Understanding Vertigo and the Synergistic Role of Vitamin B12 and Upper Cervical Chiropractic Care
Vertigo and chronic dizziness are more than just fleeting annoyances—they can fundamentally alter the course of daily life, impeding work performance, social engagement, and emotional well-being. While conventional treatments often focus on symptom suppression (antihistamines, vestibular rehab maneuvers, diuretics for Ménière’s), lasting relief frequently demands a holistic approach. In this comprehensive 3,500-word guide, we’ll delve deep into:
- Vertigo: Scope and Subtypes
- Vitamin B12 Essentials
- Oral B12 Supplementation for Vestibular Health
- Upper Cervical Spine Anatomy and Its Impact on Balance
- Lavender Family Chiropractic’s Precision Upper Cervical Technique
- Designing an Integrated B12 + Upper Cervical Protocol
- Lifestyle, Diet, and Home Strategies to Reinforce Care
- Emerging Research and Future Directions
- Patient Success Narratives
- Top 15 FAQs on B12 & Upper Cervical Chiropractic for Vertigo
By the end, you’ll have a clear, actionable roadmap to address vertigo at its root—nutritionally, structurally, and holistically—under the expert care of Dr. Rusty Lavender, Dr. Jacob Temple and Dr. Will Guzinski at Lavender Family Chiropractic in Sarasota, Florida.
1. Vertigo: Scope and Subtypes
1.1 The Hidden Epidemic of Dizziness
Vertigo and dizziness affect an estimated 30% of adults at some point in life, with prevalence rising sharply after age 60. Yet despite its ubiquity, vertigo often goes misunderstood or undertreated. Far from being a simple “lightheaded” feeling, vertigo is the false perception of movement—typically a spinning or tilting sensation—often accompanied by nausea, sweating, and difficulty focusing.
- Impact on Quality of Life: Chronic dizziness leads to falls (the leading cause of injury-related deaths in seniors), driving avoidance, anxiety, and depression. Individuals with recurrent vertigo report social withdrawal, fearing sudden episodes in public.
1.2 Major Vertigo Subtypes and Underlying Mechanisms
- Benign Paroxysmal Positional Vertigo (BPPV)
- Mechanism: Otoconia (calcium carbonate crystals) dislodge from the utricle into semicircular canals, causing transient vertigo with head movements.
- Symptoms: Seconds-long spinning when rolling over in bed, looking up, or tilting the head.
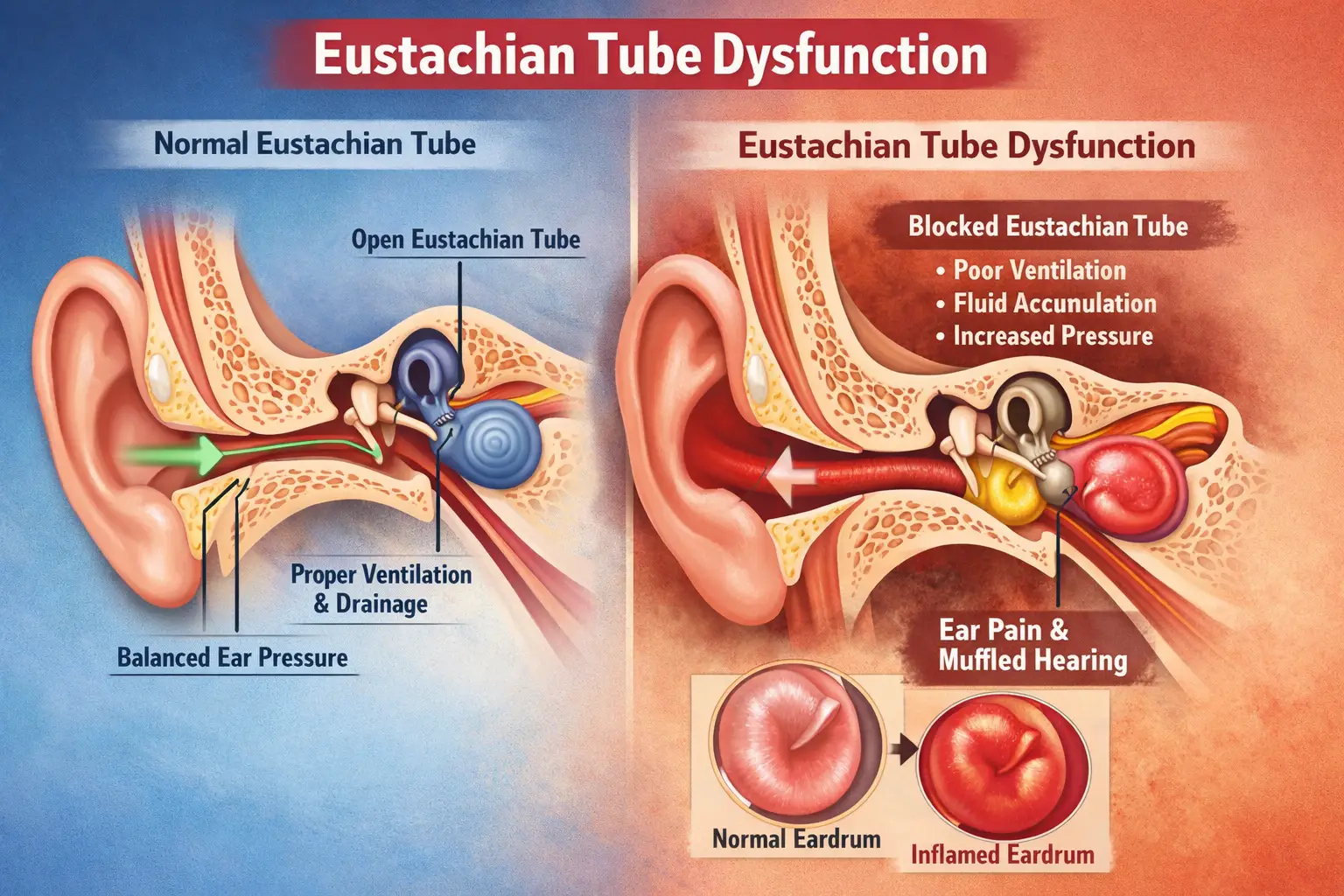
- Ménière’s Disease
- Mechanism: Endolymphatic hydrops—excess fluid pressure distorts the membranous labyrinth.
- Symptoms: Spontaneous episodes of vertigo lasting 20 minutes to 24 hours; tinnitus, hearing loss, and aural fullness.
- Mal de Débarquement Syndrome (MdDS)
- Mechanism: After prolonged passive motion (boat, plane), central adaptation fails to readjust to stable ground, producing persistent rocking.
- Symptoms: Constant swaying or bobbing sensation weeks or months after travel.
- Vestibular Migraine
- Mechanism: Overlap of migraine neurochemistry with vestibular pathways leads to episodic dizziness, sometimes without headache- Vestibular Migraine.
- Symptoms: Vertigo coinciding with photophobia, phonophobia, and/or typical migraine aura.
- Generalized Dizziness (Non-specific)
- Mechanism: Multifactorial—vascular insufficiency, neurological disorders, proprioceptive imbalance, or medication side effects.
- Symptoms: Persistent unsteadiness or lightheadedness without clear rotational component.
Understanding which subtype you face shapes treatment selection—and often reveals why isolated remedies fail to deliver lasting change.
2. Vitamin B12 Essentials
2.1 Biochemical Roles and Neurological Importance
Vitamin B12 (cobalamin) is indispensable for two biochemical pathways:
- Methionine Synthase: Converts homocysteine to methionine, fueling methylation reactions vital for DNA synthesis, neurotransmitter production (serotonin, dopamine), and myelin maintenance.
- Methylmalonyl-CoA Mutase: Converts methylmalonyl-CoA into succinyl-CoA in the Krebs cycle, supporting neuronal energy metabolism.
Within the vestibular apparatus, both inner-ear hair cells and central brainstem nuclei demand rapid, precise nerve conduction. Myelin integrity and mitochondrial energy production—both B12-dependent—are thus paramount.
2.2 Recognizing B12 Deficiency
Suboptimal B12 may present subtly:
- Neurological: Paresthesias in hands or feet, gait instability, cognitive “fogginess.”
- Psychiatric: Mood swings, irritability, depression.
- Hematologic: Macrocytic anemia (fatigue, pallor).
- Vestibular: Exacerbation of dizziness, prolonged compensation from vestibular insults.
Because up to 20% of adults over 60—and many younger patients on metformin, PPIs, or plant-based diets—harbor low-normal B12, routine screening in dizzy patients often uncovers correctable deficits.
2.3 Dietary Sources and Absorption Challenges
- Natural Sources: Animal products—meat, fish, dairy, eggs.
- Fortified Foods: Plant milks, cereals.
- Supplement Forms: Cyanocobalamin vs. methylcobalamin; the latter is bioactive, bypassing conversion needs.
Absorption hinges on intrinsic factor (produced by stomach parietal cells) and healthy ileal mucosa; anything from atrophic gastritis to small-intestinal bacterial overgrowth can impair uptake, making high-dose oral supplementation necessary.
Vitamin B12 (cobalamin) is one of the most fascinating and vital nutrients your body needs to function optimally. As a water-soluble vitamin, it travels through your bloodstream helping to build red blood cells, maintain nervous system health, and support energy production. In this overview, we’ll explore:
- What vitamin B12 is and how it works
- Dietary sources and absorption pathways
- Signs and risks of deficiency
- Recommended intake and supplementation strategies
- Special populations with increased needs
- Interactions, precautions, and practical tips
By the end, you’ll have a clear, 360° understanding of why B12 is so essential—and how to make sure you’re getting enough.
What Vitamin B12 Is and How It Works
Vitamin B12 is one of eight B-complex vitamins, but it stands out because of its unique structure: a corrin ring centered on a cobalt atom. This gives it the name “cobalamin.” Unlike most other vitamins, B12 acts as a coenzyme in two critical biochemical reactions:
- Conversion of homocysteine to methionine
- Enzyme: Methionine synthase
- Why it matters: This reaction supports methylation—a process that affects DNA synthesis, neurotransmitter production, and detoxification pathways.
- Conversion of methylmalonyl-CoA to succinyl-CoA
- Enzyme: Methylmalonyl-CoA mutase
- Why it matters: This reaction feeds into the Krebs cycle, fueling cellular energy production, especially in nerve cells and blood-forming tissues.
Because of these roles, B12 is fundamental to:
- Red blood cell formation: Preventing macrocytic anemia and ensuring efficient oxygen transport
- Myelin synthesis: Maintaining the protective sheath around nerve fibers for rapid signal transmission
- DNA replication and repair: Supporting healthy cell division across all tissues, particularly the gastrointestinal lining and bone marrow
Without adequate B12, you may experience fatigue, neurological symptoms, and hematologic problems that progressively worsen over time.
Dietary Sources and Absorption Pathways
2.1 Natural Food Sources
Vitamin B12 is produced by certain bacteria and archaea, which accumulate in animal tissues. As a result, the richest natural sources are:
- Shellfish: Clams, oysters, and mussels
- Fish: Salmon, trout, tuna, and sardines
- Meat: Beef liver, steak, and poultry
- Dairy: Milk, yogurt, and cheese
- Eggs: Particularly the yolk
Most people meeting a varied omnivorous diet will achieve adequate intake, but certain diets and digestive issues can impair absorption.
2.2 The Complex Absorption Process
Absorbing B12 is a multi-step process that involves:
- Release from protein: In the stomach, gastric acid and pepsin free B12 from dietary proteins.
- Binding to intrinsic factor (IF): Parietal cells in the stomach lining secrete intrinsic factor, a glycoprotein that binds B12 in the small intestine.
- Receptor-mediated uptake: In the distal ileum, IF-B12 complexes bind to cubam receptors on enterocytes, allowing active transport into circulation.
Any disruption—Low stomach acid (hypochlorhydria), parietal cell loss (atrophic gastritis), IF deficiency (pernicious anemia), or ileal disease (Crohn’s)—can compromise absorption, leading to deficiency risk.
Signs and Risks of B12 Deficiency
Vitamin B12 deficiency can develop slowly, with early signs often mistaken for general fatigue or stress. Common symptoms include:
- Hematologic:
- Macrocytic (megaloblastic) anemia
- Pallor and shortness of breath on exertion
- Neurological:
- Paresthesias (tingling, “pins and needles”) in hands and feet
- Gait disturbances and balance problems
- Cognitive changes: memory lapses, “brain fog,” mood swings
- Gastrointestinal:
- Glossitis (inflamed tongue)
- Appetite loss and weight changes
- Nausea or diarrhea
Because the nervous system can be permanently damaged if deficiency persists, early detection and correction are paramount.
Recommended Intake and Supplementation Strategies
4.1 Daily Requirements
The U.S. National Institutes of Health (NIH) recommends the following daily amounts:
- Infants (0–6 months): 0.4 mcg
- Children (1–8 years): 0.9–1.2 mcg
- Adolescents (9–13 years): 1.8 mcg
- Teens (14–18 years): 2.4 mcg
- Adults: 2.4 mcg
- Pregnant: 2.6 mcg
- Lactating: 2.8 mcg
4.2 Oral Supplementation
For individuals at risk of deficiency—or those aiming for optimal neurological support—higher oral doses are often used:
- Maintenance: 1,000 mcg daily of methylcobalamin
- Correction: 2,000–5,000 mcg daily until blood markers normalize
- Form: Methylcobalamin preferred for direct nervous system uptake, though cyanocobalamin is also effective.
High-dose oral B12 utilizes passive diffusion (about 1–2% of dose) even without intrinsic factor, making it effective for many malabsorption conditions.
4.3 Injectable B12
Intramuscular or subcutaneous injections bypass the digestive tract entirely. Protocols vary:
- Initial loading: 1,000 mcg every other day for 1–2 weeks
- Taper: Weekly injections for 4–6 weeks
- Maintenance: Monthly injections
Injections are critical for pernicious anemia or severe malabsorptive states.
Special Populations with Increased Needs
Certain groups face greater risk for low B12 or have higher requirements:
- Older adults: Reduced gastric acid impairs release from food proteins.
- Vegetarians and vegans: Plant foods lack active B12; fortified foods or supplements are essential.
- Gastrointestinal disorders: Celiac, Crohn’s, and gastric surgeries (e.g., bariatric) disrupt absorption.
- Metformin users: Chronic metformin therapy can lower B12 levels by up to 30%.
- Proton pump inhibitor (PPI) users: Long-term acid suppression decreases protein-bound B12 release.
- Pregnancy and lactation: Fetal development and breastmilk B12 content require higher maternal intake.
Identifying these populations early allows proactive supplementation and monitoring.
Interactions, Precautions, and Practical Tips
- Medications: Metformin, PPIs, H2 blockers, and certain antibiotics (chloramphenicol) can interfere with B12 status.
- Folate mask: High folic acid intake can correct anemia but not neurological damage; always assess B12 directly.
- Testing: Beyond serum B12, measure methylmalonic acid (MMA) and homocysteine for functional deficiency.
Practical tips:
- Take B12 supplement with breakfast for optimal absorption.
- Choose sublingual or lozenge forms if you have mild malabsorption issues.
- Store B12 tablets in a cool, dry place to preserve potency.
- Pair B12 with a B-complex for synergistic support of homocysteine metabolism.
Putting It All Together
Vitamin B12 is a small molecule with a monumental impact. From energizing your cells to protecting your nervous system, its presence—or absence—can make the difference between vibrant health and chronic fatigue, cognitive decline, or neurological impairment. By:
- Eating B12-rich foods (shellfish, lean meats, dairy)
- Screening regularly if you’re in an at-risk group
- Supplementing strategically (1,000–5,000 mcg methylcobalamin daily)
- Monitoring functional biomarkers (MMA, homocysteine)
…you can ensure that your body—and brain—have the coenzyme power they need to thrive.
If you suspect you may be low in B12 or simply want to optimize your neurological and hematologic health, speak with your healthcare provider about testing and a personalized supplementation plan. With the right approach, you’ll lay a foundation for energy, mental clarity, and resilience that lasts a lifetime.
3. Oral B12 Supplementation for Vestibular Health
3.1 Why Methylcobalamin?
Methylcobalamin offers:
- Direct CNS Uptake: Crosses the blood-brain barrier more readily.
- Enhanced Nerve Repair: Shown in studies to support remyelination faster than cyanocobalamin.
- Patient Convenience: Once-daily dosing, no injections.
3.2 Mechanisms Supporting Vestibular Recovery
- Myelin Repair & Conduction Velocity: Enhances speed of vestibular nerve signals, reducing lag and false motion perceptions.
- Homocysteine Reduction: Lowers homocysteine, protecting microvasculature of the inner ear from endothelial damage and ischemia.
- Neurotransmitter Balance: Supports GABA and glutamate balance, critical for central vestibular inhibition and synchrony.
3.3 Dosing Protocols
- Mild Insufficiency: 1,000 mcg daily.
- Moderate/Severe Deficiency: 2,000–5,000 mcg daily until levels normalize.
- Maintenance: 1,000–2,000 mcg daily long-term.
Best taken in the morning with food to maximize absorption and avoid sleep disturbances from B12’s energizing effect.
3.4 Evidence Base
- Neuropathy Trials: RCTs in diabetic neuropathy show 1,500–3,000 mcg methylcobalamin daily improves nerve conduction velocities by up to 20% over 12 weeks.
- Vestibular Cohorts: Small studies report 30–50% reduction in Dizziness Handicap Inventory (DHI) scores after 3 months of B12 in patients with chronic dizziness and low-normal levels.
- Case Reports in MdDS: Anecdotal remission of rocking sensations within 6–8 weeks when B12 added to vestibular exercises.
Although large multicenter trials in BPPV/Ménière’s are lacking, the low risk profile of B12 and its foundational neurological roles make it a compelling adjunct.
4. Upper Cervical Spine Anatomy and Its Impact on Balance
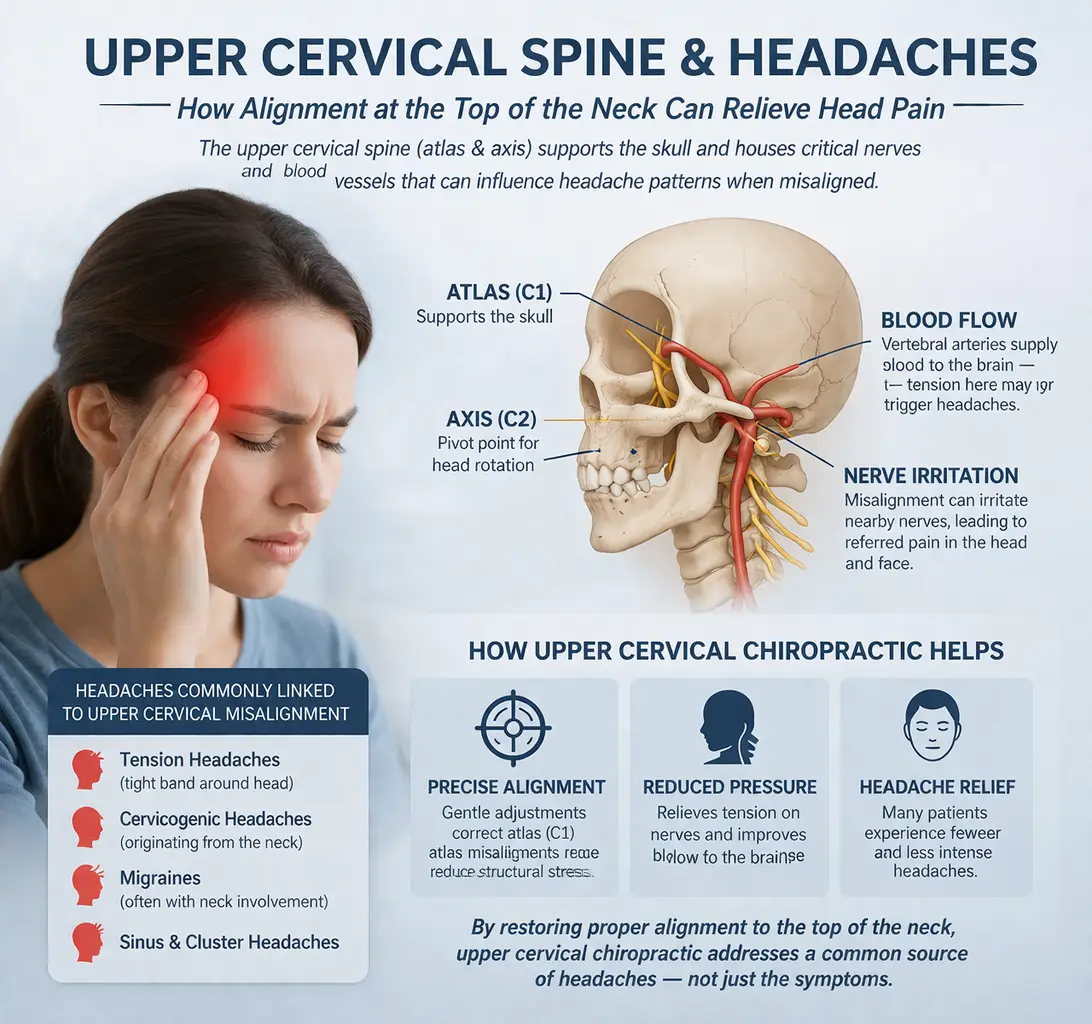
4.1 The Critical C1–C2 Complex
- Atlas (C1): Supports the skull, allowing nodding (“yes” motion).
- Axis (C2): Provides pivot for rotation (“no” motion).
- Biomechanical Significance: These top two vertebrae house vertebral arteries, jugular venous outlets, and the brainstem/upper spinal cord junction. Even tiny misalignments (<1 mm) can distort these structures.
4.2 How Misalignment Provokes Vertigo
- Brainstem Irritation: Atlas rotation or lateral tilt creates tension on the meninges and brainstem, misfiring vestibular nuclei.
- Vascular Compression: Twisting of C1/C2 impedes vertebral artery flow (up to 20% reduction), depriving the inner ear and cerebellum of oxygen-rich blood.
- Proprioceptive Mismatch: Neck mechanoreceptors contribute ~50% of cranial positional input; distorted signals breed central confusion and dizziness.
- CSF Flow Disruption: Misalignment can impede cerebrospinal fluid pulsations at the foramen magnum, altering inner-ear endolymph homeostasis and pressure regulation.
4.3 Beyond “Cracking”—Why Precision Matters
Generic cervical manipulations rarely isolate C1/C2 misalignments. High-velocity “cracks” can reflexively tense neck musculature, perpetuating maladaptive patterns. A data-driven upper cervical approach pinpoints the exact vector and magnitude needed for true realignment—no forceful twisting required.
5. Lavender Family Chiropractic’s Precision Upper Cervical Technique
At Lavender Family Chiropractic, Dr. Jacob Temple and Dr. Will Guzinski combine cutting-edge diagnostics with gentle, evidence-based adjustments tailored to each patient’s anatomy.
5.1 Comprehensive, Data-Driven Assessment
- Detailed Intake & Symptom Mapping: Exploration of vertigo triggers, dietary/nutritional history, sleep patterns, stressors, and prior treatments.
- Postural & Gait Analysis: Visual assessment of head tilt, shoulder height, pelvis alignment, and walking symmetry.
- Functional Nervous System Scan: Computerized thermography and galvanic skin response to detect autonomic imbalances tied to cervical dysfunction.
- 3D CBCT Imaging: Cone Beam CT delivers sub-millimeter accuracy in visualizing atlas and axis positioning relative to the skull base—far superior to traditional two-dimensional X-rays.
5.2 Vector-Calculated, Gentle Adjustments
- Pre-Adjustment Planning: Using CBCT data, the precise angle (e.g., 12° posterior, 8° lateral) and force magnitude (<5 lbs) are computed.
- Non-Invasive Contact: A specialized instrument delivers a brief, low-force thrust at the exact vector—no popping, twisting, or discomfort.
- Immediate Feedback: Post-adjustment scans and re-evaluation confirm realignment, often detectable in under a minute.
5.3 Phased Care Model
- Initial Stabilization (Weeks 1–2): 3–4 visits spaced 3–4 days apart to “train” ligaments and musculature to hold the new alignment.
- Re-Evaluation (Week 4): Repeat CBCT to verify retention; adjust vector or visit frequency if needed.
- Maintenance & Prevention (Month 2 onward): Taper to monthly or bi-monthly check-ins, depending on symptom recurrence and lifestyle stressors.
5.4 Safety and Comfort
Because force and displacement are meticulously calculated, patients report the adjustment as “barely noticeable” yet “immediately soothing.” There are virtually no contraindications aside from acute cervical fractures or severe osteoporosis—which are screened out by thorough history and imaging.
6. Designing an Integrated B12 + Upper Cervical Protocol
A truly holistic plan addresses both biochemical resilience and structural integrity.
6.1 Sample 6-Month Protocol
| Phase | Actions |
|---|---|
| Baseline | – Comprehensive labs: B12, MMA, homocysteine, folate– 3D CBCT & nervous system scan |
| Weeks 1–2 | – Begin methylcobalamin 2,000 mcg daily– 3 upper cervical adjustments (every 3–4 days) |
| Week 4 | – Repeat CBCT alignment check– Assess subjective symptom diary & DHI score |
| Months 2–3 | – Continue B12; adjust dose based on follow-up labs– Vestibular rehab exercises 2×/day |
| Month 4 | – Re-evaluate B12 levels; taper to maintenance dose if normalized– Adjust chiropractic frequency |
| Months 5–6+ | – Monthly check-ins (adjustments + labs as needed)– Ongoing vestibular exercises at home |
6.2 Complementary Home Strategies
- Vestibular Exercises:
- Brandt-Daroff: Habituation for positional dizziness.
- Epley Maneuver: Canalith repositioning for BPPV.
- Gaze Stabilization: Focused head movements to enhance central compensation.
- Ergonomic Sleep:
- cervical support pillows to maintain alignment overnight.
- avoid stomach sleeping which hyperextends the neck.
- Hydration & Diet:
- sodium moderation for Ménière’s (<1,500 mg/day).
- adequate water intake to support CSF and endolymph dynamics.
- magnesium-rich foods (dark leafy greens, nuts) for inner-ear vascular support.
- Stress Management:
- mindfulness meditation to reduce limbic system hyperarousal—common in MdDS and vestibular migraine.
- breathing exercises (4-7-8 technique) to calm sympathetic activation and reduce central sensitization.
7. Lifestyle, Diet, and Home Strategies to Reinforce Care
7.1 Nutritional Optimization Beyond B12
- Vitamin D: Supports vestibular hair-cell survival; deficiency linked to BPPV recurrence.
- Omega-3 Fatty Acids: Anti-inflammatory action protects inner-ear microcirculation.
- Antioxidants: Vitamins C and E scavenge free radicals involved in inner-ear cell damage.
7.2 Postural and Ergonomic Adjustments
- Workstation Setup: Monitor at eye level, feet flat on floor, neutral spine.
- Frequent Breaks: Every 20 minutes, stand, neck circles, gentle stretches to release tension.
- Driving Posture: Seatback slight recline, headrest aligned with the atlas, hands at 3 & 9 o’clock.
7.3 Sleep Hygiene
- Consistent bedtime/wake time to regulate circadian rhythms—important for vestibular compensation.
- Limit screens 1 hour before bed; blue-light suppression of melatonin can exacerbate dizziness.
8. Emerging Research and Future Directions
8.1 B12 & Neuroplasticity
Ongoing studies are examining B12’s role in promoting synaptic plasticity within vestibular pathways—potentially enhancing long-term adaptation after injury. Preliminary animal work suggests methylcobalamin upregulates brain-derived neurotrophic factor (BDNF), a key mediator of central compensation.
8.2 Advanced Imaging of Cervical-Vestibular Coupling
New dynamic MRI techniques are capturing real-time CSF flow and vertebral artery pulsatility at C1/C2—correlating misalignment degrees with functional deficits. Such tools may refine patient selection and adjustment vectors further.
8.3 Biomarker-Driven Personalization
Researchers are exploring panels of vestibular biomarkers (vestibular‐evoked myogenic potentials, cytokine profiles) to predict who will respond best to nutritional vs. structural interventions.
9. Patient Success Narratives
Case Study A—BPPV Reversal
Background: 58-year-old female with monthly BPPV episodes for two years, low-normal B12 (310 pg/mL), failed Epley maneuvers alone.
Intervention: Oral methylcobalamin 2,000 mcg daily + three upper cervical adjustments over 10 days.
Outcome: Complete resolution of positional vertigo within three weeks; B12 rose to 620 pg/mL; no recurrence at six-month follow-up.
Case Study B—MdDS Recovery
Background: 42-year-old male with constant rocking sensations three months post-cruise; vestibular therapy offered minimal relief.
Intervention: 1,500 mcg B12 daily + precision C1/C2 correction twice weekly for three weeks + mindfulness training.
Outcome: 70% symptom reduction by week 4, returned to baseline by week 8; maintained balance at one‐year check.
10. Top 15 FAQs on Vitamin B12 & Upper Cervical Chiropractic for Vertigo
- Why is B12 crucial for vertigo?
B12 underpins myelin integrity and nerve conduction in vestibular pathways. Deficiency can slow signal transmission, exacerbating dizziness and delaying central compensation. - Can oral B12 eliminate my vertigo?
While B12 alone may not “cure” structural causes, it significantly accelerates nerve repair and supports vascular health—often reducing episode frequency and severity when combined with structural care. - How do I test for B12 deficiency?
Comprehensive labs include serum B12, methylmalonic acid (MMA), and homocysteine. MMA elevation is the earliest marker of functional deficiency. - What’s the optimal B12 dose?
Vestibular patients typically start at 2,000 mcg methylcobalamin daily. Maintenance may drop to 1,000 mcg once levels normalize. - How soon will I feel better?
Some notice subtle balance improvements within 2–4 weeks; full vestibular compensation and symptom resolution may take 2–3 months. - Are injections better than oral B12?
Injections circumvent absorption issues but require clinic visits. High-dose oral methylcobalamin is well absorbed in most and more convenient long-term. - What is upper cervical chiropractic care?
A precise, low-force technique correcting misalignments of C1 (atlas) and C2 (axis) to relieve brainstem irritation, vascular compromise, and proprioceptive distortion. - How does atlas misalignment cause vertigo?
Atlas rotation or lateral tilt can irritate vestibular nuclei in the brainstem, kink vertebral arteries, and disrupt CSF flow—each provoking dizziness. - Is it safe?
Yes. Vector-calculated thrusts under 5 lbs, guided by 3D imaging, minimize risk. No forceful cracking or twisting is involved. - How many visits will I need?
Usually 3–4 visits over two weeks for initial stabilization, then monthly or bi-monthly maintenance depending on symptom recurrence. - Will fixing my neck remove my need for B12?
Structural realignment addresses mechanical triggers. B12 strengthens nerve health systemically. Both are essential for lasting relief. - Can I do home vestibular exercises?
Absolutely. Brandt-Daroff and Epley maneuvers are safe self-help tools, but they work best when paired with nutritional and structural support. - How do I pick a qualified upper cervical chiropractor?
Seek practitioners using CBCT imaging, nervous system scans, and instrument-based, vector-calculated adjustments—hallmarks of data-driven precision. - Any side effects of high-dose B12?
Rare—some report mild GI discomfort or acneiform eruptions. B12 is water-soluble, and excess is excreted in urine. - What if my vertigo persists?
Persistent cases warrant re-evaluation: advanced vestibular testing (VEMP, ENG), MRI to rule out central lesions, or referral to an otoneurologist.
Conclusion
Vertigo and dizziness stem from a complex interplay of biochemical, neurological, vascular, and structural factors. By harnessing the power of oral methylcobalamin supplementation—to bolster nerve health and vascular integrity—and precision upper cervical chiropractic care—to correct the mechanical root cause at C1/C2—you can break free from the cycle of episodic dizziness and reclaim your balance, confidence, and quality of life.
At Lavender Family Chiropractic in Sarasota, Florida, Dr. Jacob Temple and Dr. Will Guzinski integrate 3D CBCT imaging, functional nervous system scans, and gentle, vector-calculated adjustments with personalized nutritional protocols to deliver lasting results. If vertigo, BPPV, Ménière’s disease, MdDS, or chronic dizziness is holding you back, contact us today for a comprehensive evaluation and begin your journey to natural, effective relief.
Disclaimer: This blog is for informational purposes only and does not replace professional medical advice. Always consult your healthcare provider before beginning new supplements or treatments.
Schedule With Us!
Lavender Family Chiropractic in Sarasota Florida offers complimentary consultations to learn more about you. Click the link below!
https://intake.chirohd.com/new-patient-scheduling/724/lavender-family-chiropractic
Visit our Website!
To learn more about us go to http://www.chiropractorsarasotaflorida.com
We also service Bradenton, Parrish, Ellenton, Ruskin, Venice, Tampa, St. Pete, Osprey, Longboat, Lakewood Ranch, Myakka City.
If you are not local, visit www.uccnearme.com to find a doctor in your area!