Natural Occipital Neuralgia Relief: If you’ve been waking up with the same pain at the base of your skull for months, dreading the next migraine, or living in fear of the next jolt of facial pain that drops you to your knees — you are not imagining it, and you are not alone. Head and face pain are some of the most misunderstood, misdiagnosed, and under-treated conditions in modern medicine. Patients come to our office every week with thick folders of MRIs, blood work, neurology consults, dental exams, and prescription histories — all telling them the same thing: we don’t know why this is happening to you.
We do. And in most cases, the answer lives in a place very few providers ever look: the top two bones of your neck.
At Lavender Family Chiropractic / NeckWise North Sarasota, we are an upper cervical specialty office located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243. Our team — Dr. Rusty Lavender, Dr. Jacob Temple — focuses exclusively on the precise, gentle correction of the atlas (C1) and axis (C2) vertebrae using 3D CBCT imaging and Tytron functional nervous system scans. We proudly serve patients throughout Sarasota, Bradenton, Lakewood Ranch, Venice, Osprey, Port Charlotte, Parrish, and Palmetto, along with the surrounding Southwest Florida communities.
This post is going to walk you through three of the most painful conditions we help with — occipital neuralgia, chronic headaches and migraines, and trigeminal neuralgia — and explain why they so often share a hidden, common cause. If you only have the energy to read one section right now, skip to the one that matches your pain. We will be here when you are ready for the rest.
Why the Top of Your Neck Holds the Key to Natural Occipital Neuralgia Relief
Before we dive into the conditions themselves, we need to spend a few minutes on anatomy — because once you understand the design of the upper neck, everything else in this article will make sense.
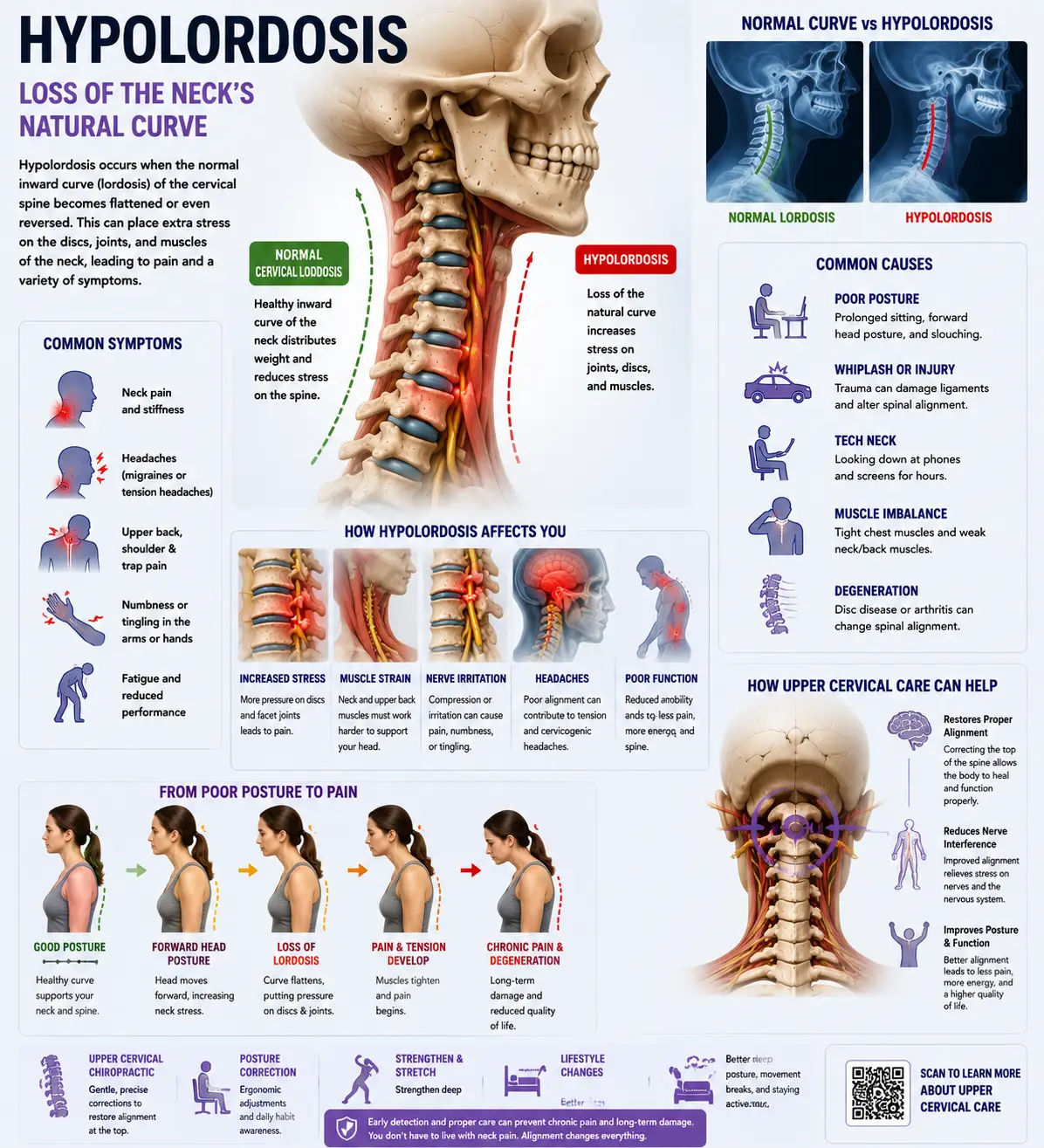
The atlas (C1) is a small, ring-shaped bone that sits directly under the skull. The axis (C2) sits beneath it. Together, these two vertebrae cradle the brainstem — the most concentrated bundle of nerve tissue in the human body. The brainstem is where the vagus nerve originates, where the trigeminal nerve nucleus extends down into, where blood and cerebrospinal fluid pass between the head and body, and where the postural reflexes that keep you upright are processed.
The greater, lesser, and third occipital nerves all emerge from this same upper neck region. The trigeminal nerve — the largest cranial nerve, responsible for sensation in your face — has a nucleus that descends down through the upper cervical spine and physically overlaps with the nerve fibers from C1, C2, and C3. This is called the trigeminocervical complex, and it’s one of the most important pieces of anatomy almost no one talks about.
When the atlas or axis loses its proper alignment — even by fractions of a millimeter — the consequences cascade. Nerves get irritated. Blood vessels get compressed. Cerebrospinal fluid drainage slows. Muscles at the base of the skull lock down to protect the area. The autonomic nervous system shifts into a low-grade fight-or-flight state. And the brain, which lives directly above all of this, starts firing pain signals it shouldn’t be firing.
This is why an atlas misalignment can show up as a headache for one person, facial pain for another, and electric shock at the base of the skull for a third. Same root cause. Different expression.
Now let’s look at each one.
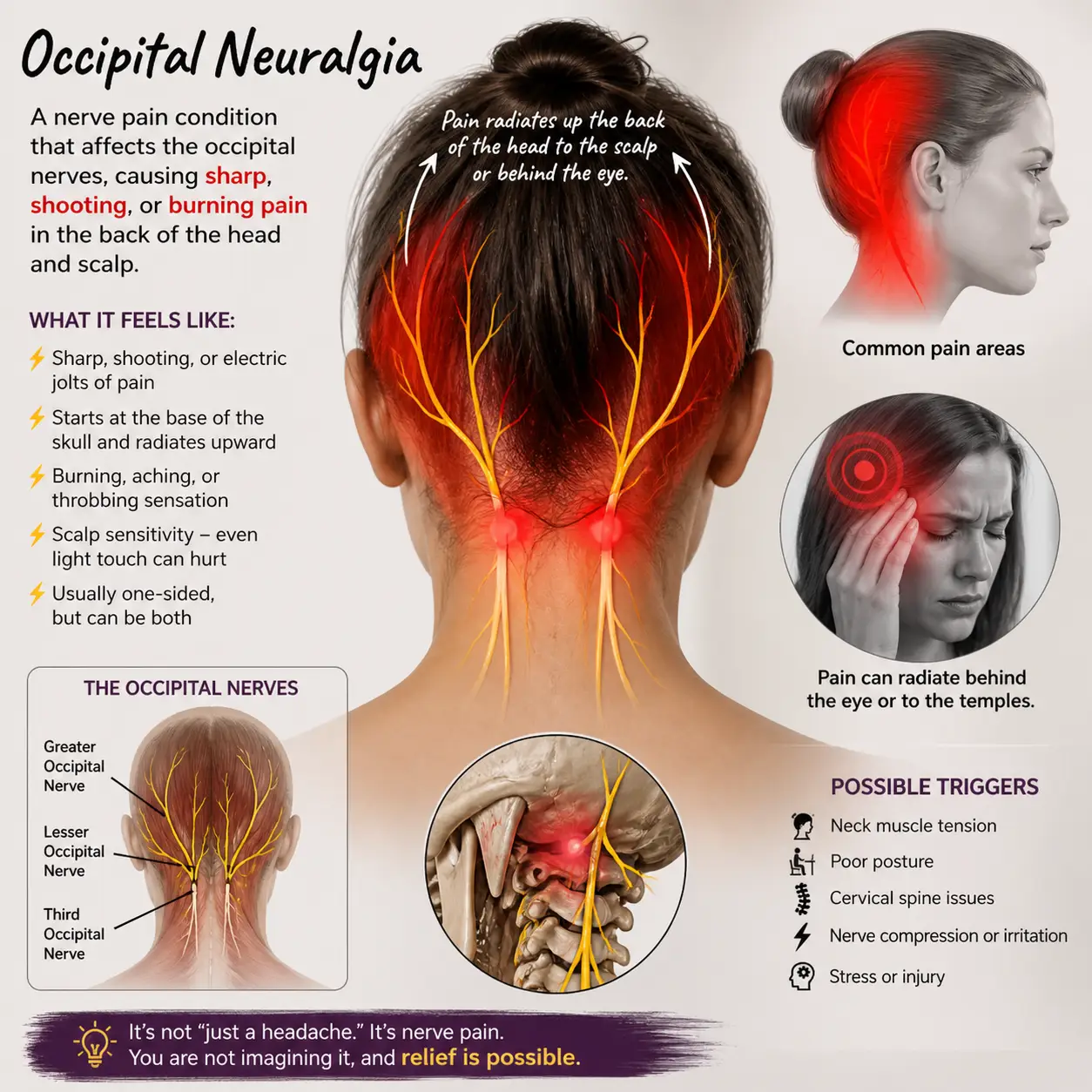
Occipital Neuralgia: The Pain That Feels Like Lightning at the Base of Your Skull
Occipital neuralgia (ON) is one of the most misdiagnosed conditions we see. Patients tell us they feel sharp, stabbing, or electric-shock pain that starts at the base of the skull and shoots upward — sometimes to the top of the head, sometimes behind the eye, sometimes across the scalp. For some, brushing their hair triggers it. For others, simply turning the head while driving sets it off. The pain can last seconds or hours, and it tends to come in unpredictable waves.
Most people with occipital neuralgia have been told they have migraines, tension headaches, or “just stress.” They’ve been prescribed muscle relaxers, anti-seizure medications like gabapentin, nerve blocks, and sometimes even surgical recommendations. Some get temporary relief; almost none get lasting relief — because none of those treatments address why the occipital nerves became irritated in the first place.
How to Tell Occipital Neuralgia From a Migraine
The two conditions overlap, but there are distinguishing features. Occipital neuralgia tends to feel sharp, electric, and shooting, while migraines tend to throb and pulse. Occipital neuralgia starts at the base of the skull and travels upward, whereas migraines often center around the temples or behind the eye. Touching the back of the head — palpation over the suboccipital muscles, or even a hairbrush — can dramatically worsen occipital neuralgia. Migraines aren’t usually that movement-dependent, while occipital neuralgia flares with neck rotation and extension. Migraines may include aura, nausea, or visual changes; occipital neuralgia often features scalp allodynia (where the skin itself feels painful to light touch) and trigger points along the suboccipital region.
That said — many patients have both, because both can be driven by the same upper cervical mechanism.
What Causes the Occipital Nerves to Get Irritated
Occipital neuralgia rarely comes out of nowhere. There’s almost always a stack of mechanical and lifestyle inputs behind it: whiplash from a car accident (even minor ones), past concussions or head trauma, falls from years ago, prolonged forward head posture from computer or phone use, repetitive stress at work, sports injuries, birth trauma, or simply the slow accumulation of micro-misalignments over a lifetime. When the atlas tilts or rotates relative to the skull, the suboccipital muscles — which are densely innervated — go into protective spasm. Those muscles wrap around and over the occipital nerves. Result: nerve compression, inflammation, and the kind of pain that doesn’t respond to ibuprofen.
Why Upper Cervical Care Works So Well for Occipital Neuralgia
When we identify a misalignment of the atlas or axis using 3D CBCT imaging and confirm nervous system stress with Tytron thermography, we can deliver a precise, gentle correction that addresses the actual mechanical irritation of the nerves. There is no twisting. No popping. No cracking. The correction is so specific that, when it holds, the body has space to settle, the suboccipital muscles release, the nerve calms, and pain often begins to decrease in days to weeks.
We’ve written extensively on this topic. If you want to go deeper, here are some of our most read pieces:
- Occipital Neuralgia Treatment Sarasota: Find HOPE Here
- Occipital Neuralgia: Proven Lasting Relief Through Atlas Alignment
- Occipital Neuralgia Treatment in Sarasota & Manatee: A Promising and Proven Treatment Option
- Occipital Neuralgia Relief in Sarasota: How Upper Cervical Chiropractic Helps You Heal at the Source
- Occipital Neuralgia: A Powerful Resolution to the Pain
Headaches and Migraines: When “Just a Headache” Isn’t Just a Headache
Over 39 million Americans suffer from migraines. Tens of millions more deal with chronic tension headaches, cluster headaches, cervicogenic headaches, hormonal headaches, and barometric pressure headaches. For most of these people, the cycle looks the same: try a medication, get partial relief, the medication stops working as well, try another medication, repeat. The frequency creeps up. The intensity gets worse. The triggers expand. And eventually, life begins to organize itself around the next headache.
We see this pattern every day at our Sarasota office, and we want to offer you a different lens.
The Brainstem-Migraine Connection
Modern migraine research has confirmed what upper cervical chiropractors have observed for decades: the brainstem plays a central role in migraine generation. The structures that sit directly beneath the atlas — the trigeminal nucleus, the vagal complex, the reticular formation, the vascular regulatory centers — are exactly the structures that go haywire during a migraine attack. When the upper cervical spine is misaligned, the irritation isn’t just mechanical. It alters cerebrospinal fluid drainage, changes blood flow dynamics in the vertebral and basilar arteries, and dysregulates the autonomic nervous system. All of these factors can lower the brain’s threshold for migraine generation — meaning your brain becomes “primed” to fire off a migraine in response to triggers that wouldn’t bother a calmer nervous system.
This is why a person with an undiagnosed atlas misalignment might experience migraines from weather changes, certain foods, lack of sleep, hormonal shifts, bright lights, or stress — while a person without that misalignment might have all the same exposures and never get a migraine.
Different Types of Headaches We Help With
Tension headaches are typically described as a band around the head, often with neck stiffness. They are very commonly cervicogenic — meaning they originate from the neck — and they respond particularly well to upper cervical correction because the suboccipital muscles and upper cervical joints are usually the source.
Migraines are throbbing, often one-sided, frequently accompanied by nausea, light and sound sensitivity, and sometimes aura. As discussed above, the brainstem-trigeminocervical connection is central to why these often improve with atlas correction.
Cervicogenic headaches start in the neck and refer pain into the head. These are almost always upper cervical in origin and are often the most dramatic to watch resolve under care.
Vestibular migraines combine migraine features with dizziness, vertigo, or balance disturbances. The vestibular system has direct connections to the upper cervical spine, which is why these patients often see significant change with care.
Barometric headaches — what we call “weather headaches” — are common in Southwest Florida, where pressure changes from approaching storms, hurricanes, and Gulf weather systems can be intense. Atlas misalignment can compound these by restricting normal venous and lymphatic drainage from the head, making the cranial vault more sensitive to pressure shifts.
Hormonal migraines in women often correlate with menstrual cycles, perimenopause, or postpartum hormonal shifts. The vagus nerve and autonomic nervous system — both heavily influenced by upper cervical alignment — play a major role in how the body responds to hormonal fluctuations.
Post-concussion headaches are some of the most life-disrupting headaches we see. Concussions almost always involve some degree of upper cervical injury, and that injury is rarely addressed in standard concussion protocols.
What “Trying Everything” Usually Means
When patients tell us they’ve “tried everything” for their headaches, they typically mean: ibuprofen, acetaminophen, triptans, beta blockers, anti-seizure meds, antidepressants used off-label, Botox injections, nerve blocks, massage, acupuncture, physical therapy, general chiropractic, dietary elimination, and various supplements. Sometimes they’ve tried 10 or 15 of these. What almost none of them have tried is a precise, specific upper cervical correction guided by 3D imaging — because that level of specificity is rare, and because most providers simply don’t think about the atlas as a primary cause of headache disorders.
This is the missing piece for many patients. Not a different drug. Not a different therapy. A different target.
If you’d like to read more about how we approach headaches and migraines specifically, here are some of our most popular blog posts:
- Migraine Treatment: Unlock Migraine Freedom in Sarasota
- Migraine: How to Resolve Migraines Naturally
- What Stretch Cures Migraines? The Real Answer for Long-Term Relief
- Top 15 FAQs About Barometric Headaches and Migraines in Bradenton
- Unlocking Lasting Migraine Relief: Magnesium Supplementation & Upper Cervical Chiropractic
- Understanding Migraines and Upper Cervical Misalignment
- Effective Relief for Vestibular Migraines: Finding Balance
Trigeminal Neuralgia: The “Suicide Disease” That Doesn’t Have to Define Your Life
Trigeminal neuralgia (TN) is widely considered one of the most painful conditions known to medicine. It has, tragically, earned the nickname “the suicide disease” because of how completely it can devastate a person’s quality of life. The trigeminal nerve — the fifth cranial nerve — provides sensation to the face. When it becomes irritated or compressed, it fires off intense, electric, stabbing pain that can be triggered by something as light as a breeze, a smile, brushing teeth, eating, drinking cold water, or applying makeup.
Patients with TN often describe it as “being struck by lightning in the face.” Episodes can last seconds to minutes and can occur dozens of times per day. There are two main types: Type 1 (classic TN), which features sudden, severe, sporadic episodes; and Type 2 (atypical TN), which involves a more constant aching or burning pain with sharp episodes layered on top.
How TN Is Usually Treated — and Why That Often Falls Short
Standard medical treatment for trigeminal neuralgia typically begins with anti-seizure medications such as carbamazepine or oxcarbazepine. These can be effective initially but often lose efficacy over time and carry significant side effects, including drowsiness, balance problems, liver issues, and cognitive fog. When medications fail, patients are commonly offered increasingly invasive procedures — nerve blocks, glycerol injections, gamma knife radiosurgery, or microvascular decompression surgery, where a surgeon physically separates the trigeminal nerve from a nearby blood vessel believed to be compressing it.
These procedures help some patients. But many patients either don’t qualify, don’t respond, or experience recurrence. And almost none of these approaches address what we believe — and what we observe clinically — to be a frequently overlooked driver of TN: irritation of the trigeminal nucleus where it descends into the upper cervical spine.
The Trigeminocervical Complex and Why It Matters
Remember the trigeminocervical complex we discussed at the start of this article? The descending portion of the trigeminal nucleus (called the spinal trigeminal nucleus) extends down to the level of C2, C3, and sometimes lower. This means that nerve input from the upper cervical spine and nerve input from the face converge in the same nucleus. Mechanical irritation, inflammation, or aberrant nerve signaling from the upper cervical region can directly influence how the trigeminal nerve behaves.
In plain English: a misaligned atlas can light up the trigeminal nerve nucleus and contribute to facial pain. Correcting the atlas can help calm it.
We have seen patients with years of trigeminal neuralgia — patients who had tried every medication and were considering surgery — experience meaningful, sometimes dramatic, reductions in symptoms after upper cervical correction held in place. We never promise outcomes, and TN is a serious condition that requires collaboration with neurology and other specialists. But for many patients, addressing the upper cervical mechanical input is the missing piece their previous care never considered.
If you’d like a deeper dive on this topic, our blog post Trigeminal Neuralgia Treatment in Sarasota: Proven for Fast Results covers our protocol, patient stories, and what to expect from a workup.
What Makes Lavender Family Chiropractic / NeckWise North Sarasota Different
Sarasota has plenty of chiropractors. So why do patients drive to us from Bradenton, Lakewood Ranch, Parrish, Palmetto, Venice, Osprey, Port Charlotte, and beyond? Here’s what sets our office apart.
We Specialize Exclusively in Upper Cervical
We do not do general chiropractic. We don’t twist, pop, or crack. We don’t adjust the lower back. Our entire focus — every patient, every day — is on the precise correction of the atlas and axis. This narrow specialization means we’ve developed a level of skill and clinical pattern recognition that simply isn’t possible in a general practice.
We Use 3D CBCT Imaging
Standard 2D X-rays cannot capture the complex, three-dimensional geometry of the upper cervical spine. The atlas is a ring-shaped bone with unique angles relative to both the skull and the axis. To know exactly how to correct it, we need to see it in three dimensions. Our 3D Cone Beam Computed Tomography scanner gives us a detailed map of your unique anatomy down to fractions of a millimeter. This isn’t a guess. It’s a measurement.
We Use Tytron Functional Nervous System Scans
Structural alignment is half the picture. The other half is how the nervous system is responding. Tytron paraspinal infrared thermography measures heat asymmetries along the spine that correlate with autonomic nervous system stress. This gives us objective, quantifiable data on whether your nervous system is in a calm, regulated state — or stuck in protection mode. We use this both to assess and to verify that corrections are holding.
Our Adjustments Are Gentle and Specific
There’s a common assumption that “more force” equals “better adjustment.” The opposite is true at the upper cervical level. The atlas is a small, precise, delicate bone. The right correction is a small, precise, delicate input — not a forceful manipulation. Our adjustments are so gentle that many patients feel almost nothing during them. The change happens over the hours and days that follow, as the body integrates the input and begins to settle.
We Verify That Corrections Hold
After an adjustment, we re-scan to make sure the correction held. If it held, we don’t re-adjust — we let your body heal. This is one of the biggest differences between upper cervical care and traditional chiropractic. We are not trying to adjust you frequently. We are trying to deliver the right input at the right time so your body can settle and stabilize.
We Listen
This sounds simple. It isn’t. Most patients with chronic head and face pain have been dismissed, rushed, or had their experience minimized somewhere along the way. Our intake is thorough. We want to know your full story — when the pain started, what’s helped, what hasn’t, what you’ve tried, what you’re afraid of, and what you most want to get back to. That story matters.
Our Service Area: Caring for Southwest Florida
Our office is located in North Sarasota at the Whitfield Avenue location, which is conveniently positioned to serve patients across the entire region. We regularly see patients from:
- Sarasota — including downtown, Lakewood Ranch corridor, and surrounding neighborhoods
- Bradenton — Manatee County’s largest city, just north of our office
- Lakewood Ranch — one of the fastest-growing master-planned communities in the country
- Venice — a short drive south on I-75 or US-41
- Osprey — between Sarasota and Venice
- Port Charlotte — coming up from the south
- Parrish — north Manatee County
- Palmetto — just across the Manatee River from Bradenton
We also serve Ellenton, Siesta Key, Longboat Key, Lido Key, Myakka City, Punta Gorda, and St. Petersburg patients regularly. If you’re outside our area entirely, we recommend visiting www.uccnearme.com to find a vetted upper cervical chiropractor near you.
What to Expect at Your First Visit
If you’ve never been to an upper cervical office, here’s what your first appointment will look like.
The conversation comes first. We sit down and listen. We want to understand your history — accidents, falls, surgeries, hormonal changes, stressors, and the timeline of your symptoms. This usually takes 30 to 45 minutes.
Examination and scans. We perform a postural and neurological evaluation, take Tytron thermography readings, and — for patients who appear to be candidates — perform a 3D CBCT scan of the upper cervical spine.
Report of findings. We sit down with you again and walk through what we found. We show you your scans on the screen. We explain what’s misaligned, why it matters, and whether we believe upper cervical care can help. If you’re not a good fit, we will tell you. If we think you’d benefit more from another specialist or modality, we’ll point you in that direction.
The correction. If you choose to move forward, your first correction is gentle, specific, and based on the exact measurements from your CBCT. There is no popping, twisting, or cracking. We re-check afterward to verify that the correction held.
Follow-through. Healing isn’t a single event — it’s a process. Your body needs time and the right environment to settle. We see you on a structured schedule designed to deliver the minimum input necessary for maximum healing. The goal is fewer adjustments over time, not more.
You Don’t Have to Live This Way
Here’s what we want you to take from this article:
If you have occipital neuralgia, chronic headaches, migraines, or trigeminal neuralgia — and you’ve been told your only options are stronger medications, more invasive procedures, or “learning to manage it” — there is another path. The upper cervical spine is a missing piece in many of these cases. And when the right correction is made by a specialist using the right tools, the body has a remarkable capacity to heal at the source.
We’ve watched patients go from 12 migraine days a month to 2. We’ve watched occipital neuralgia patients regain the ability to brush their hair without flinching. We’ve watched trigeminal neuralgia patients eat dinner with their families again — something they hadn’t been able to do in years. We don’t promise outcomes, because every body is different. But we do promise honest assessment, careful diagnostics, gentle and specific care, and a team that will work alongside you every step of the way.
Ready to Find Out If We Can Help?
We offer complimentary consultations to learn more about you and determine whether upper cervical care is the right fit. There’s no pressure, no commitment — just an honest conversation about your symptoms, your history, and your options.
Schedule your complimentary consultation here: https://intake.chirohd.com/new-patient-scheduling/724/lavender-family-chiropractic
Or call us directly: (941) 243-3729
Lavender Family Chiropractic / NeckWise North Sarasota 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 🌐 www.chiropractorsarasotaflorida.com 📱 Instagram: @lavenderfamilysrq 🎵 TikTok: @drrustylavender
Proudly serving Sarasota, Bradenton, Lakewood Ranch, Venice, Osprey, Port Charlotte, Parrish, and Palmetto — and helping patients across Southwest Florida finally heal at the root.
If you are in Tampa, Fort Myers, or Salt Lake City, you can visit our other NeckWise locations at www.neckwise.com. If you are not local to any of these, visit www.uccnearme.com to find a doctor in your area.
Your head doesn’t have to hurt forever. Your face doesn’t have to be a war zone. Your life doesn’t have to revolve around the next attack. Let’s check your atlas — and see what becomes possible.
Disclaimer: Our office is out of network with insurance. Individual results vary. Upper cervical chiropractic care is not a substitute for emergency medical care. If you experience sudden severe headache (“worst of your life”), facial droop, speech changes, double vision, or new arm/leg weakness, seek emergency care immediately.
Related Posts
Popular Posts