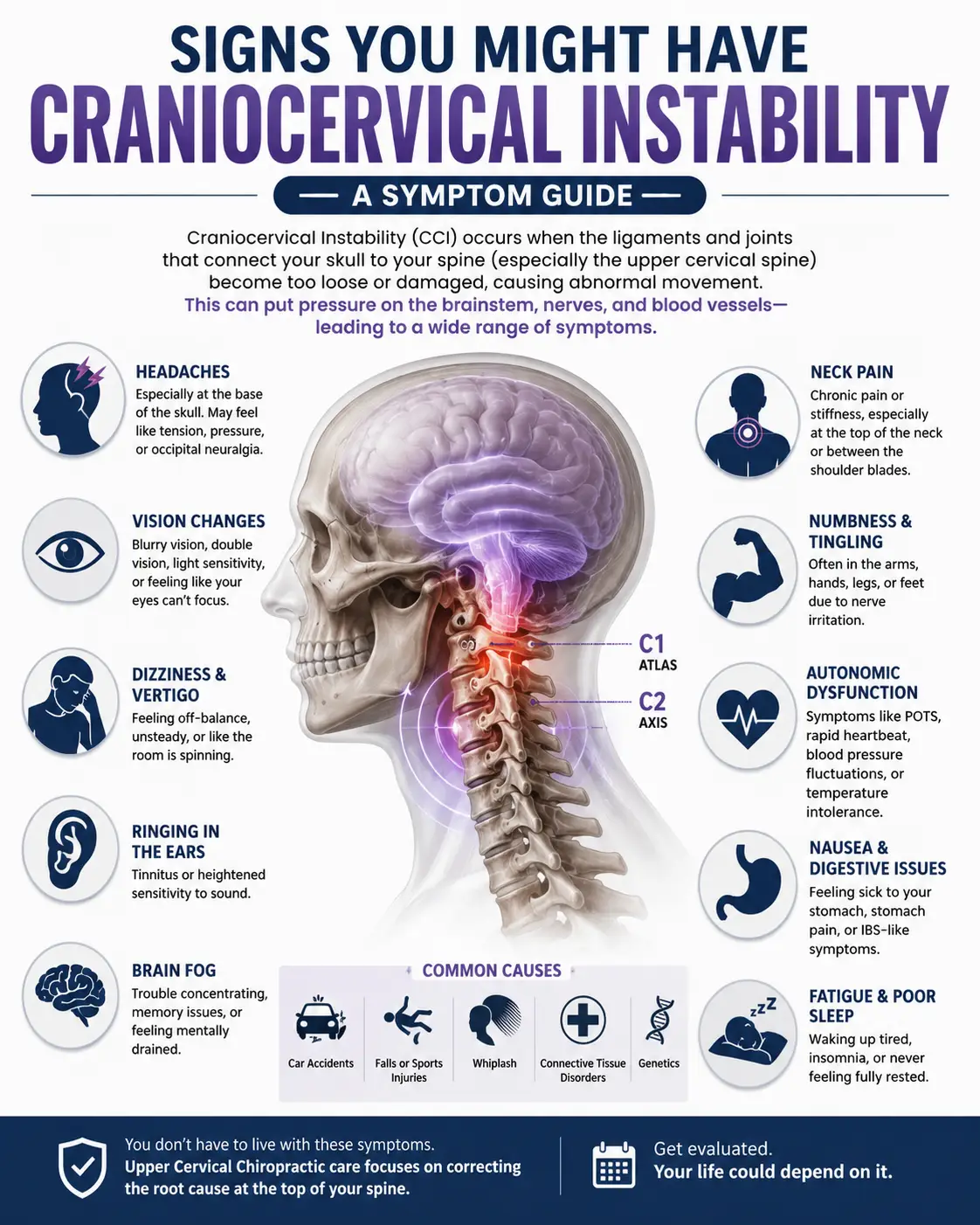
One of the most important clinical observations in MCAS is that it rarely shows up alone. Patients with MCAS very commonly also carry diagnoses of postural orthostatic tachycardia syndrome (POTS) — a form of dysautonomia where the heart rate spikes abnormally upon standing — and of hypermobile Ehlers-Danlos syndrome (hEDS) or hypermobility spectrum disorder (HSD), a connective tissue condition characterized by joint laxity and a wide range of systemic symptoms.
The co-occurrence of these three conditions is so common that the constellation has earned a nickname in the patient community: the trifecta, or the triad. Research has documented striking overlap. One study cited in the dysautonomia literature found that 31% of patients with combined POTS and EDS also met criteria for MCAS, compared to only 2% in the non-POTS-and-EDS group — a 15-fold elevation that is hard to explain by coincidence alone. The same review noted that dysautonomia in general is 3 to 10 times more common in patients with EDS, POTS, and allergic-type disorders compared to the general population.
The pathophysiology of why these three travel together is still being worked out. Some researchers have proposed a shared connective tissue mechanism — the same tissue abnormalities that produce joint hypermobility may also affect blood vessel walls (contributing to POTS) and mast cell distribution (contributing to MCAS). Others have emphasized shared autonomic dysregulation — when the autonomic nervous system loses its ability to properly modulate vascular tone, gastrointestinal motility, and immune signaling, all three conditions become more likely to manifest. A 2024 review in the Journal of Allergy and Clinical Immunology explicitly noted that MCAS has been reported in conjunction with congenital connective tissue disorders such as hypermobility EDS and dysautonomia such as POTS, and proposed autoimmunity and autonomic dysregulation as part of the shared mechanism.
This matters for upper cervical care because POTS and dysautonomia patients frequently respond meaningfully to upper cervical correction — and the same autonomic mechanisms that improve in those patients are directly implicated in mast cell regulation.
The Upper Cervical and Vagus Nerve Connection to Mast Cells
Here is the piece of the puzzle that nobody in your conventional MCAS workup is likely to mention: the vagus nerve directly regulates mast cell behavior, and the vagus nerve is functionally and anatomically tied to the upper cervical spine.
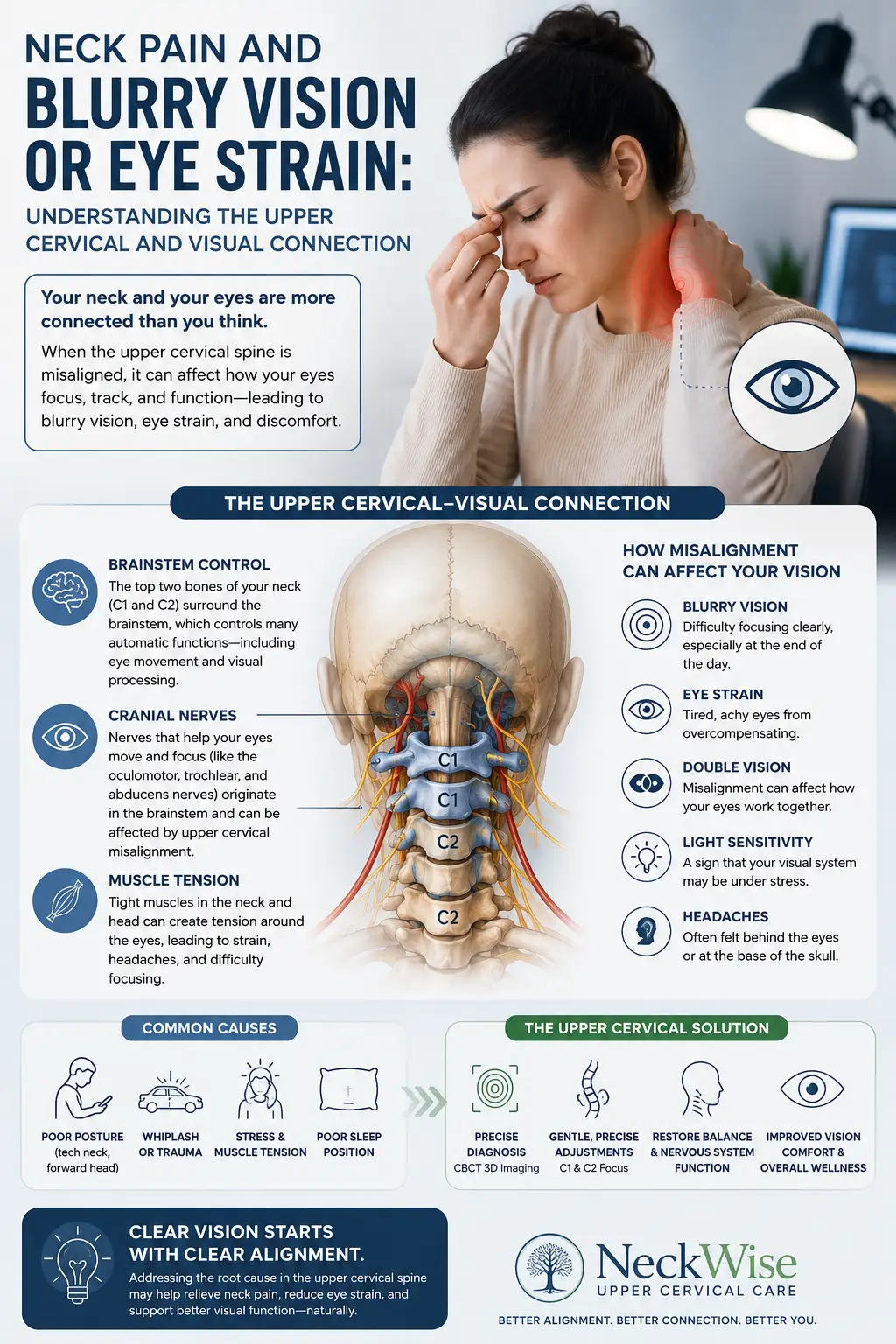
The vagus nerve is the tenth cranial nerve and the longest cranial nerve in the body. It originates in the medulla of the brainstem — the same brainstem that is housed directly behind and below the atlas (C1) and axis (C2) vertebrae — and travels down through the neck, the chest, and the abdomen, providing parasympathetic innervation to the heart, lungs, gut, and most of the body’s internal organs. It is the primary nerve of the parasympathetic nervous system, the so-called “rest and digest” branch of the autonomic nervous system.
What is less widely appreciated is the vagus nerve’s role in regulating inflammation. In the early 2000s, researcher Kevin Tracey and colleagues described what is now known as the cholinergic anti-inflammatory pathway — a system through which the vagus nerve, by releasing acetylcholine and activating alpha-7 nicotinic acetylcholine receptors (α7nAChR), actively suppresses the release of pro-inflammatory cytokines from immune cells, including mast cells. A 2014 study in PLOS One demonstrated that vagal stimulation reduced allergic responses through this nicotinic acetylcholine receptor mechanism, explicitly identifying the vagus nerve as having anti-allergic, mast-cell-regulating properties.
Subsequent research has expanded on this finding. A PMC review on the cholinergic anti-inflammatory pathway documented that α7 nicotinic acetylcholine receptors on macrophages, monocytes, and mast cells mediate the vagus nerve’s anti-inflammatory output — meaning that when vagal tone is high, mast cells are dampened, and when vagal tone is low, mast cells become more reactive. The “inflammatory reflex” model proposes that afferent vagus neurons sense peripheral inflammatory molecules, and efferent vagus neurons then release the brake on inflammation through this cholinergic mechanism.
Now connect this to the upper cervical spine. The vagus nerve exits the skull through the jugular foramen, a bony opening immediately adjacent to the atlas. The atlas’s position has a direct mechanical influence on this region — atlas misalignment can affect the structures surrounding the jugular foramen, alter venous and lymphatic drainage, change dural tension in the upper cervical region, and influence the proprioceptive input that the brainstem uses to calibrate autonomic output. When the upper cervical spine is misaligned chronically, vagal tone tends to drop. When vagal tone drops, the cholinergic anti-inflammatory pathway weakens. When that pathway weakens, mast cells lose one of their most important regulatory brakes.
This is not speculative. The autonomic dysregulation that patients with POTS experience — and that patients with MCAS so often share — is the same autonomic dysregulation that compromises mast cell stability. Addressing the upper cervical foundation that influences vagal tone is one of the few interventions that addresses the upstream mechanism rather than chasing downstream mediators with antihistamines and mast cell stabilizers.
This is exactly why our service page on vagus nerve dysfunction is so frequently relevant to the MCAS patient population — the mechanism is the same.
Why Upper Cervical Care Matters for MCAS Patients
Let us be clear about what upper cervical care can and cannot do. It is not a cure for MCAS, and we make no such claim. The underlying mast cell biology and any genetic predispositions you carry will not be erased by chiropractic care. What upper cervical care can offer is improvement in the autonomic environment in which your mast cells are operating — an environment that, for many MCAS patients, has been dysregulated by upper cervical instability, postural trauma, or chronic stress patterns that have driven them into sympathetic dominance and low vagal tone.
At Lavender Family Chiropractic, we use the Knee Chest Upper Cervical technique — a precise, gentle approach to correcting atlas and axis misalignments without any twisting, popping, or forceful manipulation. For MCAS patients specifically, this gentleness matters enormously. Patients with mast cell instability are often hypersensitive to physical stimuli, and aggressive manipulation of the neck can trigger flares. The Knee Chest technique avoids those forces entirely while still delivering structural correction with sub-millimeter precision.
For MCAS patients, upper cervical correction matters for several reasons. First, restoring proper atlas alignment supports vagal tone by reducing the mechanical and neurological stressors at the craniocervical junction that depress parasympathetic output. Improved vagal tone strengthens the cholinergic anti-inflammatory pathway, which is one of the body’s primary mast cell brakes. Second, addressing upper cervical misalignment improves the overall autonomic regulation that MCAS patients so often struggle with — the same nervous system instability that drives temperature dysregulation, heart rate swings, sleep disruption, and stress reactivity. Third, for the substantial subset of MCAS patients who also carry POTS and/or hypermobility diagnoses, upper cervical care addresses the craniocervical instability that often accompanies hypermobility spectrum disorders and contributes to the overall picture.
We see MCAS patients improve in measurable, meaningful ways under upper cervical care — not in every case, but in many. The most common reports from our patients are reduced episode frequency, decreased severity of flares when they do occur, better sleep, less anxiety, improved tolerance of foods and environments that previously triggered reactions, and a sense of general nervous system calming that they have not experienced in years. None of this comes from us “treating” the mast cells directly. It comes from supporting the autonomic system that regulates them.
What Care Looks Like at Lavender Family Chiropractic
If you come to our Sarasota office for evaluation related to MCAS, here is what to expect.
Your first visit begins with a thorough consultation. Dr. Lavender or Dr. Temple will sit down with you and review your full history — when symptoms started, your trigger profile, what diagnoses you carry, what medications and supplements you are using, what your trifecta or pentad picture looks like, what other providers have told you, and what you are hoping to address. MCAS patients have often been through extensive medical workups, and we want all of that context.
The examination is adapted to MCAS patients. We use advanced 3D CBCT imaging to visualize your upper cervical alignment, autonomic function scans to objectively measure your nervous system state, postural and gait analysis, and a careful clinical neurological exam. We are not measuring mast cells — that is your allergist’s domain. We are measuring the structural and neurological environment in which your mast cells are operating.
If the examination reveals upper cervical findings that are likely relevant to your case, we will explain our recommendations openly. We will also be honest about what upper cervical care cannot do. It is one piece of a multidisciplinary approach for most MCAS patients, and we encourage you to continue working with your allergist, immunologist, dietitian, or functional medicine provider as part of your overall care.
Care is delivered through the Knee Chest Upper Cervical technique, with the gentleness that MCAS patients specifically benefit from. We pace care thoughtfully — many MCAS patients do better with slower, more spaced-out initial visits while their nervous systems adapt — and we adjust the plan as we see how your body responds. We offer customized treatment plans tailored to each patient’s specific situation, recognizing that no two MCAS patients present identically.
Because MCAS frequently overlaps with broader autonomic and neurological dysregulation, our work with these patients often touches on the territory covered by our complex neurological conditions care — the model is designed precisely for patients whose symptoms cross multiple systems and whose diagnoses do not fit neatly into a single specialty.
📞 Call (941) 243-3729 to schedule your complimentary consultation 📅 Book your consultation online 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
What the Research Says About MCAS, Autonomic Function, and Mast Cells
The research landscape on MCAS itself is still developing rapidly, and the literature on upper cervical chiropractic specifically for MCAS is sparse. What is much more robust is the research on the autonomic and vagal mechanisms that influence mast cell behavior — which is where the indirect rationale for upper cervical care lives.
The current consensus diagnostic framework for MCAS, summarized in a 2024 Journal of Allergy and Clinical Immunology review, established the three-criterion model that has become the international standard — recurrent multi-system symptoms, measurable transient mast cell mediator increases, and response to mast cell-targeted therapy. This same review explicitly identified the well-documented co-occurrence of MCAS with dysautonomia (including POTS) and connective tissue disorders like hypermobility EDS, anchoring MCAS in a broader autonomic-immune context.
The 2024 Swedish cohort study published in the Journal of Allergy and Clinical Immunology in Practice analyzed 703 consecutive patients referred for suspected MCAS and found that only 4.4% met strict criteria for idiopathic MCAS, with the average diagnostic delay exceeding four years. This is important context — it tells us that the MCAS diagnostic process is rigorous, that suspected MCAS often turns out to be something else, but also that the patients who do meet criteria endure years of unanswered symptoms before getting a definitive diagnosis.
The mechanistic work on vagal regulation of mast cells provides the strongest support for the upper cervical angle. The 2014 PLOS One study by Kageyama-Yahara and colleagues demonstrated that vagal stimulation suppressed mast cell-driven allergic responses through the α7 nicotinic acetylcholine receptor pathway — explicitly identifying the vagus nerve as having direct anti-allergic, mast-cell-stabilizing properties.
A foundational 2013 PMC review on the cholinergic anti-inflammatory pathway documented that α7 nicotinic acetylcholine receptors on macrophages, monocytes, and mast cells mediate the cholinergic anti-inflammatory output of the vagus nerve — meaning the vagus nerve actively brakes mast cell activation through this molecular pathway. When vagal tone is high, the brake is engaged. When vagal tone is low, the brake releases and mast cells become more reactive.
Finally, a 2023 special issue review in PMC on cholinergic control of inflammation summarized two decades of research on the cholinergic anti-inflammatory pathway and confirmed its role in regulating local and systemic inflammation across a wide range of conditions, including autoimmune and inflammatory diseases. The implication for MCAS is direct: anything that supports vagal tone is likely to support mast cell stability.
This body of research does not prove that upper cervical chiropractic cures MCAS. What it establishes is the underlying biology that makes the upper cervical and vagal connection clinically plausible and worth pursuing as part of a broader strategy.
Lifestyle Factors That Support MCAS Stability
Upper cervical chiropractic care is one tool among many. For MCAS patients, lifestyle support is essential, and the patients who do best are usually working multiple angles simultaneously.
Trigger identification. A careful food and exposure diary remains one of the most useful tools for identifying personal triggers. High-histamine foods, fermented foods, alcohol, aged cheeses, leftovers, and certain medications are common offenders. Work with a clinician familiar with low-histamine and mast-cell-friendly eating.
Vagal tone work. Cold water face exposure, slow diaphragmatic breathing (longer exhales than inhales), humming, gargling, gentle gag reflex stimulation, and singing all activate vagal pathways and can be done at home. Heart rate variability training using a device like the EmWave or HRV apps can give you objective feedback.
Sleep prioritization. Mast cell stability collapses without adequate sleep. Seven to nine hours of high-quality sleep, a cool dark room, and consistent bedtimes are foundational. Many MCAS patients benefit from H1 antihistamines at bedtime as part of their medical management.
Stress reduction. Stress is one of the most potent mast cell triggers there is, because the stress response and mast cell activation share signaling pathways. Whatever practices help you down-regulate — meditation, gentle yoga, time in nature, time with safe people — belong in your toolkit.
Heat and humidity awareness. The Florida climate is a real challenge for MCAS patients. Heat triggers mast cell activation in many patients. Stay hydrated, manage your exposure during the hottest months, and use cooling strategies (cold drinks, cool showers, cooling vests) when you must be outside.
Mold and environmental exposures. Mold is a major and underrecognized MCAS trigger. If your symptoms worsen at home or at work, environmental testing may be warranted.
Movement that does not crash you. MCAS patients often have exercise intolerance, particularly those with concurrent POTS. Recumbent or supine exercise (rowing, swimming, supine cycling) is generally better tolerated than upright cardio. Gentle, consistent movement supports vagal tone and general resilience.
Medical management. Continue working with your allergist or immunologist. H1 and H2 antihistamines, mast cell stabilizers, leukotriene blockers, and other targeted medications have legitimate roles in MCAS management. Upper cervical care complements this work — it does not replace it.
If you found this guide useful, you may also want to read about brachioradial pruritus, another condition where cervical spine dysfunction directly drives a peripheral immune-type symptom (in that case, persistent itching of the forearms) — the mechanism is different but the principle of cervical involvement in a seemingly unrelated symptom is similar.
Serving Sarasota and the Surrounding Communities
Lavender Family Chiropractic is located in Sarasota, Florida, at 5899 Whitfield Avenue, Suite 107 — at the corner of University and Whitfield. From this central location, we serve patients throughout the region, including Bradenton, Lakewood Ranch, Palmetto, Parrish, Venice, Osprey, Nokomis, Ellenton, Ruskin, Myakka City, North Port, and the greater Tampa Bay area. Patients also travel from St. Pete, Riverview, and Manatee County to receive specialized upper cervical care here.
MCAS is the kind of condition where patients are often willing to drive significant distances to find a provider who understands the autonomic and upper cervical components of their illness. If you are dealing with mast cell instability, dysautonomia, hypermobility, or any combination of these and you are looking for an angle that addresses the upstream nervous system mechanisms rather than just downstream mediators, we encourage you to reach out.
Top 15 FAQs About MCAS and Upper Cervical Chiropractic Care
1. Can chiropractic care cure MCAS? No. We make no such claim. Upper cervical care does not cure MCAS, change your genetics, or eliminate the underlying mast cell biology. What it can do is support the autonomic and vagal regulation that influences how reactive your mast cells are — which for many patients produces meaningful improvement in flare frequency and severity.
2. Is upper cervical chiropractic safe for someone with MCAS? The Knee Chest Upper Cervical technique is exceptionally gentle and avoids the forceful manipulation that can trigger reactions in sensitive patients. We also pace care thoughtfully, recognizing that MCAS patients often need slower starts and more spaced-out visits than the general population.
3. What is the connection between MCAS and the vagus nerve? The vagus nerve regulates mast cell activity through the cholinergic anti-inflammatory pathway. When vagal tone is high, the vagus releases acetylcholine that binds to α7 nicotinic acetylcholine receptors on mast cells, dampening their activation. When vagal tone is low, this brake weakens and mast cells become more reactive.
4. What is the MCAS-POTS-EDS triad? It refers to the frequent co-occurrence of mast cell activation syndrome, postural orthostatic tachycardia syndrome, and hypermobile Ehlers-Danlos syndrome. The three conditions overlap so often that many clinicians consider them a recognizable clinical pattern. Patients with one are statistically more likely to have at least one of the others.
5. Will my MCAS doctor approve of chiropractic care? Most allergists and immunologists are not familiar with upper cervical chiropractic specifically, and many are skeptical of chiropractic in general. We encourage open communication with your medical team and we do not ask patients to stop conventional MCAS treatment. We complement it, not replace it.
6. How long does it take to see results? This varies enormously among MCAS patients. Some notice subtle changes in sleep, anxiety, or trigger tolerance within the first few weeks. Others take longer. MCAS is a complex condition and we cannot promise specific timelines — we can only commit to honesty about what we observe along the way.
7. Can the adjustment trigger a flare? In sensitive MCAS patients, almost anything can potentially trigger a flare, and that includes new physical interventions. The Knee Chest technique is significantly gentler than most chiropractic adjustments, but we still introduce care carefully and watch for individual responses. Many patients tolerate it very well from the first visit.
8. Do I need a formal MCAS diagnosis to come in? No. We see patients across the diagnostic spectrum — those with formal MCAS diagnoses, those with suspected MCAS who do not meet strict criteria, those with histamine intolerance, and those with multi-system symptoms that no provider has organized into a diagnosis yet. The upper cervical and autonomic angle is potentially relevant across all of these.
9. Will I need to stop my MCAS medications? No. Continue all of your medications as prescribed by your treating physicians. Upper cervical care is complementary to medical management, not a replacement for it. If your medical team eventually wants to taper based on clinical improvement, that is a discussion for you and them.
10. What if I also have POTS or EDS? That is extremely common in MCAS patients and it does not change our willingness to work with you. In fact, the autonomic and craniocervical instability components of POTS and hypermobile EDS are often particularly responsive to upper cervical care. We have experience with this patient population.
11. Is there research on chiropractic specifically for MCAS? Not yet — at least not robust, published research with MCAS as the primary outcome. What does exist is significant research on the vagal and autonomic mechanisms that regulate mast cells, and clinical research on upper cervical care for related conditions like POTS, dysautonomia, and craniocervical instability. The MCAS-specific rationale draws from this broader body of work.
12. Can stress really trigger MCAS flares? Yes, profoundly. Stress activates the sympathetic nervous system, which directly destabilizes mast cells, and it also depresses vagal tone, which removes the parasympathetic brake on mast cell activation. Stress management is one of the most underrated components of MCAS care.
13. Is the Florida climate bad for MCAS? Heat and humidity can be challenging for MCAS patients, particularly those who also have POTS. Many of our MCAS patients have learned to manage their exposure during the hottest months, hydrate aggressively, and use cooling strategies. The climate is a real factor but it is manageable.
14. How will I know if upper cervical care is right for me? The only way to know definitively is to come in for an evaluation. Our examination will identify whether your upper cervical and autonomic findings are consistent with someone who is likely to benefit. If your situation calls for a different kind of help, we will tell you that honestly.
15. How do I get started? Call our Sarasota office at (941) 243-3729 or book your consultation online. We will sit down with you, review your history, perform a thorough examination, and give you a straight answer about whether upper cervical care is a good fit for your specific situation.
Take the Next Step Toward Stability
MCAS is one of the most disorienting conditions in modern medicine — for the patients who have it, for the providers trying to help, and for the families watching someone they love react to seemingly everything in their environment. The patients who do best are the ones who build a broad, multidisciplinary team and address the condition from every angle they can — medical management, dietary work, environmental control, stress reduction, and the autonomic-nervous-system work that the upper cervical spine sits at the center of.
If you are in Sarasota, Bradenton, Lakewood Ranch, or anywhere in the surrounding region and you are dealing with MCAS, suspected MCAS, histamine intolerance, or the broader trifecta of mast cell instability, dysautonomia, and hypermobility, Dr. Rusty Lavender and Dr. Jacob Temple at Lavender Family Chiropractic are here to help you understand the upper cervical and vagal piece of your healing puzzle. It will not solve everything. It may be one of the most important pieces nobody has offered you yet.
📞 Call (941) 243-3729 today to schedule your complimentary consultation 📅 Book online here 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield