By Dr. Rusty Lavender — Lavender Family Chiropractic, Sarasota, FL
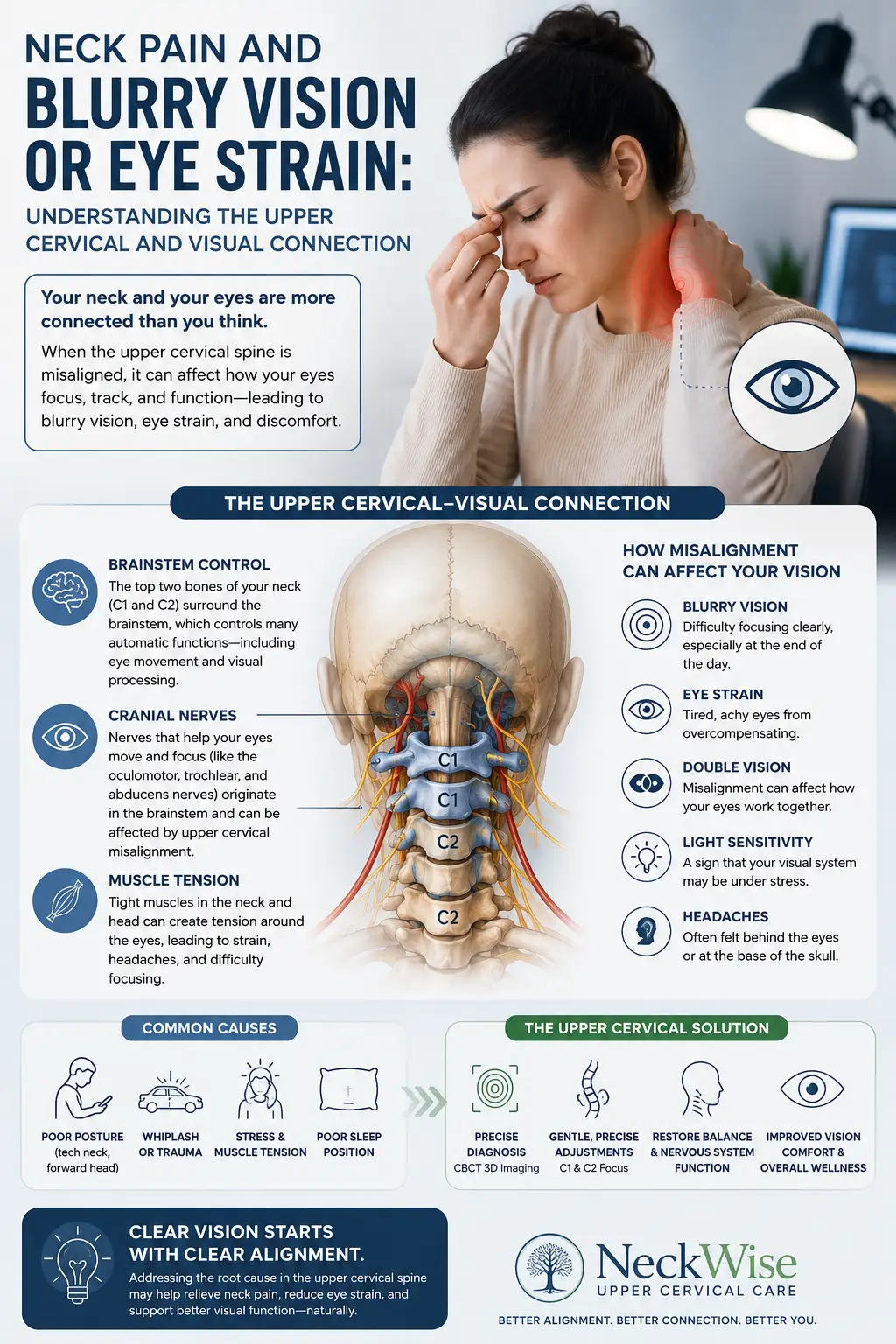
Blurry Vision: If your neck aches at the base of your skull and your eyes feel strained, tired, or slightly out of focus by the end of the day, you may have wondered whether the two problems are related. It is one of the more common questions we hear at Lavender Family Chiropractic in Sarasota, Florida: “Can my neck actually affect my vision?” It is a fair question, and the honest answer is nuanced. The eyes and the upper neck share a surprising amount of wiring in the nervous system, and for some people those connections help explain why neck tension, eye strain, and blur seem to travel together.
At the same time, we want to be clear from the very first paragraph: your eyes deserve a proper medical workup before anyone talks to you about your neck. Blurry vision, double vision, and other visual changes can have many causes, and some of them are serious. This article is meant to help you understand a specific, well-documented relationship between the cervical spine and the visual system — the upper cervical and visual connection — and how gentle, low-force chiropractic care may fit into a broader plan for natural neck pain relief once medical causes have been appropriately evaluated. It is educational information, not a diagnosis, and it is not a substitute for an examination by a physician, optometrist, or ophthalmologist.
In the pages that follow, Dr. Rusty Lavender and Dr. Jacob Temple walk through what the pattern looks like, the neurological mechanisms that tie the neck to gaze and focus, why the top of the neck matters so much, how our office approaches these cases with 3D imaging and a gentle technique, and what current research does and does not show. We will also cover practical lifestyle habits, the communities we serve around Sarasota, and answers to the fifteen questions patients ask us most. Throughout, our goal is to be useful and honest rather than to overpromise.
Blurry Vision and the Neck: When Neck Pain and Visual Symptoms Show Up Together
Let us start with the most important part of this entire article, because your safety comes first.
Sudden or severe visual changes should be treated as a medical emergency until a physician confirms otherwise. If you experience an abrupt loss of vision, a curtain or shadow moving across your visual field, a sudden shower of new floaters or flashing lights, sudden double vision, vision loss in one eye, a severe “worst headache of my life,” facial drooping, slurred speech, weakness or numbness on one side of the body, or eye pain with nausea and halos around lights, do not wait and do not book a chiropractic appointment. Call 911 or go to the nearest emergency room immediately. These symptoms can signal a stroke, a retinal detachment, acute angle-closure glaucoma, an optic nerve problem, or other neurological emergencies where minutes matter. Chiropractic care has no role in an acute emergency, and we would never want a patient to delay urgent care because they were wondering about their neck.
With that firmly established, here is the slower, more chronic pattern that often does have a musculoskeletal component. Many people describe a cluster of symptoms that build gradually over hours or days rather than appearing all at once:
- A dull ache, tightness, or pressure at the base of the skull and upper neck
- Eye strain or eye fatigue, especially after screen work, reading, or driving
- Mild, fluctuating blur or a sense that focusing takes more effort than it used to
- Trouble shifting focus smoothly between near and far objects
- Increased sensitivity to light, particularly bright screens or fluorescent lighting
- A tension-type headache that wraps around the head or sits behind the eyes
- A feeling of visual “tiredness” that improves with rest and worsens with sustained near work
When these symptoms come and go together, tend to track with neck posture and workload, and ease when you rest your neck and eyes, they point toward a functional relationship rather than a structural emergency. Even so, the responsible first step is to see an eye doctor. An optometrist or ophthalmologist can measure your refraction, check your eye pressure, examine the retina and optic nerve, and rule out primary ocular causes such as uncorrected refractive error, dry eye, presbyopia, binocular vision dysfunction, cataract, glaucoma, or retinal disease. Many cases of blur and eye strain are explained entirely by the eyes themselves, and those causes need to be treated on their own terms.
Only after primary ocular and neurological causes have been appropriately evaluated does it make sense to look upstream at the neck. That is the population this article is written for: people with persistent neck pain and eye strain who have had their eyes checked, whose emergencies have been excluded, and who are curious whether their cervical spine could be contributing to how their visual system feels and performs.
The Mechanisms: Cervical Proprioception, the Oculomotor System, and Autonomic Input
Why would the neck have anything to do with the eyes at all? The answer lies in how the brain keeps your gaze stable and your world steady while your head and body are constantly moving. Three overlapping systems do this work together, and the neck feeds signals into all three.
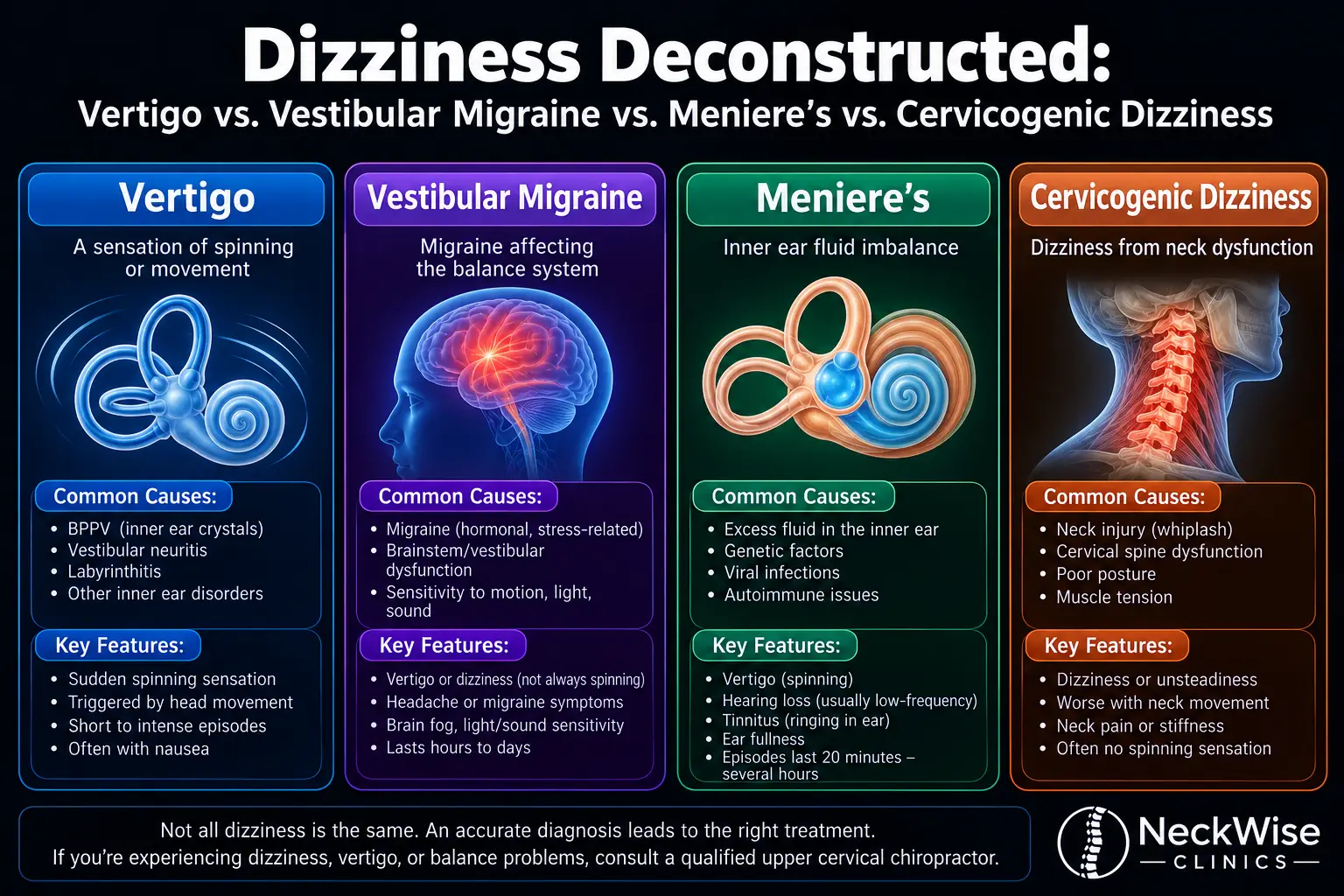
Cervical proprioception and gaze stability. Your upper neck is packed with specialized sensory receptors called proprioceptors, which continuously report the position and movement of your head relative to your body. The brain blends this neck information with input from the inner ear (the vestibular system) and from the eyes themselves to keep images stable on the retina. One of the reflex arcs involved is the cervico-ocular reflex, in which movement signals from the neck help drive compensatory eye movements. There is also the smooth pursuit system, which lets your eyes track a moving object in a smooth, controlled way, and the saccadic system, which snaps your gaze quickly from point to point. When neck proprioception is disturbed by pain, muscle tightness, or altered joint movement, the quality of these eye movements can subtly change, and the effort required to hold steady focus can rise. That extra effort is often experienced as eye strain, visual fatigue, or a vague sense of blur.
Suboccipital muscles as a sensory organ. The small muscles at the very top of the neck, the suboccipital group, contain an unusually high density of muscle spindles compared with most other muscles in the body. In other words, they are less about generating large forces and more about acting as a finely tuned sensory instrument that tells the brain exactly where the head is. This is part of why the upper neck is so influential over head, eye, and balance coordination. When these deep muscles are chronically tight or guarded, the stream of information they send can become noisy, and the brain has to work harder to reconcile neck signals with what the eyes and inner ear are reporting. That mismatch is a recognized ingredient in cervicogenic dizziness, and the same sensory conflict can accompany visual complaints such as difficulty focusing and light sensitivity.
Trigeminocervical convergence and light sensitivity. The nerves that carry sensation from the upper neck (the upper cervical nerve roots) and the nerve that carries sensation from the face and much of the head (the trigeminal nerve) converge on shared pools of neurons in the brainstem, in a region often called the trigeminocervical complex. Because these signals share circuitry, the brain can have trouble telling exactly where a given ache is coming from. This convergence helps explain why upper neck tension so often refers pain into the head and behind the eyes, and why some people with neck-related headache also report sensitivity to light. The pathways for head pain and for light discomfort overlap, so irritation upstream in the neck can color how the whole head-and-eye region feels.
Autonomic input relevant to the pupil and focusing. The autonomic nervous system, and particularly its sympathetic branch, has fibers that travel through the neck region and contribute to functions such as pupil size and the fine adjustments of accommodation (the eye’s focusing mechanism). The relationship here is more complex and less directly established than the proprioceptive one, so we describe it cautiously. Still, it is one more reason the neck and the visual system are not as separate as they might seem, and it may partly explain why some patients notice that their eyes feel more comfortable in dimmer light when their neck is flared up.
Put together, these mechanisms describe a nervous system in which the neck is a genuine contributor to gaze stability, focusing effort, and head comfort. None of this means the neck is the cause of every visual symptom, and it certainly does not replace an eye exam. What it does mean is that, for a person whose eyes have checked out and whose neck is clearly involved, addressing the neck is a reasonable part of the picture. To learn more about how we think about the neck as a whole, our overview of neck pain and its many presentations is a helpful companion to this article.
Why the Upper Neck (Atlas and Axis, C1 and C2) Is Central
If the neck influences the eyes, the top two vertebrae deserve special attention. The atlas (C1) and the axis (C2) are unlike any other bones in the spine, and their unique anatomy is exactly why the upper cervical region sits at the crossroads of head position, balance, and gaze.
The atlas is a ring of bone with no vertebral body. It cradles the base of the skull and lets you nod. The axis sits just below it and features a bony peg, the odontoid process or dens, that projects upward into the ring of the atlas. This peg acts as a pivot, and it is the reason the C1 to C2 joint is responsible for roughly sixty percent of the rotation in your entire neck. When you turn your head to check a blind spot while driving, most of that first rotation happens right at the top of the neck. Because the region is built for so much motion, it relies heavily on ligaments rather than interlocking bony stability, which makes precise, coordinated control especially important.
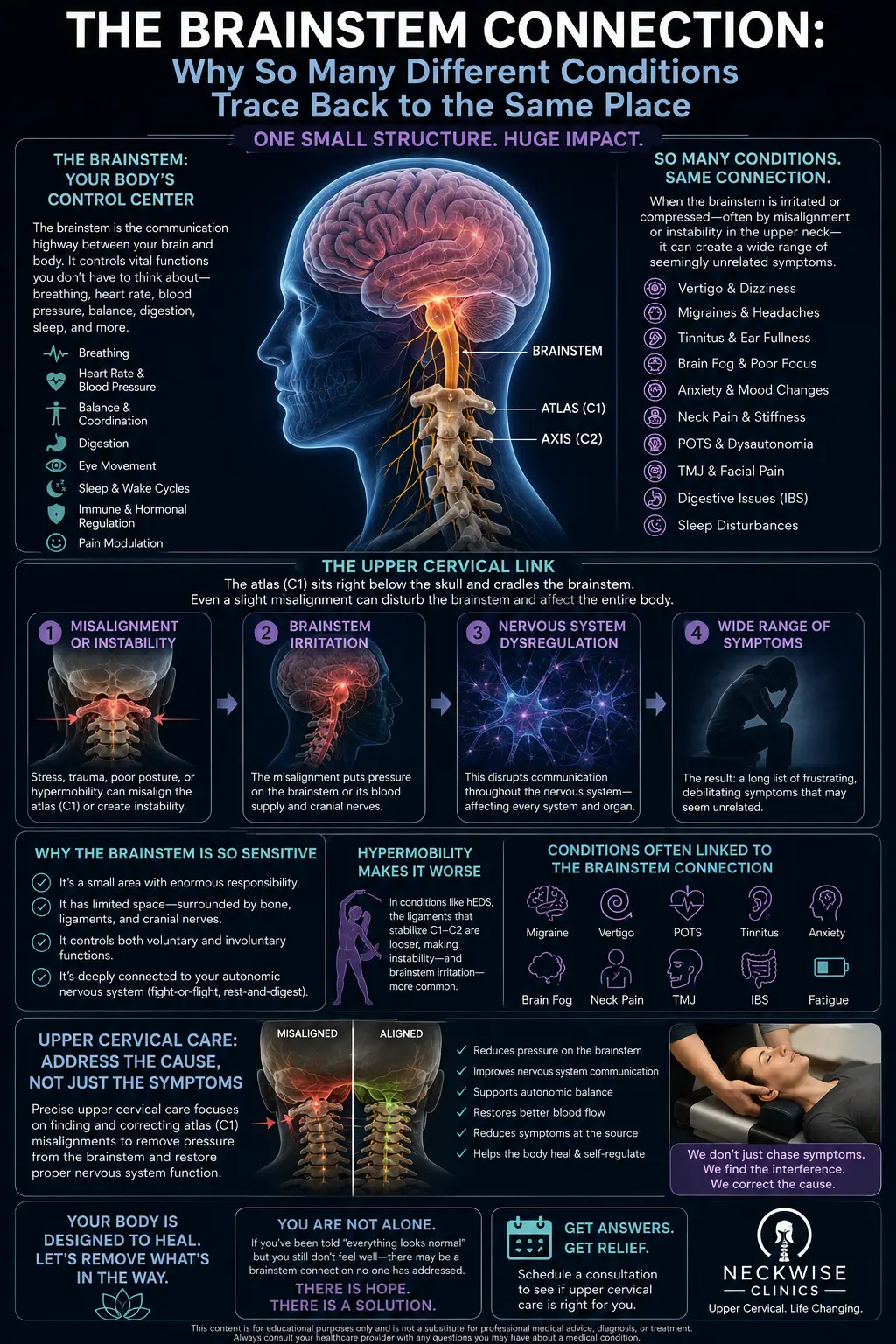
This is also the region richest in the suboccipital proprioceptors we described earlier. The dense concentration of muscle spindles in the small muscles connecting the skull to the atlas and axis makes the upper neck a primary source of the position information the brain uses to keep the eyes and head working together. And because the upper cervical spine sits immediately below the brainstem, where many of the reflex centers for eye movement, balance, and autonomic function reside, the area has an outsized influence relative to its small size. Disturbances in how the atlas and axis move and how their surrounding muscles report position may ripple into the systems that govern gaze stability and visual comfort.
This anatomy is precisely why our practice focuses on the upper cervical spine. Rather than treating the neck as one undifferentiated block, upper cervical chiropractic care concentrates on the alignment and movement of C1 and C2 and their relationship to the head. The same upper cervical involvement that can contribute to visual symptoms also shows up in related complaints we see often, such as pressure and tension at the base of the skull and neck-related dizziness. These are not coincidences; they reflect how much sensory and reflex traffic passes through this compact region.
How Upper Cervical Care Works at Lavender Family Chiropractic
Patients who come to us with neck pain and visual symptoms are often surprised by how methodical and gentle our process is. We do not guess, and we do not twist or crack the neck. Here is how we approach these cases.
A thorough consultation and history. Everything begins with listening. We want to understand the full story: when your neck pain and eye strain started, what makes each better or worse, your screen and reading habits, your sleep, any prior injuries such as whiplash or concussion, and crucially, what your eye doctor and physician have already found. If you have not yet had a comprehensive eye examination, we will encourage you to get one, because ruling out primary ocular and neurological causes is a necessary step, not an optional one. Our job is to determine whether an upper cervical problem is a plausible contributor to your symptoms, and to be honest when it is not.
3D CBCT imaging. To see the upper cervical spine clearly, we use 3D cone beam computed tomography imaging. Unlike a flat, two-dimensional X-ray, CBCT lets us evaluate the atlas and axis and their relationships from multiple angles with fine detail. This helps us understand your individual anatomy and tailor our approach to how your spine is actually built and positioned, rather than relying on a generic template.
Tytron paraspinal infrared thermography. We also use Tytron paraspinal infrared thermography, a non-invasive scan that measures subtle temperature patterns alongside the spine. Because skin temperature is partly regulated by the autonomic nervous system, these readings give us an objective, repeatable way to monitor how your nervous system is functioning over time and whether things are trending in a favorable direction. Nothing touches you and nothing is emitted; the device simply reads infrared signals.
The Knee Chest Upper Cervical technique. Our adjusting method is the Knee Chest Upper Cervical technique, a low-force, specific approach to the upper neck. There is no twisting, no forceful cracking, and no cavitation-style popping. Instead, the correction is precise and gentle, guided by your imaging and examination. For patients who are nervous about having their neck adjusted, or who have simply never liked the sensation of high-velocity manipulation, this technique is often a comfortable alternative. The aim is to support better upper cervical alignment and movement so the nervous system can do its job with less interference, which in turn may help the systems that govern gaze stability and visual comfort.
Customized care plans. After we have gathered your history, imaging, and thermography, we build a care plan tailored to you. Each plan is designed around your specific findings rather than a generic template. We design customized care plansbased on your findings, your goals, and how your body responds over time. We will explain what we see, what we recommend, and why, and we will adjust the plan as your progress guides us. Our commitment is to be transparent about expectations, including the reality that responses vary from person to person and that we cannot promise any specific change in your vision.
Ready to Talk Through Your Symptoms?
If you are dealing with persistent neck pain along with eye strain or blur, and you have had your eyes and general health appropriately evaluated, we would be glad to help you understand whether your upper cervical spine may be part of the picture. Call Lavender Family Chiropractic at (941) 243-3729 to speak with our team, or schedule directly through our new patient scheduling page. Our office is located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, right at the corner of University and Whitfield. We serve patients from across the Sarasota and Bradenton region and would be happy to answer your questions.
What the Research Says
Research into the neck and visual system is active and genuinely interesting, but it is also early and mostly focused on associations rather than treatment outcomes for vision. We think it is important to describe these studies accurately and cautiously rather than overstate them. Here are five peer-reviewed sources, with what they do and do not show.
- In a study finding that the cervico-ocular reflex is increased in people with nonspecific neck pain, published in the journal Physical Therapy, researchers used infrared eye tracking to compare people with nonspecific neck pain to healthy controls and observed a higher cervico-ocular reflex gain in the neck pain group. This suggests that altered neck sensory input can measurably change how the eyes respond to body movement, though it is a group-level association and does not establish that treating the neck changes vision.
- In a cross-sectional study of cervico-ocular and vestibulo-ocular reflexes in subclinical neck pain, published in Brain Sciences, investigators found that individuals with recurrent, low-grade neck pain had a significantly larger cervico-ocular reflex gain than healthy controls, which the authors interpreted as a sign of altered proprioceptive feedback and sensorimotor integration. Again, this points to a real neck-to-eye relationship at the level of reflexes, while remaining an observational finding in a relatively small sample.
- In a study asking whether altered oculomotor control during the smooth pursuit neck torsion test relates to subjective visual complaints in patients with neck pain disorders, published in the International Journal of Environmental Research and Public Health, researchers used video-oculography to measure smooth pursuit eye movements in neutral and neck-torsion positions and reported that measures taken with the neck turned better classified patients’ visual symptoms, suggesting a cervically driven component to some visual complaints. It is a diagnostic-classification study, not a treatment trial, so it describes an association rather than an outcome of care.
- In a narrative review of proprioceptive cervicogenic dizziness covering pathogenesis, diagnosis, and treatment, published in the Journal of Clinical Medicine, the authors describe how cervical proprioceptive input is normally integrated with visual and vestibular signals, and how a mismatch among these inputs can produce dizziness, unsteadiness, and visual disturbances. As a narrative review, it synthesizes existing literature and offers a framework rather than new experimental data, and it emphasizes careful diagnosis and exclusion of other causes.
- In a systematic analysis of the global burden of neck pain from 1990 to 2020 with projections to 2050, published in The Lancet Rheumatology as part of the Global Burden of Disease Study 2021, researchers estimated that neck pain affected roughly 203 million people in 2020 and projected continued growth in coming decades. This does not speak to vision directly, but it puts the sheer scale of neck pain in perspective and underscores why understanding its wider effects, including on daily visual comfort, matters to so many people.
Taken together, these studies support a consistent theme: the neck and the visual system are neurologically linked, and neck problems can be associated with measurable changes in eye movement control and with subjective visual complaints. What the current evidence does not do is prove that chiropractic care improves vision. We share this literature so you can make an informed decision, and we hold ourselves to describing it as it is.
Lifestyle Factors That Support Your Neck and Eyes
Care in our office is only one piece of the puzzle. The habits that fill your day have a large influence on both neck comfort and visual fatigue, and small changes often add up. These suggestions may help support your neck and eyes, and they cost nothing to try.
Follow the 20-20-20 guideline. Sustained near focus is tiring for the eyes and encourages a forward-head posture that loads the upper neck. A widely recommended habit is that every 20 minutes, you look at something about 20 feet away for about 20 seconds. This gives the focusing muscles a brief rest and prompts you to lift your head and reset your posture.
Set up your screens thoughtfully. Position the top of your monitor at or slightly below eye level so you are not craning your neck down or up. Keep the screen roughly an arm’s length away. If you use a laptop for long stretches, an external keyboard and a raised stand can spare your neck considerably. On phones and tablets, bring the device up toward your eyes rather than dropping your head down toward the device.
Mind your lighting and contrast. Harsh glare and dim, low-contrast environments both make the eyes work harder. Aim for even, comfortable lighting, reduce glare on screens, and consider warmer, dimmer lighting in the evening. If bright light bothers your eyes when your neck is flared, that is worth mentioning to both your eye doctor and to us.
Protect your posture through the day. The issue is rarely a single “perfect” posture; it is staying in any one position too long. Take movement breaks, roll your shoulders, and gently move your neck through comfortable ranges. Frequent small changes in position tend to be kinder to the upper neck than rigidly holding still.
Prioritize sleep and your sleep position. Poor sleep amplifies pain sensitivity and eye fatigue alike. A supportive pillow that keeps your neck in a neutral position, and sleeping on your back or side rather than your stomach, can reduce overnight strain on the upper cervical region. If you wake with neck stiffness and tired eyes, your sleep setup is a reasonable place to start.
Stay hydrated and blink. Screen work reduces how often we blink, which contributes to dryness and the feeling of tired, gritty eyes. Consciously blinking and staying hydrated can ease some of that discomfort. Persistent dryness should be evaluated by your eye doctor, as dry eye is a common and treatable cause of blur and strain.
If your neck symptoms also include lightheadedness or a swimmy, off-balance feeling, you may find our article on whether neck pain can cause dizziness worthwhile, since the same upper cervical mechanisms are involved. Lifestyle changes are not a replacement for proper evaluation, but they are a sensible foundation while you sort out the underlying causes with your care team.
Serving Sarasota and Surrounding Communities
Lavender Family Chiropractic is proud to serve individuals and families throughout Southwest Florida who are looking for gentle, upper-cervical-focused care. Our office at the corner of University and Whitfield is convenient to a wide area, and we welcome patients traveling from across the region.
We regularly care for people from Sarasota, Bradenton, Lakewood Ranch, Venice, Palmer Ranch, Osprey, Siesta Key, Longboat Key, Lido Key, University Park, Parrish, Ellenton, Myakka City, Punta Gorda, and St. Petersburg. Whether you are just down the road in Sarasota or making the drive from Punta Gorda or St. Petersburg, our team is glad to help you understand your neck symptoms and whether our approach is a fit for your situation. If you are unsure about travel or scheduling, please reach out through our contact page or give us a call and we will do our best to make it work.
Top 15 Questions About Neck Pain, Eye Strain, and Upper Cervical Care
1. Can neck problems really affect my vision? The neck and visual system are neurologically connected through cervical proprioception, shared brainstem circuitry, and reflexes such as the cervico-ocular reflex. For some people, upper neck dysfunction is associated with eye strain and difficulty focusing. That said, the neck is not the cause of every visual symptom, and your eyes should be evaluated first.
2. When is blurry vision an emergency, and should I see an eye doctor before a chiropractor? Yes, please see an eye doctor first for any new or persistent visual changes. And treat certain symptoms as emergencies: sudden vision loss, a curtain or shadow across your vision, a sudden burst of floaters or flashes, sudden double vision, severe eye pain with halos and nausea, or vision changes with weakness, numbness, facial droop, or slurred speech. Those require calling 911 or going to the emergency room right away, because they can signal stroke, retinal detachment, acute glaucoma, or other serious conditions. Chiropractic care is only appropriate after emergencies and primary ocular causes have been appropriately evaluated.
3. Will upper cervical chiropractic improve my eyesight? We cannot promise any change in your vision, and we will never claim to. What we focus on is your neck. Some patients report that their eyes feel less strained as their neck comfort improves, but the research supports an association between neck function and eye movement control rather than proof that chiropractic improves vision. We aim to be honest about that distinction.
4. What causes the combination of neck pain and eye strain in the first place? Common contributors include prolonged near work and screen time, forward-head posture, tightness in the suboccipital muscles, prior neck injuries such as whiplash, and uncorrected vision problems that make you strain. Often several factors overlap, which is why we look at the whole picture and coordinate with your eye care.
5. Is the Knee Chest Upper Cervical technique painful? No. It is a low-force, gentle, and specific technique with no twisting and no forceful popping. Most patients find it comfortable, including those who have felt uneasy about traditional high-velocity neck adjustments.
6. Why do you use 3D CBCT imaging instead of a regular X-ray? 3D cone beam computed tomography lets us evaluate the atlas and axis in three dimensions with fine detail, so we can tailor our approach to your actual anatomy rather than a flat, generic view. It helps us be precise and specific.
7. What is Tytron thermography and does it hurt? Tytron paraspinal infrared thermography is a non-invasive scan that reads subtle temperature patterns alongside your spine, which reflect autonomic nervous system activity. Nothing touches you and nothing is emitted. It gives us an objective way to monitor your progress over time.
8. How is this different from a general chiropractor? Our practice concentrates on the upper cervical spine, the C1 and C2 region, using specific low-force correction guided by 3D imaging and thermography. Rather than adjusting the whole spine broadly, we focus on this influential area and how it relates to the head and nervous system.
9. Do you take my insurance? We are a cash-pay, out-of-network practice, which means we do not bill insurance directly. We provide a superbill you can submit to your insurance company for possible reimbursement, depending on your individual plan and benefits. Being out-of-network lets us structure care around your needs rather than around insurance restrictions. Our team is happy to explain the details before you begin.
10. How do you structure your care? We design customized care plans based on your history, imaging, thermography, and goals. Your plan is built around what your evaluation actually shows, and we explain what we recommend and why up front, so you always know what to expect. Everything is tailored to you.
11. How long before I might notice a difference? Responses vary widely from person to person, and we cannot promise any particular timeline or outcome. Some people notice changes in neck comfort relatively early, while others take longer, and some do not respond as hoped. We track your progress objectively and keep you informed as your plan unfolds.
12. Could my headaches be related to all of this too? Often, yes. Tension-type and cervicogenic headaches frequently involve the upper neck, and the trigeminocervical convergence in the brainstem helps explain why upper neck tension can refer pain into the head and behind the eyes. Many patients with neck pain, eye strain, and headache have overlapping mechanisms.
13. I sit at a computer all day. Is my job the problem? Prolonged screen work and forward-head posture are common contributors to both neck strain and visual fatigue. Your job may not be the sole cause, but adjusting your workstation, taking movement breaks, and using the 20-20-20 habit can meaningfully support your neck and eyes.
14. Is upper cervical care safe? The Knee Chest Upper Cervical technique is a gentle, low-force method with no twisting or cracking, and we screen carefully during your consultation and imaging to determine whether you are an appropriate candidate. If your symptoms suggest a medical or ocular emergency, we will direct you to the appropriate provider rather than proceed with care.
15. What should I do first if I have both neck pain and blurry vision? Start with your health: if anything is sudden, severe, or accompanied by neurological symptoms, seek emergency care. For persistent, gradual symptoms, see an optometrist or ophthalmologist to evaluate your eyes. Once emergencies and primary ocular causes have been appropriately addressed, you are welcome to contact us to discuss whether your upper cervical spine may be contributing and whether our gentle approach is a reasonable fit.
Take the Next Step Toward Natural Neck Pain Relief
Neck pain paired with eye strain can wear you down, and understanding the connection is the first step toward doing something about it. If your eyes and overall health have been appropriately evaluated and you are ready to explore whether your upper cervical spine is part of the story, we would be glad to help you find natural neck pain relief through gentle, specific care.
Call Lavender Family Chiropractic today at (941) 243-3729, or book online through our new patient scheduling page. You can also learn more about our approach on our contact page. Our office is located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, at the corner of University and Whitfield, and we serve patients throughout Sarasota, Bradenton, Lakewood Ranch, and the surrounding communities. When you are ready to talk it through, reach out at (941) 243-3729and our team will help you take the next step.