Labyrinthitis: If you’ve ever been hit with a sudden, terrifying combination of room-spinning vertigo, hearing loss, ringing in your ears, and overwhelming nausea — all at the same time — there’s a strong chance you experienced labyrinthitis. It’s one of the most disorienting inner ear conditions a person can go through, and the acute episode is severe enough that many patients end up in the emergency room thinking they’re having a stroke.
The frustrating part isn’t always the acute illness, though. It’s what comes after. Many labyrinthitis patients find themselves dealing with lingering dizziness, ongoing tinnitus, partial hearing loss, brain fog, and a sense of being “off” that drags on for weeks, months, or even years after the original infection has cleared. The body has technically healed, but the symptoms haven’t.
Here in Sarasota, Florida, at Lavender Family Chiropractic, located at 5899 Whitfield Avenue, Suite 107 at the corner of University and Whitfield, Dr. Rusty Lavender and Dr. Jacob Temple specialize in helping post-labyrinthitis patients address one of the most overlooked contributors to incomplete recovery: dysfunction in the upper cervical spine. This blog will walk you through exactly what labyrinthitis is, why it causes such severe symptoms, what current research shows, and how upper cervical chiropractic care fits into a complete recovery plan.
This article is part of our broader vertigo resource hub. For the full picture of how we approach dizziness as a whole, we recommend starting with our main page on vertigo care in Sarasota with Dr. Jacob Temple.
What Is Labyrinthitis?
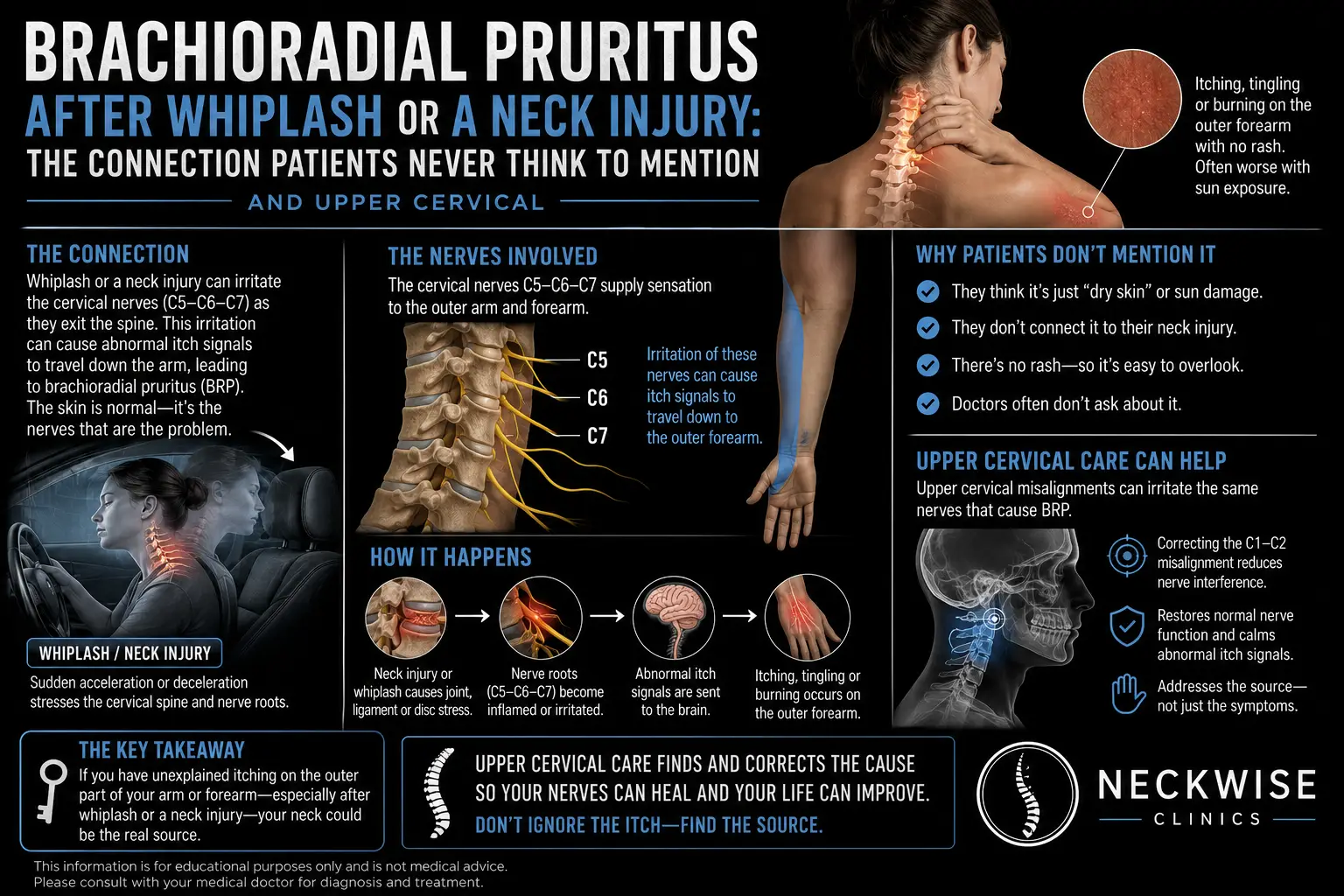
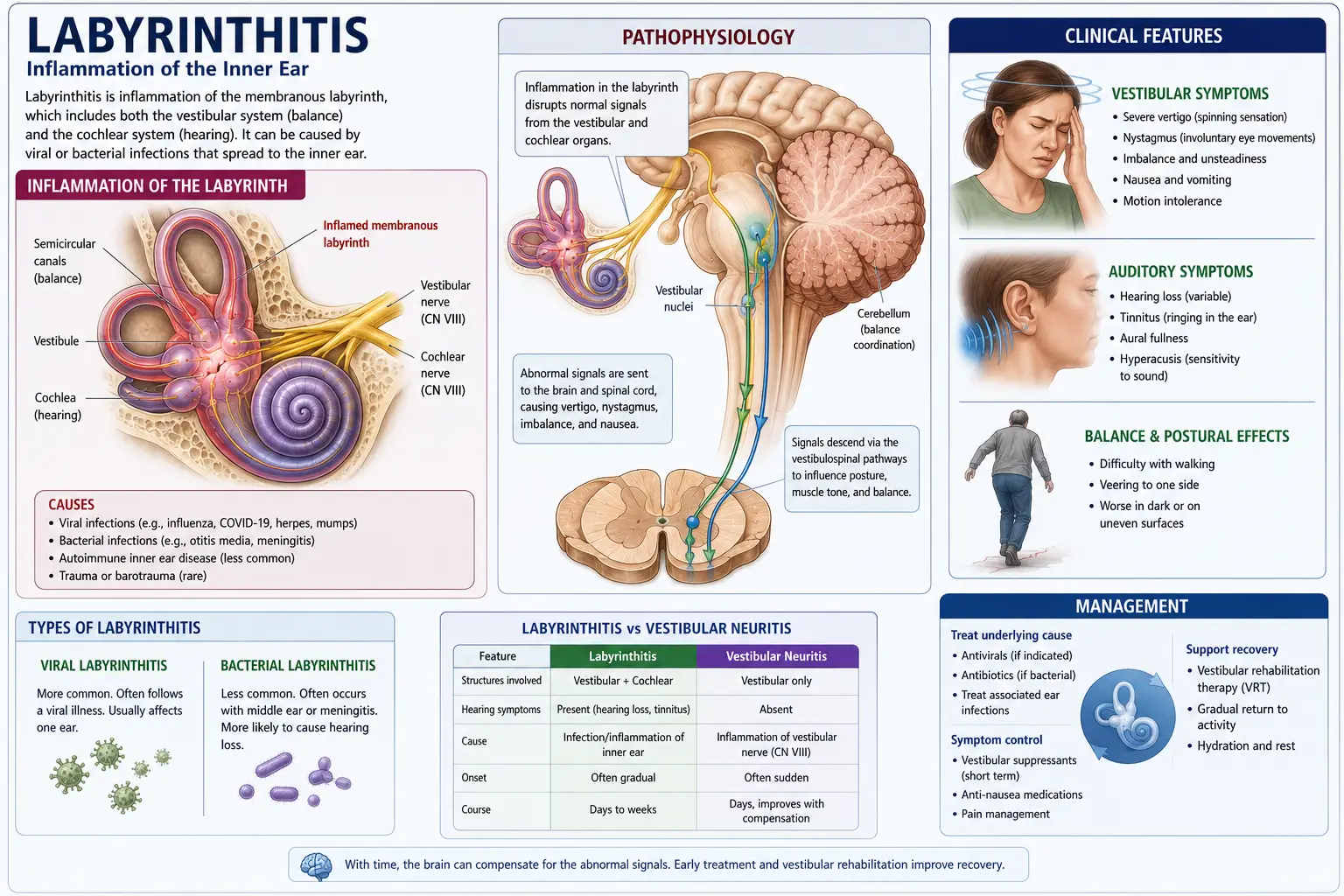
Labyrinthitis is an inflammatory condition of the inner ear that affects both balance and hearing. To understand it, you have to know a little about the anatomy of the inner ear.
Deep inside your ear sits a delicate structure called the labyrinth — a system of fluid-filled tubes and chambers that does two jobs at once. The first part, the cochlea, is responsible for hearing. The second part, the vestibular system, is responsible for balance and spatial orientation. When the labyrinth becomes inflamed, both systems get disrupted simultaneously — which is why labyrinthitis produces such a unique combination of symptoms.
This is the key feature that separates labyrinthitis from its close cousin, vestibular neuritis. Vestibular neuritis affects only the balance nerve, so patients experience vertigo without hearing changes. Labyrinthitis affects the entire labyrinth, so patients experience vertigo AND hearing symptoms — hearing loss, tinnitus, ear pressure, or muffled hearing in the affected ear.
Common symptoms of acute labyrinthitis include:
- Sudden, severe vertigo (room-spinning sensation)
- Hearing loss in one ear
- Ringing in the ears (tinnitus)
- A feeling of ear fullness or pressure
- Intense nausea and vomiting
- Loss of balance — patients often fall toward the affected side
- Involuntary eye movements (nystagmus)
- Difficulty walking, standing, or even sitting up
- Extreme sensitivity to head movement
- Profuse sweating and a sense of impending doom
Most cases of labyrinthitis are caused by viral infections — often following a cold, flu, upper respiratory infection, or other viral illness. Less commonly, bacterial labyrinthitis can develop as a complication of middle ear infections or meningitis. In rare cases, autoimmune conditions, allergies, head trauma, or certain medications can also trigger labyrinthitis.
According to current literature, the acute phase typically lasts a few days to a week, with most patients seeing significant improvement within two to three months. However, a substantial number of patients experience lingering symptoms — vertigo, imbalance, tinnitus, or partial hearing loss — that persist long beyond the original infection. Older adults are particularly likely to have prolonged recovery, and in rare cases, permanent hearing loss or balance issues can occur.
How Labyrinthitis Affects Your Nervous System and Blood Flow
To understand why so many patients struggle with incomplete recovery from labyrinthitis, you need to look at how deeply this condition affects the nervous system — and why the upper cervical spine becomes such a critical part of healing.
Your balance system relies on three primary sensory inputs:
- Vestibular input from the inner ear and labyrinth
- Visual input from your eyes
- Proprioceptive input from your joints and muscles, especially in the neck
When labyrinthitis damages the labyrinth, vestibular input becomes unreliable — sometimes permanently. The brain doesn’t get rid of that unreliable input; it tries to recalibrate by leaning more heavily on the other two systems. This recalibration process is called vestibular compensation, and it happens almost entirely in the brainstem and cerebellum — the same areas that sit directly adjacent to your upper cervical spine.
That’s why dysfunction in the upper neck matters so much after labyrinthitis. Even if the upper cervical spine wasn’t the original cause, it dramatically affects how well your brain can compensate. If your neck is sending faulty proprioceptive data on top of the damaged vestibular input, your brain now has two unreliable inputs to work with. Compensation stalls. Symptoms linger.
There’s a vascular component too. The vertebral arteries — major blood vessels that supply the brainstem, cerebellum, and inner ear — pass directly through the bones of the upper cervical spine. When the upper cervical spine is misaligned or surrounded by chronic muscle tension, blood flow through these arteries can be subtly compromised. Reduced flow to the very areas your brain needs for inner ear recovery means slower healing, more persistent tinnitus, and prolonged dizziness.
And then there’s the vagus nerve, which exits the skull right next to the atlas (C1). The vagus regulates autonomic balance — heart rate, digestion, blood pressure, and overall recovery state. Upper cervical dysfunction can irritate the vagus nerve, contributing to the brain fog, fatigue, and lingering nausea that post-labyrinthitis patients describe months after their acute episode.
There’s one more factor specific to labyrinthitis: the Eustachian tube and middle ear pressure regulation. The muscles that control the Eustachian tube are innervated from the upper cervical region. Post-labyrinthitis patients frequently develop secondary Eustachian tube dysfunction, contributing to ongoing ear fullness, pressure, and muffled hearing that doesn’t fully resolve with time alone.
In short: labyrinthitis starts in the inner ear, but its long-term outcome is heavily influenced by what’s happening in the upper neck.
Why the Upper Cervical Spine Matters in Labyrinthitis Recovery
A common question we hear from patients is: “If my labyrinthitis was caused by a virus, why does my neck have anything to do with my recovery?”
The answer comes down to two things: how vestibular compensation works, and what actually happens to your neck during a labyrinthitis episode.
How compensation works: When the labyrinth is damaged, the brain has to rebuild a new sense of balance using the remaining inputs — primarily vision and neck proprioception. The neck proprioceptors involved in this process are concentrated overwhelmingly in the upper cervical spine (C1 through C3). This region has the highest density of mechanoreceptors anywhere in the spine, and the most direct neurological connections to the vestibular nuclei in the brainstem.
If the upper neck is functioning well, the brain has excellent backup data to compensate with. Recovery proceeds smoothly.
If the upper neck is dysfunctional, the brain’s “backup system” is also unreliable. Now the brain has to compensate using a damaged labyrinth AND a poorly-signaling neck. Recovery stalls.
What happens to your neck during labyrinthitis: This is the piece most patients have never had explained to them. During the acute phase, you likely:
- Lay rigidly still for days, afraid to move your head
- Tensed your neck and shoulder muscles for hours on end fighting nausea
- Slept in awkward positions trying to find any relief
- Avoided turning your head for a week or more
- Were unable to fully relax until the worst symptoms passed
Every one of those things creates real, measurable upper cervical dysfunction. The original viral inflammation may resolve in days. The neck dysfunction it caused often persists for months or years.
This is why so many post-labyrinthitis patients say their dizziness “changed” at some point. The spinning fades. The tinnitus settles into the background. But a new pattern emerges — swimming, rocking, ear pressure, balance issues, brain fog — and nobody can figure out why it won’t go away. The answer, in many cases, is that the original labyrinthitis has evolved into a secondary upper cervical problem that nobody has addressed.
Upper Cervical Chiropractic Care for Labyrinthitis: What to Expect
At Lavender Family Chiropractic, we approach post-labyrinthitis recovery in a careful, gentle, and precise way. Our role is not to replace any medical care you received during your acute episode — it’s to support and complete the recovery process that your body has been trying to finish on its own.
Here’s what your journey looks like at our Sarasota office.
Step One: Comprehensive Consultation
Your first visit starts with a real conversation. Dr. Lavender or Dr. Temple will sit down with you and learn the full story — when the labyrinthitis hit, how severe it was, whether you had hearing loss or tinnitus, what treatments you’ve tried, what symptoms remain, and how this has impacted your life. Labyrinthitis recovery is rarely linear, and details matter.
Step Two: 3D CBCT Imaging and Neurological Scanning
Next, we use 3D CBCT X-ray technology to take precise, three-dimensional images of your upper cervical spine. This advanced imaging shows us — down to the millimeter — exactly how your atlas (C1) and axis (C2) are positioned, allowing us to calculate the precise corrective vector your spine needs.
We pair this with paraspinal infrared thermography, which measures nervous system function along your spine. Thermography is particularly useful for post-labyrinthitis patients because it shows us patterns of nervous system stress and inflammation that often correspond to the lingering symptoms you’re experiencing.
Step Three: A Gentle, Specific Correction
When you receive your upper cervical correction, you’ll likely be surprised at how gentle it is. There is no twisting, popping, or cracking. We use the Advanced HIO Knee Chest Upper Cervical Technique (AHKC), which delivers a calculated, feather-light adjustment based on your specific imaging.
This precision and gentleness matter enormously for labyrinthitis patients. After what you’ve been through, anything aggressive or forceful around your head or neck is the last thing you want. Our technique is designed to work with your nervous system, not against it — appropriate even for the most dizziness-sensitive patients.
Step Four: Monitoring and Stabilizing Your Recovery
The goal of upper cervical care isn’t to adjust you forever. The goal is to help your spine hold its corrected position, so your nervous system can finally finish the compensation it started. We track your progress visit by visit — your symptoms, your alignment, your nervous system function — and adjust your care plan as you stabilize.
Most post-labyrinthitis patients begin noticing changes within the first few weeks: clearer thinking, less rocking sensation, reduced ear fullness and pressure, better tolerance to head movement, improved sleep, and sometimes meaningful changes in tinnitus. Recovery is gradual but real, and the trajectory is almost always positive once the upper cervical piece is addressed.
Has your labyrinthitis recovery stalled? Call us at (941) 243-3729 or book a complimentary consultation online. We’ll help you figure out whether upper cervical care is the missing piece.
What the Research Says About Labyrinthitis
The medical literature on labyrinthitis has expanded steadily over the past several years. Here are some of the most relevant findings for our patients.
A 2025 update published in StatPearls (NCBI Bookshelf) confirmed that while most cases of labyrinthitis are viral in origin, the long-term outcome varies widely — some patients recover fully, while others experience lasting impairments to hearing or vestibular function. The authors emphasized that expeditious evaluation and accurate diagnosis are essential to optimizing outcomes, particularly because labyrinthitis can mimic more serious conditions like stroke.
According to the Cleveland Clinic and ENT Health professional resources, recovery from labyrinthitis typically takes up to six weeks for most patients, with severe symptoms usually resolving within a week. However, older adults are significantly more likely to experience prolonged dizziness, and rare cases involve permanent hearing loss or balance dysfunction.
Research from Johns Hopkins Medicine notes that labyrinthitis can occasionally be associated with herpes virus (herpes zoster or shingles), Lyme disease, or other organisms — and that the conditions are likely to resolve on their own, though medications may be prescribed depending on the underlying cause.
Importantly, current literature emphasizes that long-term use of vestibular suppressants (like meclizine or benzodiazepines) actually impairs recovery because they suppress the very signals the brain needs to compensate. Most vestibular specialists now recommend tapering off these medications as soon as the acute phase passes.
The takeaway from current research is consistent: labyrinthitis is treatable, recovery is possible, and the quality of long-term outcome depends heavily on how well the nervous system can compensate after the initial damage.Upper cervical chiropractic care directly supports that compensation process — which is why it has become such an important piece of post-labyrinthitis recovery for so many patients.
Lifestyle Habits That Support Recovery from Labyrinthitis
Beyond upper cervical care, daily habits play a major role in how completely your nervous system can recover. Here’s what we recommend most often to our post-labyrinthitis patients.
Move regularly — but gradually. The instinct after labyrinthitis is to hold still and avoid anything that triggers symptoms. The opposite is what your brain needs. Gradual, daily exposure to head movement and walking is essential for vestibular compensation. Avoidance prolongs the dizziness.
Sleep well. Quality sleep is when the brain does the bulk of its compensation work. Aim for 7–9 hours per night and use a supportive pillow that maintains proper neck alignment. Stomach sleeping is particularly hard on the upper cervical spine and should be avoided.
Stay hydrated. Inner ear fluid balance is directly affected by systemic hydration, and Florida’s heat and humidity make dehydration a daily risk. Aim for at least half your body weight in ounces of water per day. This single habit can meaningfully reduce both dizziness and tinnitus.
Address screen and posture habits. Forward head posture during screen use puts enormous strain on the upper cervical spine — exactly the area your brain is leaning on for balance information. Eye-level monitors, periodic posture resets, and limiting prolonged phone scrolling all help.
Manage stress. Stress drives sympathetic nervous system overactivity, increases muscle tension in the neck and shoulders, and amplifies dizziness and tinnitus. Breathing exercises, walking outside, and time away from screens are simple but powerful tools.
Wash your hands and protect against repeat infections. Since most cases of labyrinthitis follow a viral illness, basic infection prevention reduces your risk of a repeat episode. Cold and flu season warrants extra caution.
Address related conditions. Post-labyrinthitis patients often develop secondary issues — Eustachian tube dysfunction, neck pain, and tension-pattern headaches. For more on how the cervical spine drives dizziness even after the inner ear has healed, our blog on the connection between neck pain and vertigo is a useful companion read.
Serving Sarasota and Surrounding Areas
Lavender Family Chiropractic is located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — right at the corner of University and Whitfield. We are easy to reach from anywhere in the greater Sarasota region.
We proudly serve patients dealing with labyrinthitis and other forms of chronic dizziness from across the area, including:
- Sarasota, FL
- Bradenton, FL
- Lakewood Ranch, FL
- Venice, FL
- Osprey, FL
- Parrish, FL
- Ellenton, FL
- Siesta Key, FL
- Longboat Key, FL
- St. Pete, FL
- Tampa, FL
To learn more about the full region we serve, visit our areas we service page. Wherever you’re driving from, we’re set up to help.
Top 15 FAQs About Labyrinthitis
What exactly is labyrinthitis?
Labyrinthitis is inflammation of the inner ear’s labyrinth — the structure responsible for both balance and hearing. It causes a combination of severe vertigo, hearing loss, tinnitus, ear fullness, nausea, and balance problems. Most cases are caused by viral infections, often following a cold or flu.
What’s the difference between labyrinthitis and vestibular neuritis?
Vestibular neuritis affects only the balance nerve, so patients have vertigo without hearing changes. Labyrinthitis affects the entire labyrinth, so patients have vertigo PLUS hearing symptoms — hearing loss, tinnitus, ear fullness, or muffled hearing. They are closely related conditions and often respond to similar care approaches.
How long does labyrinthitis last?
The acute phase typically lasts a few days to a week. Most patients see significant improvement within two to three months. However, a substantial percentage of patients experience lingering symptoms — dizziness, tinnitus, partial hearing loss — that can persist for months or even years without targeted care.
Why am I still dizzy months after my labyrinthitis episode?
This usually means your brain’s vestibular compensation is incomplete. Common contributors include unaddressed upper cervical dysfunction, secondary Eustachian tube dysfunction, prolonged stress, poor sleep, and dehydration. Addressing the upper neck often makes the single biggest difference for chronic post-labyrinthitis patients.
Can labyrinthitis cause permanent hearing loss?
In rare cases, yes — particularly with bacterial labyrinthitis or severe viral episodes. Most patients recover their hearing fully, but a minority experience some degree of permanent hearing loss in the affected ear. Cochlear implants or bone-conduction hearing aids may be options in severe cases.
Why do I have tinnitus that won’t go away after labyrinthitis?
Tinnitus after labyrinthitis can persist long after the initial infection clears, especially if there’s secondary Eustachian tube dysfunction or upper cervical involvement. Many post-labyrinthitis patients see meaningful tinnitus reduction with upper cervical correction, though full resolution depends on individual factors.
Is upper cervical care safe after labyrinthitis?
Yes. Upper cervical chiropractic is one of the gentlest forms of chiropractic care available. There is no twisting, popping, or cracking. We use precise, imaging-guided corrections that are appropriate even for the most dizziness-sensitive patients.
Will I need vestibular rehabilitation too?
Some patients benefit from combining upper cervical care with vestibular rehabilitation, particularly if compensation has stalled. Others recover well with upper cervical care alone. We’ll help you decide what combination makes sense for your case.
How soon after my labyrinthitis episode should I seek upper cervical care?
The sooner the better. Research shows that the longer dizziness patterns persist, the more entrenched they become in the brain. That said, it’s never too late — patients who have been dealing with post-labyrinthitis symptoms for years can still see meaningful improvement.
Can labyrinthitis come back?
Recurrence is possible but uncommon. More frequently, what feels like a “recurrence” is actually a flare-up of incomplete compensation triggered by stress, illness, or another upper cervical issue. Restoring proper upper cervical function helps stabilize against these flares.
Are medications helpful for chronic dizziness after labyrinthitis?
Medications like meclizine can reduce acute symptoms but tend to delay recovery if used long-term, because they suppress the very signals the brain needs to compensate. Most vestibular specialists recommend tapering off vestibular suppressants as soon as the acute phase passes.
Why does my dizziness get worse with screen use or busy environments?
After labyrinthitis, your brain often becomes more dependent on visual input for balance. Busy visual environments — screens, scrolling, supermarkets, crowds — overwhelm that compensation and produce dizziness. Restoring neck proprioception through upper cervical care reduces visual dependency.
Can stress make my post-labyrinthitis symptoms worse?
Yes. Stress increases sympathetic nervous system activity, tightens the muscles around the upper neck, and amplifies dizziness and tinnitus. Stress management is a meaningful part of post-labyrinthitis recovery.
Can children get labyrinthitis?
Yes, though it’s more common in adults. Children with labyrinthitis usually recover quickly with proper care, especially if the underlying viral or bacterial infection is identified and treated early. Chronic post-labyrinthitis symptoms are less common in children than in older adults.
How do I know if Lavender Family Chiropractic is right for me?
If you’ve had labyrinthitis and are still experiencing lingering dizziness, tinnitus, ear fullness, brain fog, or fatigue months after the original episode — or if traditional care hasn’t fully resolved your symptoms — you’re an excellent candidate for an evaluation. Call (941) 243-3729 to schedule a complimentary consultation.
You Don’t Have to Stay Stuck in Post-Labyrinthitis Recovery
Labyrinthitis is one of the most frightening conditions to live through, and one of the most frustrating to recover from. The acute episode is dramatic, but the long tail — the lingering dizziness, the tinnitus that won’t quit, the ear fullness that comes and goes, the brain fog you can’t shake — is often what wears patients down most.
At Lavender Family Chiropractic, Dr. Rusty Lavender and Dr. Jacob Temple have helped many patients across Sarasota close the gap between “almost recovered” and “truly back to themselves.” If you’re tired of being told to just give it more time, we’d be glad to help you understand what’s still standing in the way of complete recovery.
📞 Call us today at (941) 243-3729 📅 Or book your complimentary consultation online
You don’t have to live with the leftover symptoms anymore.
Related Articles
- Vertigo Sarasota: Dr. Jake’s #1 Way to Resolve Dizziness
- Why Vertigo Happens: Our #1 Guide to Resolving the Spinning
- Neck Pain and Vertigo: 1 Quick Way to Resolve Symptoms
By Dr. Rusty Lavender and Dr. Jacob Temple — Lavender Family Chiropractic, Sarasota, FL