By Dr. Rusty Lavender — Lavender Family Chiropractic, Sarasota, FL
Pain in the shoulder blades: Few complaints are as stubborn or as puzzling as a deep, nagging ache parked squarely between the shoulder blades. You feel it when you sit at your desk, when you scroll on your phone, when you try to fall asleep, or when you have been driving too long on I-75. You stretch it, you foam-roll it, you dig a tennis ball into it against a wall, and you rub creams into the spot itself. Sometimes it eases for an hour. Then it creeps right back to that same tender patch of upper back. If this sounds like your daily story, you are far from alone, and the reason the pain keeps returning may have very little to do with the place where you feel it.
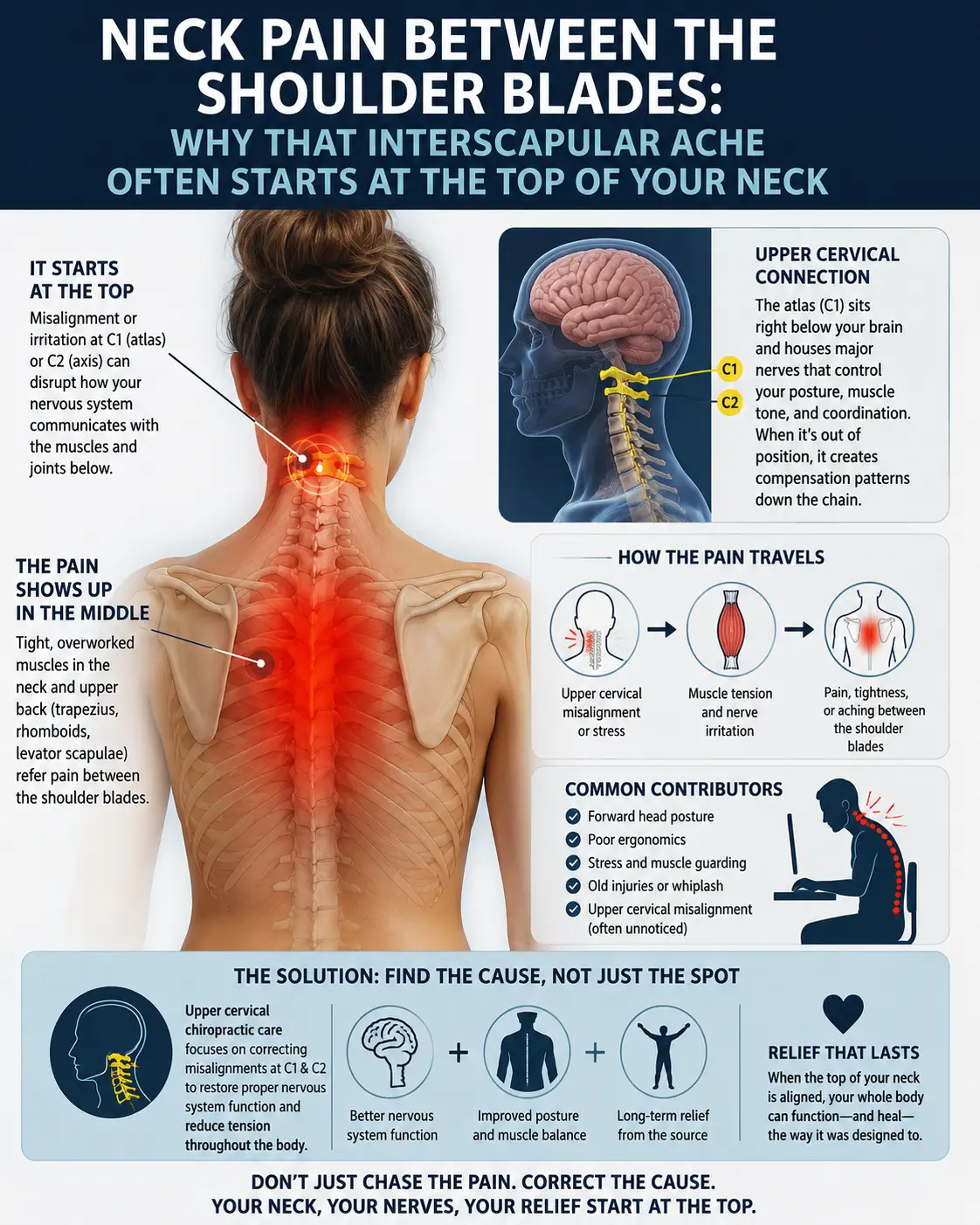
Here is one of the most counterintuitive truths in musculoskeletal care: pain felt between the shoulder blades, in the interscapular and upper-back region, frequently originates higher up, in the neck, and often near the very top of the cervical spine. The nerves that carry sensation from your neck and the muscles that anchor your shoulder blades are wired together in ways that can send a signal from the neck and make it “land” in the mid-back. When the top of the neck is not moving or aligned the way it should, the muscles below it work overtime to compensate, and that constant tension tends to settle right where so many people point when they say, “It hurts right here.”
At Lavender Family Chiropractic in Sarasota, Florida, we focus on the upper cervical spine, the delicate junction where your head meets your neck, using a low-force, no-twisting, no-popping approach. In this article, we will walk through what actually causes pain between the shoulder blades, the nerve mechanisms that refer neck problems down into the upper back, why the atlas and axis (C1 and C2) sit at the center of so many compensation patterns, and how gentle upper cervical chiropractic care may support natural neck pain relief. We will also be candid about something important: interscapular pain can occasionally be a warning sign of a serious, non-musculoskeletal problem, and knowing those red flags is the first step before anyone should focus on the spine at all.
What Causes Pain Between the Shoulder Blades?
Most of the time, pain between the shoulder blades is musculoskeletal, meaning it comes from muscles, joints, ligaments, discs, or the nerves that serve them. But “musculoskeletal” covers a lot of ground, and understanding the layers helps explain why the obvious remedies so often fall short.
The muscles that live between your shoulder blades
Three muscles get blamed most often, and for good reason. The rhomboids (major and minor) run from the spine of the thoracic and lower cervical vertebrae out to the inner border of each shoulder blade. Their job is to pull the shoulder blades toward the spine and stabilize them against the rib cage. When you sit hunched forward for hours, your shoulder blades drift apart and the rhomboids are held in a lengthened, strained position, which is a recipe for a burning, aching interscapular complaint.
The levator scapulae is arguably the most important muscle in this whole conversation, and we will return to it repeatedly. It attaches to the upper four cervical vertebrae (C1 through C4) at the top and to the upper inner corner of the shoulder blade at the bottom. Because it bridges the neck and the shoulder blade so directly, a problem at the top of the neck can translate into tightness, tenderness, and referred discomfort right at the medial border of the scapula, exactly where interscapular pain tends to hide.
The trapezius, especially its middle and lower fibers, spans the base of the skull, the neck, and the mid-back, fanning out to the shoulder blade and collarbone. Its upper fibers are the ones that “bunch up” toward your ears when you are stressed, and the middle fibers cross the interscapular zone directly. Sustained tension anywhere along the trapezius can create trigger points, those tight, tender knots that not only hurt locally but also refer pain to distant areas.
When these muscles develop myofascial trigger points, the pain map does not always match the source. Research on the muscles that cross the neck, shoulder, and interscapular region has documented how trigger points in the levator scapulae, rhomboids, and neighboring muscles can reproduce a patient’s medial periscapular pain, particularly in people with forward head carriage and rounded, protracted shoulders. In other words, the spot you press is often the messenger, not the origin.
Joints, discs, and posture
Beyond muscle, the small facet joints of the cervical and upper thoracic spine, the intervertebral discs, and the ligaments that hold everything together can all contribute to upper-back and interscapular pain. Prolonged forward head posture, the kind produced by laptops, phones, and long commutes, dramatically increases the load these structures must bear. For every inch the head drifts forward of the shoulders, the effective weight the neck and upper-back muscles must support rises substantially. That is a big reason “tech neck” and interscapular pain so often travel together. If this pattern sounds familiar, our overview of why tech neck develops and how to break free of it is a useful companion read.
An honest note on red flags
Before we go any further, we need to be intellectually honest, because this matters more than any adjustment. Pain between the shoulder blades is usually mechanical, but not always. The interscapular region is one of the classic places where the body refers pain from internal organs. A heart problem, including angina or a heart attack, can present as pain or pressure between or beneath the shoulder blades, sometimes with jaw, arm, or chest involvement, shortness of breath, sweating, or nausea. Gallbladder disease classically refers pain to the right shoulder blade area. Problems with the aorta, esophagus, lungs, or, rarely, spinal infection or tumor can also announce themselves here. Sudden, severe, tearing pain, pain with fever, unexplained weight loss, night pain that will not let you rest, or pain accompanied by cardiac or breathing symptoms are not problems for a chiropractor to sort out first. They warrant urgent medical evaluation, and in the case of possible cardiac symptoms, calling 911. We would rather you be checked and reassured than assume a serious problem is “just a knot.” Only once those concerns have been responsibly ruled out does it make sense to focus on the cervical and upper cervical angle we discuss below.
The Nerve Mechanisms: Referred Pain From the Neck
To understand why a neck problem can be felt in the upper back, you have to understand how the nervous system is wired, and specifically the concept of referred pain.
Why the brain gets “confused” about location
Referred pain happens because sensory nerve fibers from different regions of the body converge on the same segments of the spinal cord before their signals travel up to the brain. When many inputs share a common highway, the brain cannot always tell exactly which side road a signal came from, so it interprets the pain as coming from a broader or different area than the true source. This is not a flaw so much as a feature of how densely the body is innervated, and it is exactly why cervical structures can produce pain that is felt well below the neck.
The cervical nerve roots and the dorsal rami
Each level of the cervical spine gives rise to a pair of spinal nerves, from C1 down through C8. Shortly after a spinal nerve exits, it splits into a ventral ramus (which serves the front and sides of the body and the arms) and a dorsal ramus(which serves the deep muscles, skin, and joints of the back of the neck and back). The dorsal rami are quiet workhorses. Their medial branches supply the facet joints of the spine and the deep paraspinal muscles, and they carry pain signals from those structures back to the cord.
This is where interscapular pain enters the picture. Classic pain-mapping research determined the referral zones of the cervical facet joints and cervical dorsal rami by stimulating them directly and recording where patients felt the resulting pain. The lower cervical joints and dorsal rami, particularly around C6 and C7, were shown to refer pain into the shoulder girdle and the region over and between the shoulder blades. So a joint irritation at the base of the neck can generate a very real, very physical ache that the patient perceives as an upper-back problem, because the nerve that reported it is anatomically tied to the interscapular zone.
Complementary mapping work in the cervical spine confirmed that individual facet joints produce characteristic, and to a large degree predictable, referral patterns. The C7 zygapophysial joint in particular has been associated with pain radiating toward the interscapular and superomedial scapular region. When clinicians know these maps, a patient’s pain diagram becomes a clue pointing back up to the responsible cervical segment rather than a treatment target in its own right.
The levator scapulae and the dorsal scapular nerve: a direct C3–C5 link
Now we can tie the muscle story and the nerve story together. The levator scapulae, that neck-to-shoulder-blade bridge, is supplied by branches of the C3, C4, and C5 nerves, and by the dorsal scapular nerve, which arises primarily from the C5 root (with frequent contribution from C4). The dorsal scapular nerve also supplies the rhomboids. Trace that circuit and the picture becomes clear: the muscles most responsible for holding your shoulder blades in place are driven by nerves that originate in the middle and upper portions of your neck.
When those upper and mid-cervical segments are irritated, mechanically stressed, or not moving well, the muscles they power, the levator scapulae and rhomboids, can become chronically tense, tender, and prone to trigger points. A retrospective clinical review of interscapular, mid-thoracic myofascial pain highlighted exactly this cluster, describing a periscapular pain pattern involving the trapezius, rhomboids, levator scapulae, and the dorsal scapular nerve, frequently in the setting of forward head posture. This is the anatomical reason that rubbing the sore spot between your shoulder blades so often disappoints: you are treating the muscle at the end of the wire, not the neck segment where the wire begins.
Why the Upper Neck (Atlas/Axis, C1/C2) Drives Compensation Downstream
If the middle and lower neck can refer pain into the upper back, why do we at Lavender Family Chiropractic pay such close attention to the very top of the neck, the atlas (C1) and axis (C2)? Because the upper cervical spine is the master regulator of how the entire spine and postural system organizes itself, and small problems there tend to cascade downward.
The unusual anatomy of C1 and C2
The upper cervical spine is unlike any other region of the spine. The atlas (C1) is a ring of bone with no vertebral body and no disc between it and the skull or between it and the axis below. Instead of interlocking bony joints and a disc for stability, the atlas relies heavily on ligaments and muscles to stay properly positioned while still allowing a remarkable range of motion. It cradles the skull and lets you nod “yes.” The axis (C2) has a peg-like projection called the dens, or odontoid process, that rises up through the ring of the atlas and acts as a pivot. This pivot is why roughly half of your head’s total rotation, commonly cited at around 50 percent or more of cervical rotation and the majority of the neck’s uppermost rotational movement, occurs at the C1–C2 joint alone. When you turn your head to check your blind spot on University Parkway, the atlantoaxial joint is doing most of that work.
This design gives you mobility and a wide field of view, but it comes with a trade-off. Because the atlas is stabilized more by soft tissue than by bone and disc, it can shift out of its ideal alignment relative to the skull above and the axis below. The upper cervical region also sits at the crossroads of enormous amounts of neurology; the brainstem transitions into the spinal cord here, and the postural control centers that keep your head level and your eyes on the horizon are constantly reading signals from this area.
How an upper cervical misalignment ripples down the chain
Your body has a non-negotiable priority: keep your eyes level and your head balanced over your center of gravity so you can see, hear, and stay upright. If the atlas shifts, even slightly, the head can tilt or rotate away from level. The nervous system will not tolerate a crooked head, so it recruits compensations further down the chain to bring your eyes back to the horizon. The lower neck may side-bend or rotate to counter the top. One shoulder may ride higher than the other. The muscles that anchor the head and shoulder blades, the levator scapulae, upper trapezius, and rhomboids, are pulled into an asymmetrical, sustained holding pattern to prop up the correction.
That sustained holding pattern is fatiguing, and fatigue in a postural muscle shows up as aching, tightness, and trigger points. Because the levator scapulae attaches at both the upper neck (C1–C4) and the shoulder blade, it is uniquely positioned to broadcast an upper cervical problem straight down to the interscapular region. Meanwhile, the mid and lower cervical facet joints, now working through an abnormal amount of compensatory motion, can become irritated and refer their own pain into the upper back through the dorsal rami, exactly as the pain-mapping studies describe. The result is a person who feels pain squarely between the shoulder blades while the true driver sits several segments higher, at the top of the neck.
This is why chasing the symptom rarely settles the pattern. Stretch the levator scapulae and it tightens again by afternoon, because the nervous system still needs it to hold the head level. Massage the rhomboids and they knot up again by the next workday. Until the upper cervical alignment and movement are addressed, the compensation, and the interscapular pain it produces, has a reason to keep coming back. If you want to go deeper on the muscle side of this loop, our guide on practical ways to release tight neck muscles pairs well with the structural approach described here, and our broader neck pain resource ties the whole picture together.
How Upper Cervical Care Works at Lavender Family Chiropractic
Our approach is built around a simple idea: find out precisely what is happening at the top of the neck, then make a gentle, specific correction, and let the body do the rest. We do not twist, crack, or forcefully manipulate the neck. Here is what care looks like at our Sarasota office.
A thorough consultation and history
Everything begins with listening. We want to understand your pain, its history, your work and sleep postures, prior injuries (including old whiplash, sports impacts, or falls that you may have forgotten), and, critically, we screen for the red-flag features described earlier. If anything suggests a non-musculoskeletal cause, our job is to make sure you get the right medical evaluation first. Care that is right for you starts with making sure care is appropriate at all.
Precise imaging: 3D CBCT and Tytron thermography
The upper cervical spine is small, three-dimensional, and highly individual; no two atlases are misaligned in exactly the same way. Guessing is not good enough. That is why we use 3D cone beam computed tomography (CBCT) imaging to see the true anatomy and orientation of your atlas, axis, and skull in three dimensions. This lets us measure the specific direction and degree of misalignment so any correction is tailored to your structure rather than a generic template.
We pair that structural picture with Tytron paraspinal infrared thermography, a completely non-contact, radiation-free scan that reads the heat patterns alongside the spine. Because skin temperature is partly regulated by the nervous system, asymmetrical thermal patterns can offer an objective window into how your nervous system is functioning around the upper neck, and they give us a way to track change over time rather than relying on how you happen to feel on a given day.
The Knee Chest Upper Cervical technique
Our correction method is the Knee Chest Upper Cervical technique, a low-force, precise adjustment delivered while you rest in a supported, knee-chest position. There is no twisting of the neck, no aggressive rotation, and no popping or cracking. Instead, the contact is specific and gentle, designed to encourage the atlas back toward its proper relationship with the skull and axis. For people who are nervous about having their neck manipulated, and understandably so, this style of care is often a welcome relief. The goal is to reduce the upper cervical misalignment so the downstream compensations, including the interscapular tension, have a reason to unwind on their own.
You can learn more about the philosophy behind this work on our upper cervical chiropractic care page.
Customized care plans, not one-size-fits-all
Because everyone’s structure, history, and goals are different, we build customized care plans around you. Your plan reflects your imaging findings, your thermographic patterns, how your body is holding its corrections, and how you are responding over time. We believe in a clear, individualized path rather than a guessing game.
Ready to Get to the Root of Your Interscapular Pain?
If you are tired of chasing a knot that never quite leaves, we would be glad to help you understand what is actually driving it. Call Lavender Family Chiropractic at (941) 243-3729 to ask questions or schedule a consultation. You can also book directly through our online new-patient scheduling. We are located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, right at the corner of University and Whitfield, convenient to Sarasota, Bradenton, and Lakewood Ranch.
What the Research Says
We believe in being transparent about the science that informs our thinking. The studies below are peer-reviewed and publicly available. They do not study our specific technique, and they do not promise any particular outcome, but they help explain the anatomy and referral mechanisms discussed throughout this article.
- The GBD 2021 global analysis of neck pain published in The Lancet Rheumatology estimated that neck pain affected roughly 203 million people worldwide in 2020 and projected cases to rise to about 269 million by 2050, underscoring how common and disabling neck-related pain is across the global population.
- The multispecialty international consensus practice guidelines on interventions for cervical (facet) joint pain, in Regional Anesthesia and Pain Medicine review the evidence that the cervical facet (zygapophysial) joints are a well-recognized source of chronic neck pain and characteristic referred pain, and they detail how these joints, innervated by the cervical dorsal rami, are diagnosed and treated.
- The study Referred pain distribution of the cervical zygapophyseal joints and cervical dorsal rami, published in Pain (Fukui et al., 1996) stimulated cervical joints and dorsal rami in patients and mapped where the pain was felt, showing that lower cervical segments refer pain into the shoulder-girdle and interscapular region, direct evidence that neck structures can produce upper-back pain.
- The paper Cervical Zygapophysial Joint Pain Maps, published in Pain Medicine (Cooper et al., 2007) analyzed the pain patterns reported by patients with confirmed cervical facet joint pain and found segment-specific referral zones, including lower cervical levels referring toward the superomedial and interscapular scapular region.
- A retrospective review of an ultrasound-guided technique for interscapular, mid-thoracic myofascial pain, in a PMC-indexed report (2024) described medial periscapular pain involving the trapezius, rhomboids, levator scapulae, and dorsal scapular nerve, frequently associated with forward head posture, illustrating the muscle-and-nerve cluster tied to the neck that so often underlies interscapular symptoms.
Taken together, these sources support a central theme of this article: pain felt between the shoulder blades is commonly referred from, or driven by compensation at, the cervical spine, which is why care aimed only at the interscapular muscles may offer limited, temporary help.
Lifestyle Factors That Support Your Neck and Upper Back
Structural care works best alongside daily habits that reduce the load on your neck and shoulder blades. None of these are a substitute for professional evaluation, but they may help create an environment in which your body can hold its improvements.
Set up your desk and screen for a neutral neck
The single biggest driver of interscapular strain we see is the forward-head, rounded-shoulder posture that a poorly arranged workstation encourages. Raise your monitor so the top third of the screen is at eye level, which keeps your head balanced over your shoulders instead of drifting forward. Pull your chair in so you are not reaching for the keyboard, support your forearms, and keep your feet flat. If you work on a laptop, use an external keyboard and a stand so you are not constantly hunched over a low screen. Our article on correcting poor posture and straightening up offers a practical walkthrough.
Mind your phone
Looking down at a phone for hours loads the neck heavily. Bring the phone up toward eye level, take frequent breaks, and try to notice when your head has drifted forward. Small, frequent corrections beat occasional heroic stretches.
Move often and strengthen the scapular stabilizers
The upper back is not designed to hold one position all day. Set a timer to stand, roll your shoulders back, and gently draw your shoulder blades down and together every 30 to 60 minutes. Over time, gentle strengthening of the middle and lower trapezius and the rhomboids, the muscles that retract and stabilize the shoulder blades, may help counteract the pull of a forward posture. Simple movements like scapular squeezes, wall angels, and rows, performed comfortably and without straining a painful neck, are a reasonable starting point. If a movement sharply increases neck or interscapular pain, ease off and ask us about it.
Sleep in a neck-friendly position
You spend a large fraction of your life in bed, so your sleep posture matters. Aim to keep your neck in a neutral position: a pillow that fills the gap between your head and the mattress without propping your head too far forward or letting it fall back. Back and side sleeping tend to be kinder to the neck than stomach sleeping, which forces the head into prolonged rotation. If you consistently wake with interscapular or neck pain, your pillow and position are worth a careful look.
Manage stress and breathing
Stress lives in the upper trapezius and the muscles of the neck and shoulders. When you are tense, you tend to elevate and brace your shoulders, feeding the very pattern that produces interscapular pain. Slow, diaphragmatic breathing and regular decompression, whether that is a walk on Siesta Key, time outdoors, or simple breathing breaks during the workday, can lower the baseline tension your postural muscles carry.
Serving Sarasota and Surrounding Communities
Lavender Family Chiropractic is proud to serve patients from across the region who are looking for gentle, upper-cervical-focused neck pain treatment. Our office at the corner of University and Whitfield is convenient to Sarasota, Bradenton, Lakewood Ranch, Venice, Palmer Ranch, Osprey, Siesta Key, Longboat Key, Lido Key, University Park, Parrish, Ellenton, Myakka City, Punta Gorda, and St. Petersburg. Whether you are commuting from the beaches, coming in from the ranch communities to the east, or driving down from the Bradenton and Ellenton area, we aim to make focused upper cervical care accessible. If you would like directions or have questions about getting here, our contact page has everything you need.
Top 15 Questions About Neck Pain Between the Shoulder Blades
1. Why does the pain between my shoulder blades keep coming back even after massage? Because massage treats the muscle where you feel the pain, but if the true driver is a compensation pattern rooted in the neck, the muscle has a reason to tighten again. Addressing the upper cervical alignment aims at the source rather than the symptom.
2. Can a problem in my neck really cause pain in my upper back? Yes. This is called referred pain. The cervical nerve roots and dorsal rami are wired so that irritation in the neck can be felt in the shoulder-girdle and interscapular region. Published pain-mapping research has documented these patterns directly.
3. What is the levator scapulae, and why does it matter so much? It is a muscle that connects the upper four cervical vertebrae to the upper inner corner of your shoulder blade, and it is supplied by nerves from the mid and upper neck. That dual attachment makes it a direct bridge that can carry a neck problem straight to the interscapular area.
4. What does the atlas (C1) have to do with pain between my shoulder blades? The atlas sits at the top of the neck and helps keep your head level. If it shifts, your body compensates all the way down the chain, loading the muscles that anchor your shoulder blades. That sustained compensation often shows up as interscapular pain.
5. Is the Knee Chest Upper Cervical technique going to crack or twist my neck? No. It is a low-force, specific correction performed in a supported position, with no twisting, cracking, or popping. Many patients choose it precisely because they are uncomfortable with forceful neck manipulation.
6. Do you take my insurance? We are a cash-pay, out-of-network practice, which means we do not bill insurance directly. We provide a superbill you can submit to your insurance company for possible out-of-network reimbursement, depending on your individual plan. This model lets us focus fully on your care rather than on insurance requirements.
7. Do you sell packages or make me prepay for a bunch of visits? We build customized care plans based on your imaging, your findings, and how your body responds. Your plan is individualized to you rather than a generic package, and we are always happy to explain it clearly before you begin.
8. Why do you use 3D CBCT imaging and thermography? Because the upper cervical spine is small and individual, and precision matters. The 3D CBCT scan shows the true, three-dimensional orientation of your atlas and axis so corrections are specific to your anatomy, and Tytron thermography gives an objective, non-contact way to monitor your nervous system’s patterns over time.
9. When is upper back pain an emergency? Seek urgent medical care right away if interscapular or upper-back pain comes with chest pressure or pain, shortness of breath, sweating, nausea, or pain spreading to the jaw or arm, which can signal a heart problem, and call 911 in that situation. Also seek prompt evaluation for sudden severe or tearing pain, pain with fever, unexplained weight loss, relentless night pain, or new weakness or numbness. These are not situations to handle with a chiropractor first; they need medical assessment. We screen for these red flags and will refer you appropriately.
10. Can poor posture alone cause this kind of pain? Posture is a major contributor. Forward head and rounded shoulders load the interscapular muscles and the cervical joints, and over time this can produce and perpetuate pain. Addressing posture and the underlying neck mechanics together tends to be more helpful than either alone.
11. How long before I might notice a difference? Everyone is different, and we cannot promise a timeline or a specific result. Some people notice changes relatively early, while others with long-standing compensation patterns take more time. We track your progress objectively so we can see how your body is responding.
12. Is upper cervical care safe? The Knee Chest Upper Cervical technique is a gentle, low-force approach, and we screen carefully before beginning care to make sure it is appropriate for you. If your situation calls for medical evaluation first, we will tell you.
13. I mostly have neck pain, not shoulder blade pain. Is this still relevant? Yes. Neck pain, upper-back pain, and interscapular pain frequently share the same underlying mechanics. Our neck pain resource covers the broader picture, and the upper cervical approach applies across these overlapping complaints.
14. Will I need to keep coming forever? Your care plan is customized and goal-oriented. We will discuss what makes sense for your situation, and the plan reflects your findings and response rather than an open-ended commitment you cannot understand.
15. What should I do first if I think my neck is the source? The simplest first step is a conversation. Call us at (941) 243-3729 or book online, and we will help you determine whether upper cervical care is a reasonable fit or whether you should be evaluated elsewhere first.
Take the Next Step Toward Natural Neck Pain Relief
Pain between the shoulder blades is exhausting, especially when nothing you do at the spot itself seems to help for long. The reason may be that the ache is a messenger from higher up, at the top of your neck, where the atlas and axis quietly organize your posture and where the nerves that run your shoulder-blade muscles begin. Gentle, precise upper cervical care is designed to address that root pattern rather than chase the symptom.
If you are in Sarasota, Bradenton, Lakewood Ranch, Venice, or anywhere in between, we would be honored to help you understand what is really going on. Call Lavender Family Chiropractic at (941) 243-3729, book your visit through our new-patient scheduling page, or stop by our office at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, at the corner of University and Whitfield. And if anything about your pain fits the emergency red flags described above, please seek medical care first; we will always be here once you have been safely evaluated. When you are ready, reach us at (941) 243-3729, and let us help you get to the root of it.