By Dr. Rusty Lavender — Lavender Family Chiropractic, Sarasota, FL
Craniocervical instability: If your head sometimes feels too heavy for your neck to hold, if a headache builds at the base of your skull when you are upright and eases when you lie down, or if dizziness, brain fog, and strange waves of fatigue have become part of your daily life, you may have started searching for answers. Somewhere in that search, a term keeps appearing: craniocervical instability, often shortened to CCI. It describes excessive or abnormal movement at the junction where your skull meets the top of your spine, and it has become one of the most talked-about topics among people living with hard-to-explain neurological and autonomic symptoms.
Here at Lavender Family Chiropractic in Sarasota, Florida, we hear these stories every week. People arrive after months or years of appointments, tests, and referrals, still looking for a framework that makes their experience make sense. This guide is written to help you understand the signs and symptoms commonly associated with craniocervical instability, why they happen, which symptoms are genuine red flags that call for urgent medical attention, and how precise upper cervical chiropractic care may fit into a thoughtful, coordinated plan.
Before we go any further, we want to be direct and honest with you, because honesty is the foundation of trust. The symptoms described in this article overlap with many different conditions. Having several of them does not confirm that you have craniocervical instability. True structural CCI is a medical diagnosis that requires specialized imaging and clinical evaluation, usually by physicians who focus on the craniocervical junction. Upper cervical chiropractic care does not repair ligaments or reverse structural instability, and it is not a substitute for medical evaluation. What careful, low-force upper cervical care can do is assess how well your head is balanced over your atlas, address alignment and nervous-system tension at the top of the neck, and help coordinate your care with the right providers. Our goal in this guide is to help you understand your body better and to encourage proper evaluation rather than self-diagnosis.
The Common Signs and Symptoms of Craniocervical Instability
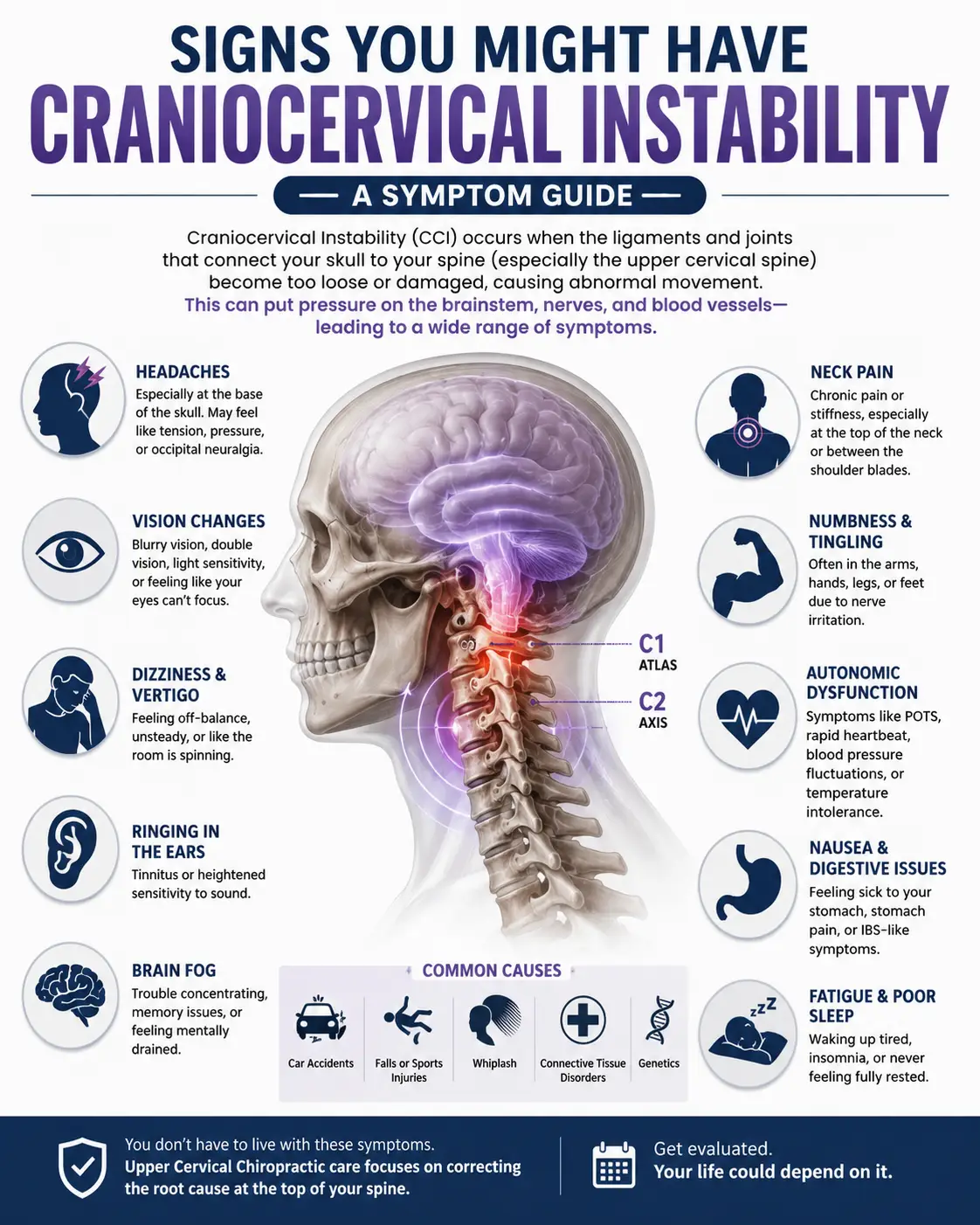
Craniocervical instability produces a cluster of symptoms that can feel bewildering precisely because they span so many systems at once. One day it feels like a neck problem, the next like a brain problem, and the day after like a heart or stomach problem. That is part of what makes the craniocervical junction so unique: it sits at the crossroads of the skull, the upper spine, the brainstem, and the nervous-system pathways that regulate much of what your body does automatically. Below are the signs and symptoms people most often describe.
A head that feels too heavy, or the “bobblehead” sensation
Perhaps the most characteristic complaint is the feeling that your head is too heavy for your neck to support. People describe needing to hold their head up with a hand, cradling the back of the skull against a chair or pillow, or feeling as though the head might “bobble” or wobble on top of the spine. Some call it a bobblehead feeling. This sensation often worsens with prolonged upright activity, reading, screen time, or carrying anything, and it tends to ease when the head is fully supported or when lying down. If this description resonates, our companion article on why the head feels too heavy and its link to vertigo explores this experience in more depth.
A base-of-skull headache that is worse upright and better lying down
A hallmark pattern reported with craniocervical instability is a headache that concentrates at the base of the skull, in the suboccipital region where the head meets the neck. What makes this pattern notable is its positional nature: it frequently intensifies when standing or sitting upright and eases, sometimes considerably, when reclining or lying flat. Many people notice that the headache builds over the course of the day and improves after rest. This upright-worse, lying-down-better quality is one of the details that prompts clinicians to think carefully about the craniocervical junction, although similar patterns can appear with other conditions as well.
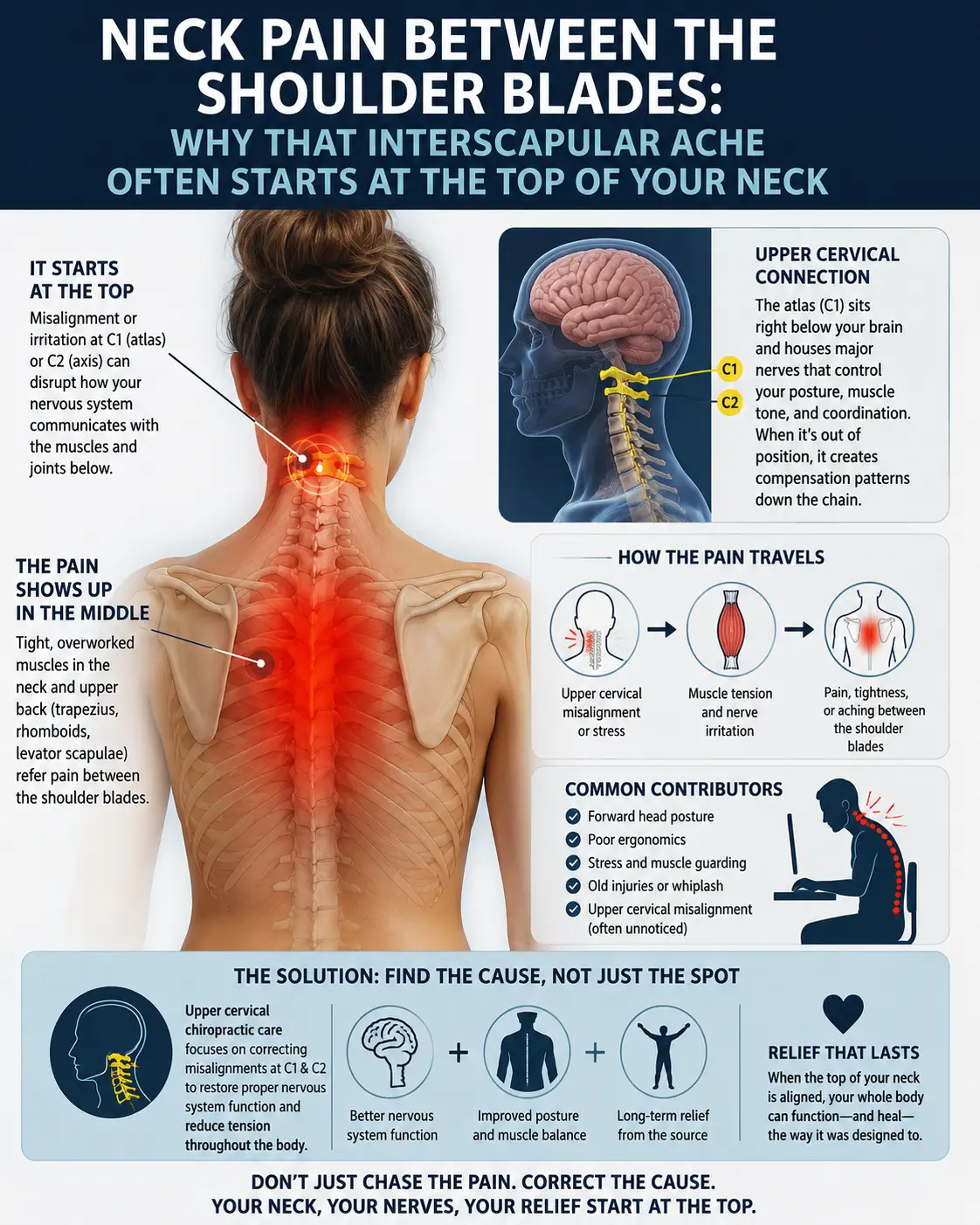
Neck pain and a persistent sense of instability
Neck pain is common, but the quality people describe with suspected CCI often goes beyond ordinary stiffness. They report a sense that the neck is unstable, loose, or unable to “lock in,” a feeling that certain movements produce a clunk, catch, or grinding, or an urge to constantly reposition and brace the neck. Some feel most comfortable in a cervical collar or with the neck fully supported. Pain may radiate into the shoulders, upper back, or the back of the head.
Dizziness, imbalance, and unsteadiness
Dizziness is one of the most frequently reported symptoms. It can take the form of true spinning (vertigo), a floating or rocking sensation, lightheadedness, or a general feeling of being off-balance and unsteady on the feet. People often describe difficulty walking in a straight line, bumping into door frames, or feeling worse in busy visual environments like grocery store aisles. Because the upper neck feeds an enormous amount of positional information to the brain, disturbances here can contribute to a sense that the world is not quite stable.
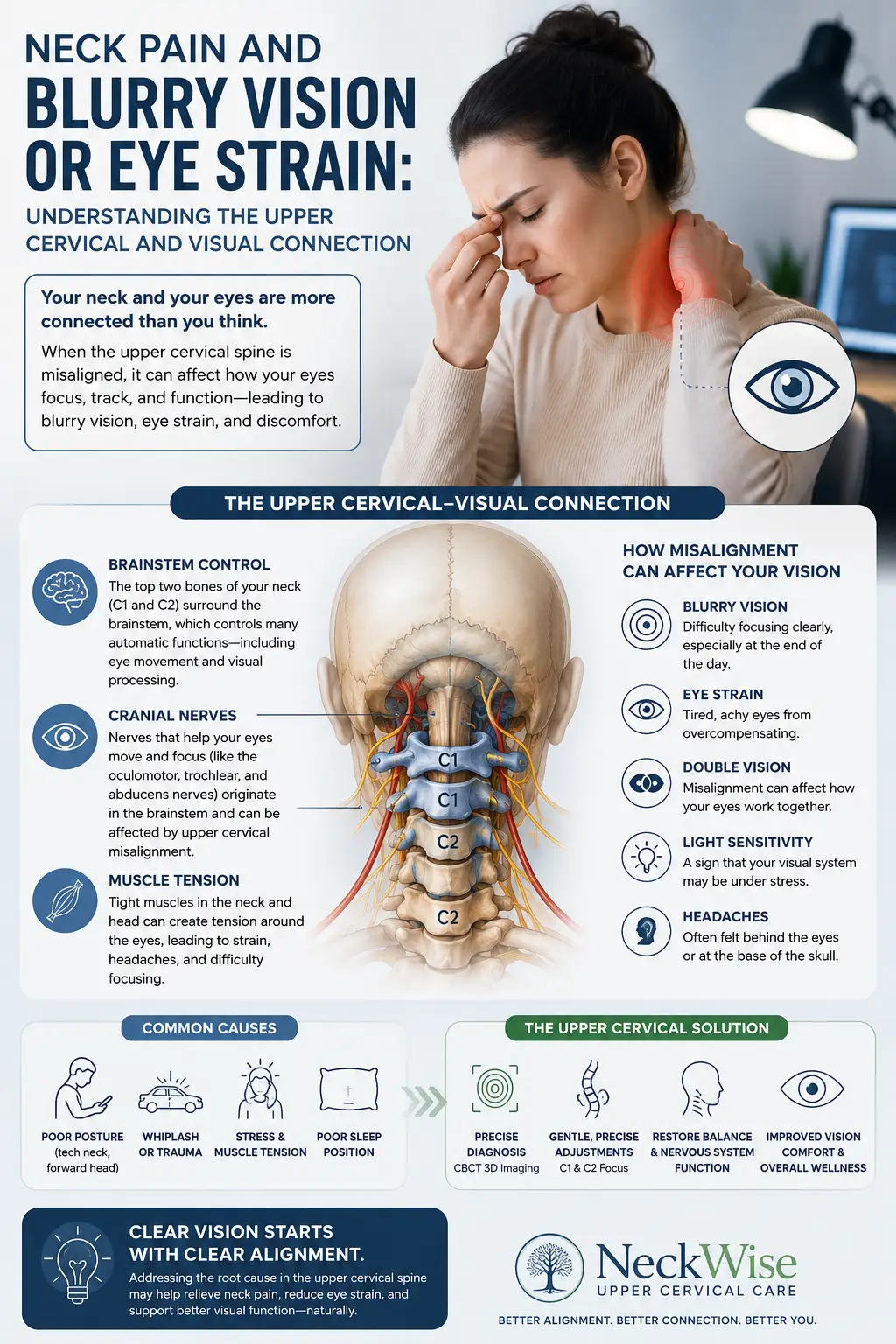
Visual disturbances
Visual symptoms are common and can be unsettling. People describe blurred vision, difficulty focusing, sensitivity to light, trouble tracking moving objects, eye strain, or a sense that their eyes and head are not coordinating well. Some notice that reading or screen work quickly triggers other symptoms such as headache or nausea.
Brain fog and cognitive fatigue
The phrase brain fog captures a real and frustrating experience: trouble concentrating, word-finding difficulty, short-term memory lapses, mental fatigue after brief effort, and a sense of moving through cognitive molasses. Many people find this symptom especially demoralizing because it interferes with work, parenting, and conversation, and because it is invisible to others.
Profound fatigue
Fatigue associated with suspected craniocervical instability is often out of proportion to activity. People describe waking unrefreshed, crashing after minor exertion, and needing to lie down to recover. Because lying down often relieves multiple symptoms at once, some people find themselves spending more and more time horizontal, which can compound deconditioning and low mood.
Autonomic symptoms: heart rate and blood pressure swings, digestive changes
Some of the most striking symptoms are autonomic, meaning they involve the body’s automatic regulatory systems. People report a racing or pounding heart, especially on standing, blood pressure that swings, lightheadedness or near-fainting when upright, temperature dysregulation, sweating changes, and digestive complaints such as nausea, bloating, early fullness, or irregular motility. This overlap with dysautonomia and POTS is well recognized, and we explore it further in our article on dysautonomia and POTS. Again, the presence of these symptoms does not confirm CCI; they can arise from many causes and deserve careful medical evaluation.
Why These Symptoms Happen: Mechanisms at the Craniocervical Junction
To understand why a single region can produce such a wide-ranging symptom picture, it helps to appreciate the anatomy of the craniocervical junction, or CCJ. This is the area where the base of the skull (the occiput), the first cervical vertebra (the atlas, or C1), and the second cervical vertebra (the axis, or C2) come together. It is one of the most mobile and most delicately balanced regions of the entire spine, designed to allow you to nod, rotate, and tilt your head across a remarkable range while protecting the structures that pass through it.
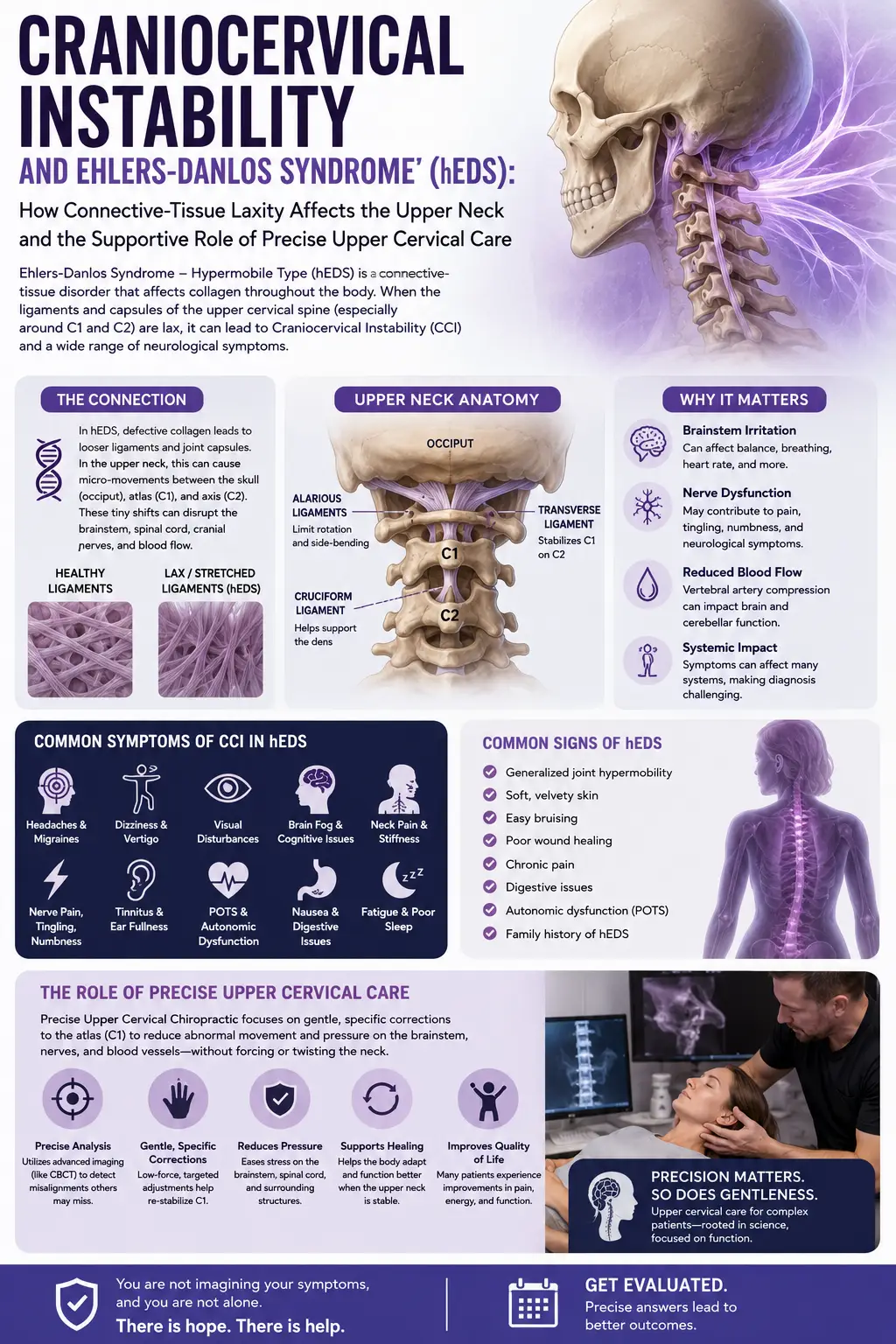
Several features make this region so consequential. First, the brainstem transitions into the spinal cord right here. The brainstem is responsible for an extraordinary range of functions, including aspects of consciousness, balance, eye movement coordination, and the regulation of heart rate, blood pressure, breathing, and digestion. When there is abnormal movement or mechanical stress at the CCJ, the theory is that these sensitive neural structures can experience irritation or altered dynamics, which may help explain why symptoms cross so many systems at once. A detailed clinical description of this constellation, sometimes called cervical medullary syndrome, has been documented in the medical literature in patients with connective tissue disorders and craniocervical instability.
Second, the stability of this junction depends heavily on ligaments rather than on bony interlocking. Strong ligaments, including the alar and transverse ligaments and the broader ligamentous complex, hold the skull and upper vertebrae in proper relationship and limit excessive motion. When these ligaments are lax, injured, or inherently more elastic, as can occur in hereditary connective tissue disorders such as Ehlers-Danlos syndrome, the junction may permit more movement than it should. A thorough anatomic and functional review of these ligaments explains how each contributes to stability and why their integrity matters so much for protecting the neural structures nearby.
Third, this region is dense with autonomic and sensory pathways. The upper cervical spine sends a huge volume of proprioceptive information, data about position and movement, to the brain. When that input is disturbed, it can conflict with information from the eyes and the inner ear, producing dizziness, imbalance, and visual difficulty. The region also lies near pathways associated with the vagus nerve and other autonomic circuitry that help govern heart rate, blood pressure, and digestion. Mechanical stress or altered signaling in this area is one proposed reason that autonomic symptoms so often travel alongside neck and head complaints.
It is worth emphasizing that these are mechanisms and models, not certainties in every individual case. The human nervous system is complex, and symptoms rarely map onto a single tidy cause. This is precisely why proper evaluation matters and why we approach every person as an individual rather than assuming that a familiar symptom pattern always points to the same source.
Symptoms That Are Red Flags
Some symptoms are not something to research, monitor, or bring to a routine appointment. They are signals that warrant urgent medical attention, sometimes emergency care. If you are experiencing any of the following, please treat them seriously and seek prompt medical evaluation. Chiropractic care is not the appropriate first response to these signs.
- Progressive weakness in the arms or legs, especially if it is worsening over hours or days
- New or worsening problems with coordination, such as dropping objects, clumsiness of the hands, or an unsteady, stumbling gait
- Changes in speech, such as slurring, or changes in swallowing, such as choking or difficulty getting food down
- Fainting or repeated near-fainting episodes
- New numbness or tingling that is spreading, particularly around the mouth, in all four limbs, or across the body
- Sudden, severe headache unlike any you have had before
- Vision loss, double vision that does not go away, or new difficulty with eye movements
- Loss of bladder or bowel control
- Any rapidly changing neurological symptoms
These red-flag symptoms can indicate that neural structures at or near the craniocervical junction, or elsewhere, are under significant stress, or they may point to another serious condition entirely. In any of these situations, the right move is to contact your physician promptly or go to the emergency department. We would always rather you be evaluated urgently and reassured than wait and wonder. When you come to our office, part of our role is to screen for exactly these kinds of signs and to make sure you are directed to appropriate medical care when that is what the situation calls for.
Conditions That Can Look Like CCI
One of the most important messages in this entire guide is that many conditions produce symptoms nearly identical to those associated with craniocervical instability. This is not a minor caveat; it is central to getting the right care. Self-diagnosing CCI from a symptom list is understandable when you are suffering and searching, but it can lead you down the wrong path. Here are some of the conditions whose symptoms overlap substantially.
Migraine and other primary headache disorders can produce head pain, light sensitivity, visual disturbance, nausea, dizziness, and brain fog. Vestibular migraine in particular can be difficult to distinguish from other causes of dizziness. Vestibular disorders, including benign paroxysmal positional vertigo, vestibular neuritis, and Meniere’s disease, can cause vertigo, imbalance, and nausea. Concussion and post-concussion syndrome can produce headache, fog, fatigue, and dizziness that linger for months.
Dysautonomia and postural orthostatic tachycardia syndrome (POTS) can cause heart-rate and blood-pressure changes on standing, lightheadedness, fatigue, brain fog, and digestive symptoms. Notably, dysautonomia can coexist with upper cervical issues, which is part of why these pictures are so tangled. Anxiety and panic disorders can generate a racing heart, dizziness, chest tightness, brain fog, fatigue, and a sense of unreality, and they can also accompany chronic illness rather than being the sole cause. Thyroid disorders, anemia, sleep disorders, and medication side effects can all contribute to fatigue, fog, and lightheadedness. Cervical spine conditions such as disc problems, arthritis, or muscle-based neck pain can cause overlapping neck and head symptoms without any instability at all.
Because so many possibilities exist, proper evaluation matters. That may include working with your primary care physician, a neurologist, an ear-nose-and-throat or vestibular specialist, a cardiologist or autonomic specialist for orthostatic symptoms, and, where structural craniocervical instability is genuinely suspected, physicians who specialize in the craniocervical junction and can order and interpret the specialized imaging required to diagnose it. Our role is to be one thoughtful part of that larger picture, not to replace it.
Why the Upper Neck (Atlas and Axis) Is Central, and How Precise Upper Cervical Care Fits
Given everything above, you can see why the atlas and axis, the top two vertebrae, occupy such a central place in this conversation. They are the mechanical foundation on which your roughly ten-to-twelve-pound head balances, and they sit closest to the brainstem and the dense web of neural and autonomic pathways described earlier. When the head is not well balanced over this foundation, the muscles, joints, and nervous system of the upper neck can carry chronic tension and altered signaling. This is the domain of upper cervical chiropractic care.
At Lavender Family Chiropractic, we practice a specialized, focused approach centered on the upper neck, and we want to describe exactly what that involves and, just as importantly, what it does not do.
We begin with careful measurement rather than assumption. Using 3D cone beam computed tomography (CBCT) imaging, we obtain a detailed three-dimensional view of your unique upper cervical anatomy and how your head is aligned over the atlas. This lets us base our care on your individual structure rather than a generic model. We also use Tytron paraspinal infrared thermography, a non-touch scan that reads patterns of heat along the spine as an indirect reflection of nervous-system activity, giving us an objective way to track how your body is responding over time.
Our correction itself is delivered through the Knee Chest Upper Cervical technique. This is a precise, low-force adjustment. It is not high-velocity twisting or forceful cracking of the neck. Instead, it is a specific, gentle correction designed to encourage the head to rebalance over the atlas based on your imaging and measurements. Many people who have felt apprehensive about their neck are relieved to learn how controlled and gentle this approach is.
Now, the honest part, because it matters. Precise upper cervical care does not repair or tighten ligaments, and it does not reverse structural craniocervical instability. If a person has true, medically diagnosed structural instability, that is managed within a medical framework, and in some cases surgically, by specialists in the craniocervical junction. What our care can reasonably aim to do is assess and improve how your head is balanced over the upper neck, reduce mechanical tension and irritation in the region, support better nervous-system function, and provide careful screening so that anything requiring medical or emergency attention is identified and referred. We see ourselves as a coordinating partner. If your history and examination raise concern for structural instability or any red-flag findings, our job is to help point you toward the appropriate medical evaluation, not to keep you in our office indefinitely. Every plan is individualized through customized care plans built around your findings, your goals, and your response to care.
Ready to Understand What Is Happening in Your Neck?
If the symptoms in this guide sound familiar and you would like a careful, honest evaluation of your upper cervical alignment, we would be glad to help. You can reach Lavender Family Chiropractic at (941) 243-3729 or request an appointment through our online new patient scheduling page. Our office is located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, at the corner of University and Whitfield. We serve Sarasota and the surrounding communities, and we welcome your questions.
What the Research Says
Understanding craniocervical instability is an active area of medical study, particularly in the context of hereditary connective tissue disorders. The following peer-reviewed sources offer accurate, science-based context. We share them so you can read further and discuss them with your own providers. None of them describe our specific chiropractic technique, and we present them for educational understanding of the craniocervical junction, not as evidence that chiropractic care treats structural instability.
- Henderson FC, Francomano CA, Koby M, et al. Cervical medullary syndrome secondary to craniocervical instability and ventral brainstem compression in hereditary hypermobility connective tissue disorders: 5-year follow-up after craniocervical reduction, fusion, and stabilization. Neurosurgical Review, 2019. This study describes the cluster of brainstem-related symptoms (cervical medullary syndrome) that can accompany craniocervical instability in people with connective tissue disorders and reports on outcomes after surgical stabilization.
- Lohkamp LN, Marathe N, Fehlings MG. Craniocervical Instability in Ehlers-Danlos Syndrome: A Systematic Review of Diagnostic and Surgical Treatment Criteria. Global Spine Journal, 2022. This systematic review examines how craniocervical instability is diagnosed and surgically managed in Ehlers-Danlos syndrome and highlights the current lack of standardized criteria.
- Castori M, Voermans NC. Neurological manifestations of Ehlers-Danlos syndrome(s): A review. Iranian Journal of Neurology, 2014. This review surveys the wide range of neurological symptoms, including headache, dizziness, and autonomic complaints, that can occur in Ehlers-Danlos syndrome.
- Fiester P, Rao D, Soule E, et al. Anatomic, functional, and radiographic review of the ligaments of the craniocervical junction. Journal of Craniovertebral Junction and Spine, 2021. This review details the ligaments that stabilize the craniocervical junction and explains their roles in limiting excessive motion and protecting nearby neural structures.
- Canlı K, De Greef I, Van Looveren E, et al. The effects of physiotherapy on neck pain with associated symptoms, including cervicogenic dizziness and tinnitus: a systematic review. BMC Musculoskeletal Disorders, 2026. This systematic review evaluates conservative, physiotherapy-based approaches for neck pain accompanied by symptoms such as cervicogenic dizziness, illustrating how neck-related dysfunction can contribute to dizziness and related complaints.
What to Do If These Signs Sound Familiar
If you have read this far and recognized yourself in these descriptions, here is a calm, practical path forward.
First, take stock of urgency. Review the red-flag list above. If you are experiencing progressive weakness, coordination or speech or swallowing changes, fainting, or rapidly changing neurological symptoms, do not wait; contact your physician promptly or seek emergency care.
Second, if your symptoms are chronic and troubling but not red-flag emergencies, start keeping a simple symptom log. Note what makes symptoms better or worse, especially whether they improve when you lie down, how they relate to posture and activity, and how they change through the day. This information is genuinely valuable to every provider you see.
Third, build your team. Your primary care physician is a good starting point and can coordinate referrals to a neurologist, a vestibular or ENT specialist, an autonomic or cardiology specialist for orthostatic symptoms, and, where structural craniocervical instability is truly suspected, physicians who specialize in the craniocervical junction. Proper evaluation is how you avoid the trap of self-diagnosis.
Fourth, consider a careful upper cervical assessment as one part of that team-based approach. You are welcome to call our Sarasota office at (941) 243-3729 with questions before you decide. At Lavender Family Chiropractic, an evaluation includes 3D CBCT imaging of your upper cervical anatomy, Tytron thermography, a thorough history, and screening for anything that warrants medical referral. If we can help, we will explain how and why. If your situation calls for medical or emergency care instead, we will tell you that plainly. To go deeper on the overall condition, our comprehensive craniocervical instability resource is a helpful next read, and if dizziness and the heavy-head sensation are your main concerns, our article on craniocervical instability and vertigo may resonate.
Above all, be patient and persistent with yourself. Complex, multi-system symptoms take time to sort out, and you deserve providers who listen carefully and communicate honestly.
Serving Sarasota and Surrounding Communities
Lavender Family Chiropractic is proud to serve individuals and families throughout the Suncoast region. Our office at the corner of University and Whitfield is convenient to a wide area, and we welcome patients from Sarasota, Bradenton, Lakewood Ranch, Venice, Palmer Ranch, Osprey, Siesta Key, Longboat Key, Lido Key, University Park, Parrish, Ellenton, Myakka City, Punta Gorda, and St. Petersburg. Because we are a cash-pay, out-of-network practice, patients often travel to us from beyond these communities specifically for our focused upper cervical approach. Wherever you are coming from, we aim to make your first visit clear, unhurried, and informative.
Top 15 Questions About Craniocervical Instability and Upper Cervical Care
1. Do these symptoms mean I definitely have craniocervical instability? No. This is the most important question to answer honestly. The symptoms in this guide overlap with many conditions, including migraine, vestibular disorders, dysautonomia, POTS, anxiety, thyroid problems, and ordinary neck conditions. Having several of these symptoms does not confirm CCI. True structural craniocervical instability is a medical diagnosis that requires specialized imaging and clinical evaluation. Please use this guide to inform a conversation with qualified providers rather than to self-diagnose.
2. How is structural craniocervical instability actually diagnosed? It is diagnosed medically, typically by physicians who specialize in the craniocervical junction, using specialized imaging and detailed clinical criteria. As the research notes, standardized diagnostic criteria are still evolving, which is one reason expert medical evaluation is so important.
3. Can chiropractic care repair the ligaments or reverse instability? No. Precise upper cervical chiropractic care does not repair or tighten ligaments and does not reverse structural instability. What it can do is assess how your head is balanced over the atlas, address mechanical tension and nervous-system irritation in the upper neck, and screen for signs that need medical referral.
4. Is your technique the same as forceful neck “cracking”? No. We use the Knee Chest Upper Cervical technique, which is a precise, low-force correction guided by your imaging and measurements. It is not high-velocity twisting or forceful manipulation of the neck.
5. What are the red-flag symptoms that mean I should seek urgent care instead of booking a chiropractic visit?Progressive weakness in the arms or legs, new coordination problems, changes in speech or swallowing, fainting, spreading numbness, sudden severe headache, vision loss or double vision, loss of bladder or bowel control, and any rapidly changing neurological symptoms all warrant prompt medical attention or a visit to the emergency department. These are not situations to manage with routine chiropractic care.
6. Why do you use 3D CBCT imaging? 3D cone beam CT imaging gives us a detailed, three-dimensional picture of your individual upper cervical anatomy and how your head aligns over the atlas. This lets us tailor a precise correction to your unique structure rather than relying on assumptions.
7. What is Tytron thermography and why does it matter? Tytron paraspinal infrared thermography is a non-touch scan that reads heat patterns along the spine as an indirect reflection of nervous-system activity. It gives us an objective way to monitor how your body is responding to care over time.
8. Do you take insurance? We are a cash-pay, out-of-network practice. This allows us to spend the time and use the specialized imaging and technique that our approach requires, without being limited by insurance restrictions.
9. Can I still use my insurance benefits at all? We provide superbills, which are detailed receipts you can submit to your insurance company for possible out-of-network reimbursement. Whether you are reimbursed depends on your individual plan, so we encourage you to check your out-of-network benefits directly with your insurer.
10. How much will care cost? Because every person’s situation is different, care is organized through customized care plans based on your findings and goals. We will explain the details clearly and transparently before you commit to anything, so you can make an informed decision.
11. I think I might have POTS or dysautonomia. Is that related to my neck? Autonomic symptoms such as heart-rate and blood-pressure swings and digestive changes can travel alongside upper cervical issues, and the two can coexist. That said, dysautonomia and POTS require proper medical evaluation. Our article on dysautonomia and POTS explains the connection, and we are glad to coordinate with your medical team.
12. Why does my headache get better when I lie down? A base-of-skull headache that eases when lying flat and worsens when upright is a pattern sometimes associated with the craniocervical junction, though it can occur with other conditions too. It is a detail worth sharing with your providers, as it can help guide evaluation.
13. Could my dizziness be coming from my neck? The upper neck sends a large amount of position information to the brain, and disturbances there can contribute to dizziness and imbalance, sometimes called cervicogenic dizziness. However, dizziness has many possible causes, including vestibular and neurological conditions, so proper evaluation is important.
14. What happens at a first visit? A first visit includes a thorough history, 3D CBCT imaging of your upper cervical anatomy, Tytron thermography, and screening for anything that needs medical referral. We take time to explain what we find and whether our care is a good fit for you.
15. What if my evaluation suggests I need medical care rather than chiropractic? Then we will tell you plainly and help point you toward appropriate providers. We see ourselves as a coordinating partner in your overall care. Directing you to the right place is part of doing our job well.
Let’s Take the Next Step Together
If the signs in this guide sound familiar, you do not have to keep guessing on your own. A careful, honest evaluation can help you understand what is happening at the top of your neck and how it fits into your larger health picture. Call Lavender Family Chiropractic at (941) 243-3729, or request a visit through our new patient scheduling page. You can also learn more or reach us through our contact page. We are located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, at the corner of University and Whitfield, and we look forward to helping you find clarity and support.
Related Articles
- Craniocervical Instability: The Complete Guide — Start here for a comprehensive overview of CCI, its symptoms, causes, and how precise upper cervical care fits into a coordinated approach. This is our main pillar resource on the topic.
- Craniocervical Instability and Vertigo: Why Your Head Feels Too Heavy — A closer look at the heavy-head sensation, dizziness, and imbalance.
- Dysautonomia and POTS — Understanding autonomic symptoms and their connection to the upper cervical spine.