PPPD: If you’ve spent months — maybe years — feeling like you’re constantly rocking on a boat, swaying as you walk, floating instead of standing solidly, or just plain “off” no matter what you do, you may be dealing with one of the most under-recognized dizziness conditions in modern medicine: Persistent Postural-Perceptual Dizziness, often abbreviated as PPPD (pronounced “3PD” or “triple-P-D”).
PPPD is one of the most frustrating conditions we see at our office in Sarasota. It rarely shows up on imaging. Vestibular tests often come back close to normal. Inner ear specialists tell patients “everything looks fine.” And yet the dizziness is unrelenting — present nearly every day, worse in busy visual environments, worse with standing or walking, often paired with anxiety because patients feel like nobody can find what’s wrong with them.
Here at Lavender Family Chiropractic, located at 5899 Whitfield Avenue, Suite 107 at the corner of University and Whitfield in Sarasota, Dr. Rusty Lavender and Dr. Jacob Temple specialize in helping PPPD patients understand the upper cervical and nervous system component of their condition — a piece that is almost universally missed in conventional care. This blog will walk you through exactly what PPPD is, why it develops, what the current research says, and how upper cervical chiropractic care fits into helping the brain finally turn off the chronic “danger signal” driving the dizziness.
This article is part of our broader vertigo resource hub. To see how PPPD fits into the larger picture of dizziness conditions, we recommend starting with our main page on vertigo care in Sarasota with Dr. Jacob Temple.
What Is Persistent Postural-Perceptual Dizziness (PPPD)?
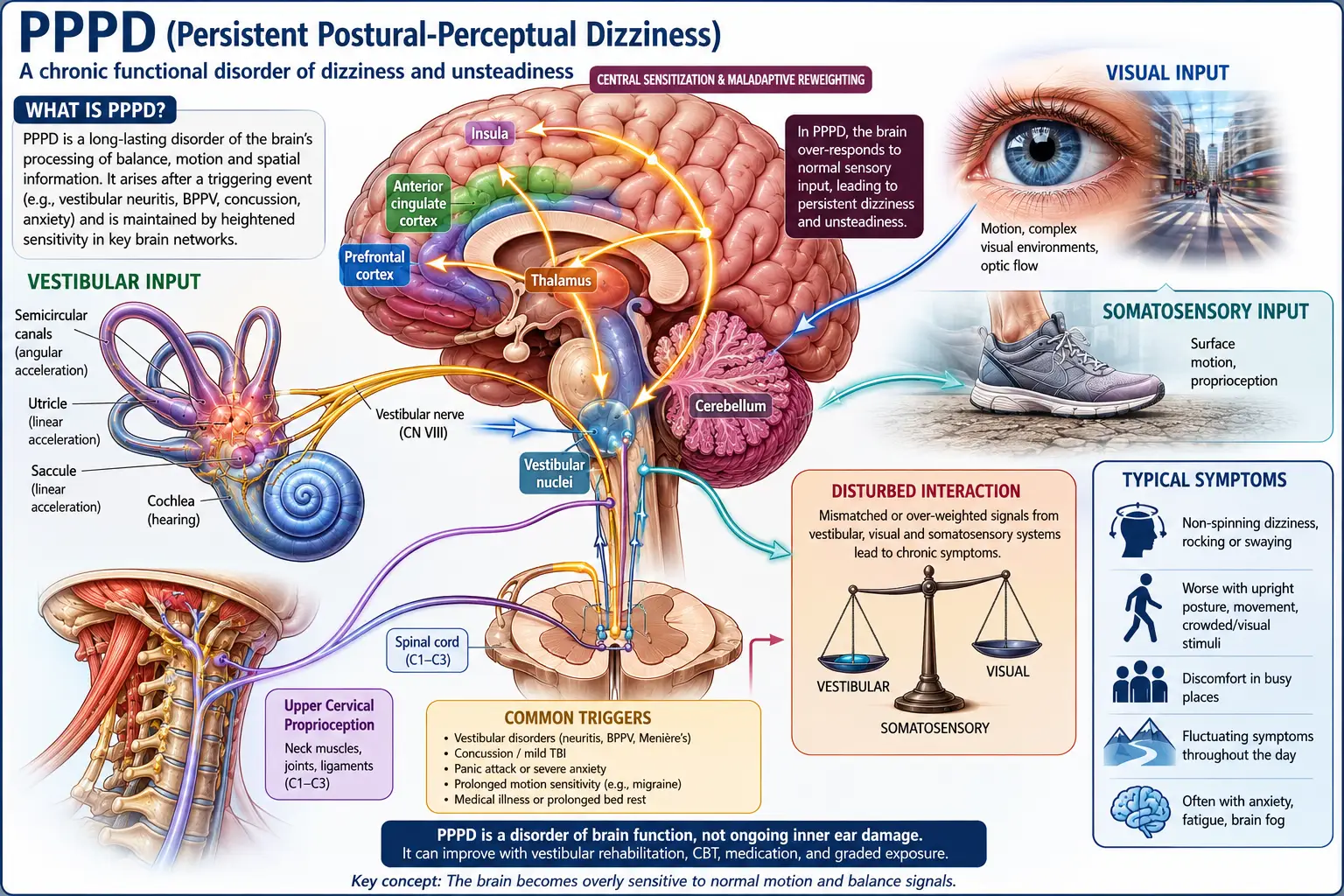
PPPD is a chronic vestibular disorder defined by ongoing, non-spinning dizziness, unsteadiness, and a sense of swaying or rocking that lasts at least three months. It was officially defined as a distinct disorder in 2015 by the Bárány Society, with formal diagnostic criteria established in 2017.
Patients with PPPD typically describe their symptoms in very specific ways:
- A constant rocking, swaying, or floating sensation
- Feeling like the floor is moving even when standing still
- Dizziness that’s present most of the day, most days
- Symptoms that get worse when standing upright
- Symptoms that get worse in busy visual environments — supermarkets, scrolling phones, driving, crowds, patterned floors, large screens
- Symptoms that get worse with active or passive motion
- Symptoms that don’t spin — there’s no rotational vertigo
- A sense of being “off” that’s hard to put into words but is unmistakably real
Critically, PPPD almost always starts after another vestibular event. The triggering event might be:
- A bout of vestibular neuritis or labyrinthitis
- An episode of BPPV
- A vestibular migraine attack
- A concussion or head injury
- A panic attack with vertigo
- A medical illness
- Sometimes psychological stress alone
The original event resolves — but the dizziness doesn’t. The brain stays stuck in a hypervigilant, motion-sensitive pattern long after the initial cause has healed. This is what makes PPPD different from other vestibular conditions: it’s not a problem of structural damage. It’s a problem of nervous system pattern. The brain has essentially learned to perceive itself as dizzy.
A 2025 study published in the European Journal of Neurology described PPPD as a “functional neurological disorder” — meaning it’s a problem with how the brain processes balance information, not a problem with the inner ear itself. According to current research, PPPD affects roughly 4 percent of the general population and is the second most common diagnosis among all vestibular patients, particularly in adults aged 30 to 50.
How PPPD Affects Your Nervous System and Sensory Processing
To understand why this condition is so persistent — and why upper cervical chiropractic care can make such a meaningful difference — you have to understand what’s actually happening in the brain.
Your balance is maintained by the brain integrating three sensory inputs:
- Vestibular input from your inner ear
- Visual input from your eyes
- Proprioceptive input from your joints and muscles, especially in the neck
In healthy balance, your brain weighs all three inputs and integrates them smoothly. In PPPD, the brain develops a maladaptive sensory weighting — meaning it leans too heavily on visual input and not enough on vestibular and proprioceptive input. This is why busy visual environments feel so overwhelming to PPPD patients. Their brain is overreliant on vision for balance, and when vision gets noisy (crowds, scrolling, patterns), the system overloads.
There’s also a threat-detection component. The brain regions responsible for processing balance overlap with the regions that process threat and anxiety. After a frightening vestibular event, the brain can effectively get “stuck” in high-alert mode — interpreting normal sensory input as dangerous and producing constant dizziness as a result. This is one of the reasons PPPD so frequently comes with anxiety, panic, and avoidance behaviors.
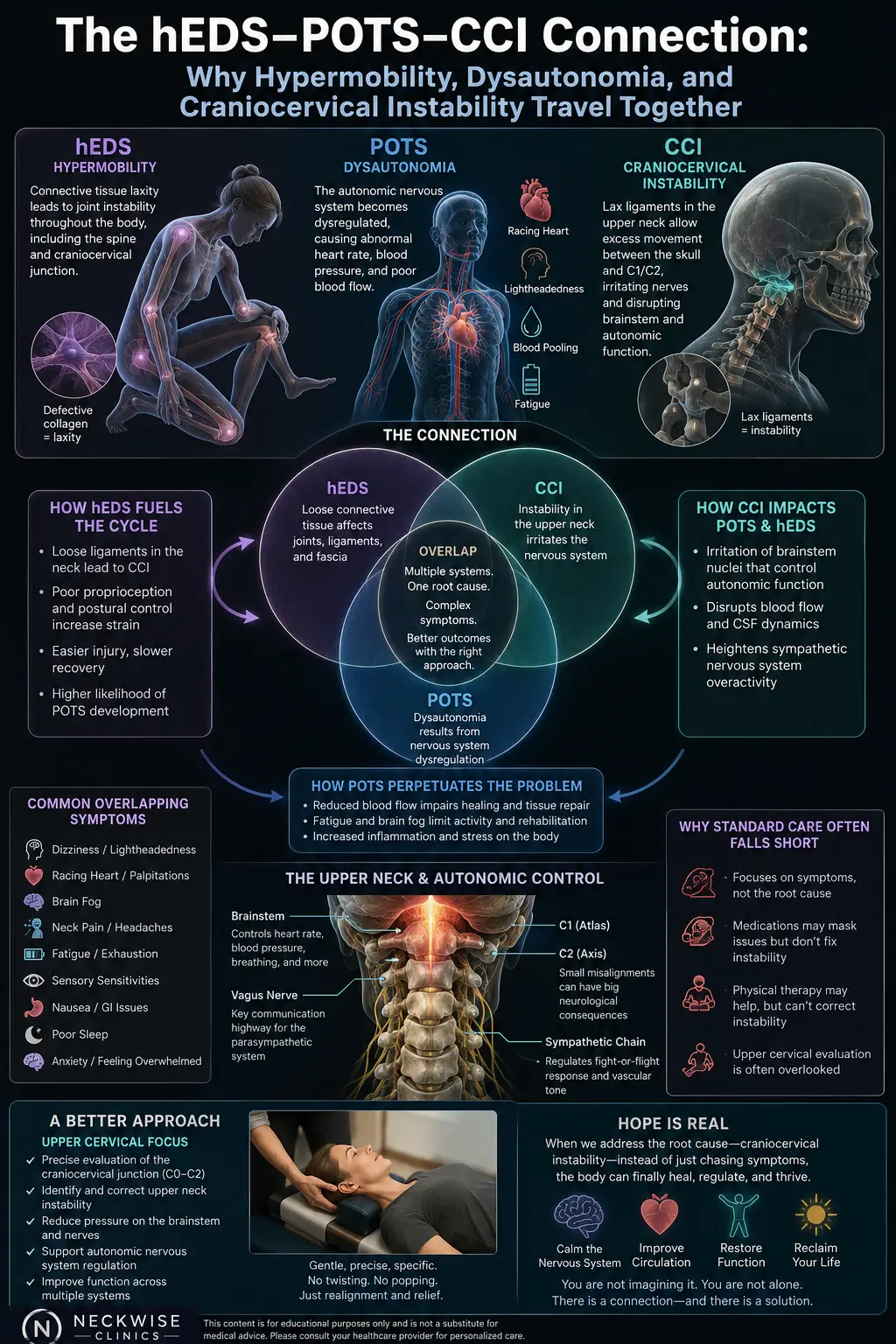
The upper cervical spine plays a powerful role in all of this through three pathways:
1. Proprioceptive input. The upper neck has the highest density of position-sensing receptors anywhere in the spine. When this input is accurate, the brain has reliable data to lean on, which reduces visual dependence. When this input is faulty due to upper cervical dysfunction, the brain has even more reason to rely on vision — which feeds directly into PPPD’s maladaptive pattern.
2. Brainstem signaling. The upper cervical spine sits adjacent to the brainstem and the vestibular nuclei — the very areas where this conditions altered processing takes place. Misalignment in this region can subtly interfere with the brain’s ability to recalibrate normal vestibular function.
3. Vagus nerve and autonomic balance. The vagus nerve exits the skull right next to the atlas (C1) and is critical for regulating the autonomic nervous system — including the threat-response state that often drives PPPD. Irritation of the vagus nerve from upper cervical dysfunction can keep the body in a chronic sympathetic-dominant state, amplifying the dizziness, anxiety, and hypervigilance.
There’s also a vascular component. The vertebral arteries pass through the bones of the upper cervical spine before supplying the brainstem, cerebellum, and inner ear. Subtle upper cervical dysfunction can affect blood flow to these areas, reducing the body’s ability to fully resolve sensory misintegration.
In PPPD, the nervous system is essentially stuck in a loop. The upper cervical spine is one of the most effective places to interrupt that loop.
Why the Upper Cervical Spine Matters in PPPD Recovery
Almost every patient we see at our Sarasota office has a story that includes some kind of upper cervical involvement — even if they don’t realize it.
The original triggering event was usually traumatic to the upper neck. Vestibular neuritis caused them to lie rigidly still for days, tensing every muscle in their upper neck. A concussion whipped their head on their neck even when the impact wasn’t direct. A vestibular migraine attack lasted hours and was accompanied by white-knuckle muscle bracing in the neck and shoulders. An episode of BPPV had them avoiding head movement for weeks. A panic attack drove their sympathetic nervous system into overdrive, locking up the suboccipital muscles.
Every one of these scenarios creates real, measurable upper cervical dysfunction — dysfunction that long outlives the original trigger. And as long as that dysfunction is present, the brain has another reason to stay in PPPD mode. Faulty proprioceptive signals coming from the neck reinforce the brain’s sense that something is wrong, which keeps the maladaptive sensory weighting in place.
This is why so many patients improve with vestibular rehabilitation but never fully resolve. Vestibular rehab addresses one input. It teaches the brain to better integrate vision and movement. But if the upper cervical spine continues to send unreliable proprioceptive data, the brain never has a complete, accurate sensory picture to work with.
Upper cervical chiropractic care is the missing input. When the atlas and axis are corrected, the neck begins sending clean, accurate proprioceptive signals again. The brain finally has the third input it’s been missing — and the maladaptive pattern starts to unwind.
This isn’t a quick fix for this condition. It’s a piece of the puzzle. But for many of our patients, it’s the piece that allows everything else they’re doing to finally start working.
Upper Cervical Chiropractic Care for PPPD: What to Expect
At Lavender Family Chiropractic, we take a careful, measured, and gentle approach with PPPD patients. We know you’ve been through a lot. We know you’ve been told a hundred different things by a hundred different specialists. And we know that anything involving the head and neck can be intimidating when your nervous system already feels on edge.
Here’s what your journey with us looks like.
Step One: Comprehensive Consultation
Your first visit starts with conversation. Dr. Lavender or Dr. Temple will sit down with you and listen to the full story — when the dizziness started, what triggered it, what diagnostic journey you’ve been on, what treatments you’ve tried, what makes you better, what makes you worse, and how PPPD has affected your daily life. This isn’t a rushed intake. PPPD is a complex condition, and we want to understand exactly what you’re dealing with.
Step Two: 3D CBCT Imaging and Neurological Scanning
Once we have your story, we use 3D CBCT X-ray technology to take three-dimensional images of your upper cervical spine. This advanced imaging shows us — down to the millimeter — exactly how your atlas (C1) and axis (C2) are positioned, and allows us to calculate the precise corrective vector your spine needs.
We pair this with paraspinal infrared thermography to assess how your nervous system is functioning along the spine. Thermography is particularly useful for PPPD patients because it shows us patterns of nervous system stress and sympathetic-dominant function that often parallel the dizziness experience.
Step Three: A Gentle, Specific Correction
Once we know exactly what needs to change, we deliver a precise upper cervical correction. This is not the type of chiropractic adjustment most people picture. There is no twisting, no popping, no cracking. We use the Advanced HIO Knee Chest Upper Cervical Technique (AHKC), one of the gentlest and most precise methods of upper cervical correction available.
For PPPD patients especially, gentleness matters. Your nervous system has been on high alert for months or years. Anything that feels aggressive or threatening can set you back. Our approach is built to work with your nervous system, not against it.
Step Four: Monitoring and Stabilizing the Pattern Change
The goal of upper cervical care for PPPD isn’t to adjust you weekly forever. The goal is to help your spine hold its corrected position so your nervous system can finally start changing its pattern. We track your progress visit by visit and adjust your care plan as your symptoms shift.
Most PPPD patients begin noticing small but meaningful changes within the first few weeks: less rocking, slightly more tolerance for visual environments, better sleep, less brain fog, less anxiety. Progress is often slow and stepwise — but it’s real, and it builds.
Have you been stuck in PPPD for months or years with no real answers? Call us at (941) 243-3729 or book a complimentary consultation online. We’ll help you understand whether upper cervical care fits into your recovery.
What the Research Says About PPPD
The science on PPPD has advanced significantly in recent years. Here’s what current research tells us.
A 2026 paper published in the European Journal of Neurology described PPPD as a functional neurological disorder driven by altered sensory integration in the brain — confirming that the condition is real, neurological, and treatable, despite the absence of clear structural abnormalities on standard imaging.
A 2025 systematic review and meta-analysis published in PMC examined the effect of vestibular rehabilitation therapy on PPPD patients and concluded that VRT produces meaningful reductions in dizziness and improvements in postural control — but with significant variability between patients. Importantly, the researchers noted that response to VRT depends heavily on overall nervous system function, suggesting that addressing co-existing factors (like upper cervical dysfunction) may amplify outcomes.
A 2025 review by Vestibular First confirmed that PPPD involves persistent functional alterations in the brain’s sensory and perceptual systems rather than structural injury — exactly the type of pattern that responds best to interventions that calm and reorganize nervous system function rather than treating a fixed structural problem.
A 5-year case series of 198 PPPD patients published earlier in Frontiers in Neurology confirmed that anxiety disorders and vestibular migraine are the most common precipitating conditions, and that cognitive behavioral therapy produces significant reductions in anxiety and dizziness over a six-month follow-up period.
Across the literature, the theme is consistent: PPPD is a brain-pattern condition, and effective treatment supports the brain’s ability to recalibrate. Upper cervical chiropractic care is one of the most direct ways to give the brain a clean, accurate proprioceptive input — which is precisely what the maladaptive PPPD pattern needs in order to resolve.
Lifestyle Habits That Support Recovery from PPPD
Beyond upper cervical care, daily habits make a major difference in PPPD recovery. Here’s what we recommend most often.
Don’t avoid movement. PPPD instincts will tell you to hold still, stay home, and avoid anything that triggers symptoms. The opposite is what your nervous system needs. Gradual, daily, progressive exposure to movement is essential. Avoidance reinforces the pattern.
Reduce visual overload — but don’t eliminate it. Scrolling phones, watching action movies on large screens, and prolonged exposure to busy visual environments can flare PPPD. But complete avoidance also strengthens visual dependency. The goal is gradual exposure within tolerance, building back resilience over time.
Sleep well. Your nervous system does its most important reorganization during sleep. Aim for 7–9 hours per night. Use a supportive pillow that maintains proper upper cervical alignment. Stomach sleeping is particularly disruptive and should be avoided.
Stay hydrated. Inner ear function depends on systemic hydration, and Florida heat and humidity make dehydration a daily risk. Half your body weight in ounces of water per day is a solid target.
Manage stress and anxiety. PPPD and anxiety are deeply intertwined. Breathing exercises, vagal-tone work, walks outside, and time away from screens are all powerful and free interventions. Cognitive behavioral therapy has strong research support for PPPD specifically and is worth considering.
Address related conditions. PPPD frequently coexists with vestibular migraine, anxiety, TMJ dysfunction, and post-concussion syndrome. For more on how multiple dizziness-related conditions overlap, our blog on TMJ pain in Sarasota and why your jaw issues might actually start in your neck is a useful companion read — there’s significant overlap between TMJ dysfunction and PPPD because both share upper cervical roots.
Be patient. PPPD recovery is rarely linear. Good weeks are followed by hard weeks. The trajectory matters more than any single day. With the right combination of upper cervical care, gradual exposure, stress management, and time, most patients see meaningful improvement.
Serving Sarasota and Surrounding Areas
Lavender Family Chiropractic is located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — right at the corner of University and Whitfield. We’re easy to reach from anywhere in the greater Sarasota region.
We proudly serve PPPD patients and others dealing with chronic dizziness from across the area, including:
- Sarasota, FL
- Bradenton, FL
- Lakewood Ranch, FL
- Venice, FL
- Osprey, FL
- Parrish, FL
- Ellenton, FL
- Siesta Key, FL
- Longboat Key, FL
- St. Pete, FL
- Tampa, FL
To learn more about the full region we serve, visit our areas we service page. No matter where you’re driving from, we’re set up to help.
Top 15 FAQs About PPPD
What is PPPD in simple terms?
PPPD is a chronic dizziness condition where your brain stays stuck in a hypersensitive, motion-perceiving state long after the original cause of dizziness has resolved. It’s not spinning vertigo — it’s a constant rocking, swaying, or floating feeling, especially when you’re upright or in busy visual environments.
How is PPPD different from vertigo?
True vertigo is the sensation that you or your surroundings are spinning. PPPD is a non-spinning sense of imbalance, rocking, or unsteadiness. Vertigo episodes typically come and go in distinct attacks; PPPD symptoms are present most of the time, most days.
Can PPPD be diagnosed with imaging?
Not directly. PPPD is a clinical diagnosis based on the pattern of symptoms and history, made after other causes have been ruled out. MRIs and CT scans are often performed to exclude more serious conditions, but they don’t show PPPD itself.
How long does PPPD last?
By definition, PPPD lasts at least three months. Without targeted treatment, it can persist for years. With the right combination of care — including upper cervical correction, vestibular rehabilitation, stress management, and gradual exposure — most patients see significant improvement, and some achieve full resolution.
What triggers PPPD?
PPPD is almost always triggered by an initial vestibular event — vestibular neuritis, BPPV, vestibular migraine, concussion, panic attack, or another illness that disrupts balance. The original event resolves, but the brain stays stuck in a hypervigilant pattern.
Why does PPPD get worse in busy visual environments?
In PPPD, the brain becomes overreliant on visual input for balance. Busy visual environments — supermarkets, crowds, scrolling phones, driving — overload the system and trigger dizziness. This is called “visually-induced dizziness” and is a hallmark of PPPD.
Is PPPD all in my head?
In the most literal sense, yes — PPPD is a functional brain pattern. But that does NOT mean it’s imaginary, psychological, or “not real.” PPPD involves measurable, documented alterations in how the brain processes balance information. It is a real condition that produces real, debilitating symptoms.
Can upper cervical chiropractic actually help PPPD?
Yes. While upper cervical care doesn’t directly “treat” PPPD as a diagnosis, it addresses one of the most overlooked contributors to the condition — faulty proprioceptive input from the upper neck. When that input is corrected, the brain has the accurate sensory data it needs to begin recalibrating.
Is upper cervical care safe for PPPD?
Yes. Upper cervical chiropractic is one of the gentlest forms of chiropractic care available. There is no twisting, popping, or cracking. Corrections are precise, light, and tailored to your specific anatomy — appropriate even for patients with the most sensitive nervous systems.
How long until I notice improvement?
Every PPPD patient is different. Some notice changes in the first few weeks; others take months. Progress is often gradual and stepwise rather than dramatic. The trajectory matters more than any single visit.
Do I need vestibular rehabilitation in addition to upper cervical care?
Many patients benefit from combining the two. Upper cervical care gives the brain accurate proprioceptive input; vestibular rehabilitation trains the brain to use all three sensory inputs together. The combination is often more effective than either alone.
Is PPPD related to anxiety?
PPPD and anxiety frequently coexist and reinforce each other. The brain regions involved in balance overlap with those involved in threat detection. This doesn’t mean PPPD is “caused by anxiety” — but managing anxiety is an important part of PPPD recovery.
Can PPPD come back after I’ve recovered?
It can flare during periods of high stress, illness, or another vestibular event. The good news is that patients who have learned how to manage PPPD generally know how to recognize and address flares before they become entrenched again.
Can children or older adults get PPPD?
PPPD is most common in adults aged 30 to 50, but it can occur at any age. Older adults with PPPD often have additional balance issues that complicate the picture; younger patients tend to recover more quickly with consistent care.
How do I know if Lavender Family Chiropractic is right for me?
If you’ve been diagnosed with PPPD, suspect you have PPPD, or have chronic dizziness that started after another vestibular event and won’t fully resolve, you’re an excellent candidate for an evaluation. Call (941) 243-3729 to schedule a complimentary consultation and we’ll help you figure out whether upper cervical care fits into your recovery plan.
You Don’t Have to Stay Stuck in PPPD
PPPD is one of the most disorienting and isolating conditions to live with — not because the symptoms are unbearable on their own, but because so few people understand what you’re going through. You don’t look sick. Your tests come back normal. People around you assume you’re better. But you know you’re not.
At Lavender Family Chiropractic, Dr. Rusty Lavender and Dr. Jacob Temple have spent years helping patients understand the upper cervical and nervous system component of PPPD — and helping them finally make real progress when nothing else has worked.
📞 Call us today at (941) 243-3729 📅 Or book your complimentary consultation online
Real recovery is possible. Let’s find your way out together.
Related Articles
- Vertigo Sarasota: Dr. Jake’s #1 Way to Resolve Dizziness
- Orthostatic Hypotension in Sarasota, Florida: How Upper Cervical Chiropractic Care Helps Resolve the Dizziness, Lightheadedness, and Faintness That Drops Your Blood Pressure Every Time You Stand
- TMJ Pain in Sarasota: Why Your Jaw Issues Might Actually Start in Your Neck
By Dr. Rusty Lavender and Dr. Jacob Temple — Lavender Family Chiropractic, Sarasota, FL