MdDS: If you’ve stepped off a cruise ship, gotten off a flight, or finished a long drive — and then days, weeks, or even months later you’re still feeling like you’re on the boat, you may be dealing with one of the most under-recognized and isolating balance disorders in modern medicine: Mal de Débarquement Syndrome, abbreviated as MdDS.
Translated from French, Mal de Débarquement literally means “sickness of disembarkment.” The name describes the condition perfectly. Most healthy people, after getting off a boat, plane, or long car ride, experience a brief sense of rocking or swaying — what sailors call “sea legs” — for a few minutes to a couple of days. With MdDS, that feeling never goes away. The body returns to land, but the brain stays at sea.
In a community like Sarasota, surrounded by water and a major hub for boating, cruising, and air travel, we see MdDS more often than most realize. Patients come to our office at Lavender Family Chiropractic describing a constant rocking sensation that started after a Caribbean cruise, a long flight, a fishing trip on the Gulf, or sometimes for no apparent reason at all. Many have spent months or years bouncing between ENT specialists, neurologists, and vestibular therapists, only to be told there’s nothing they can do.
Here at Lavender Family Chiropractic, located at 5899 Whitfield Avenue, Suite 107 at the corner of University and Whitfield in Sarasota, Dr. Rusty Lavender and Dr. Jacob Templespecialize in helping MdDS patients address one of the most overlooked contributors to the condition: dysfunction in the upper cervical spine. This blog will walk you through exactly what MdDS is, why it happens, what the current research shows, and how upper cervical chiropractic care fits into a complete recovery plan.
This article is part of our broader vertigo resource hub. For the full picture of how we approach dizziness as a whole, we recommend starting with our main page on vertigo care in Sarasota with Dr. Jacob Temple.
What Is Mal de Débarquement Syndrome (MdDS)?
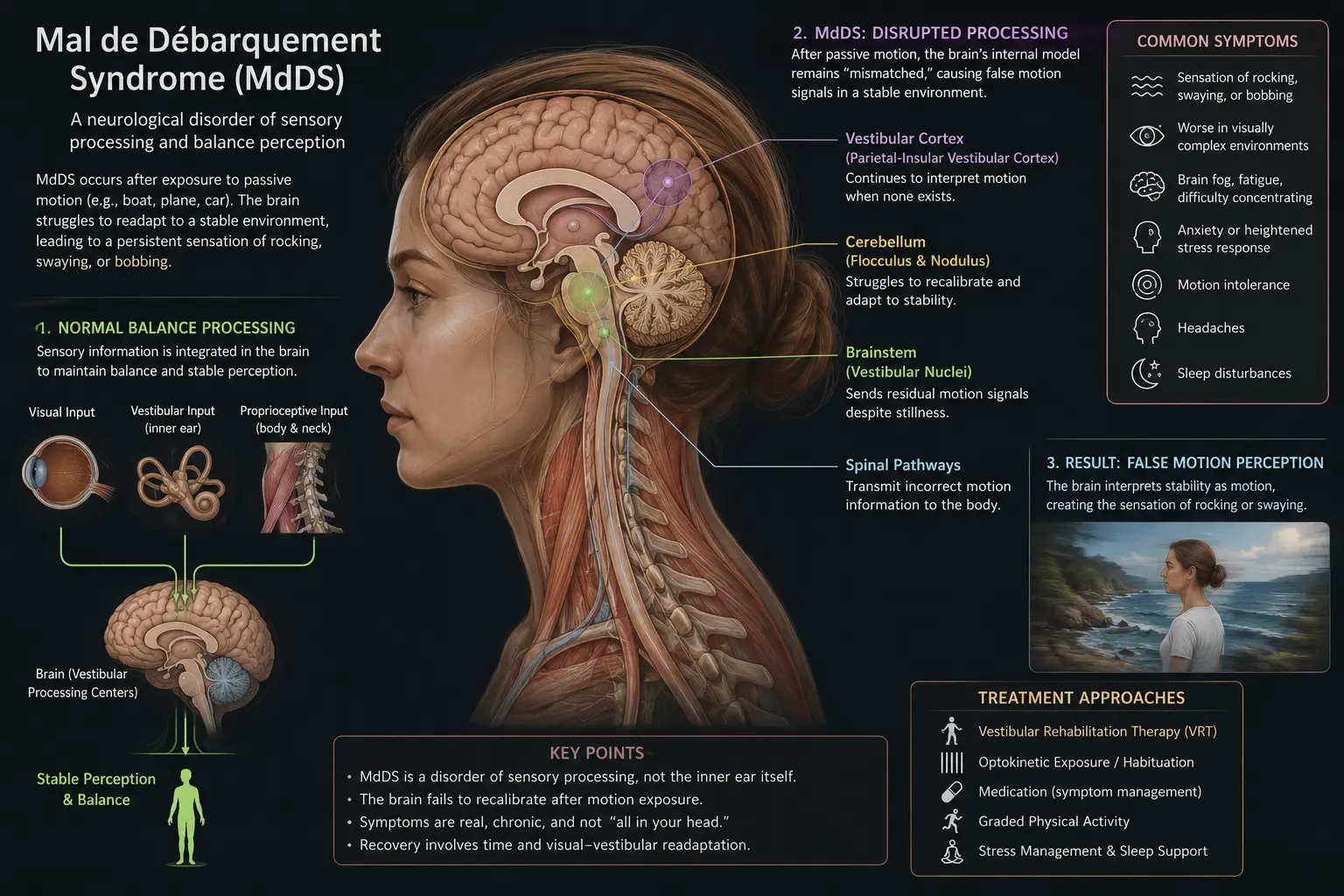
Mal de Débarquement Syndrome is a neuro-otological balance disorder characterized by a persistent, false sense of self-motion — usually described as rocking, bobbing, or swaying — that continues long after a person has stopped moving. Unlike most forms of vertigo, MdDS does NOT involve spinning. The world doesn’t whirl around the patient. Instead, it’s as if the floor underneath them is constantly moving, undulating, or shifting.
There are two recognized forms of MdDS:
Motion-Triggered MdDS (MT-MdDS): The classic form, which begins after exposure to prolonged passive motion — most commonly a cruise, but also flights, long car rides, train trips, or even time on smaller boats. The brain adapts to the constant motion of the vehicle, but then fails to fully readapt to stable ground after the motion ends.
Spontaneous-Onset MdDS (SO-MdDS): Less common but well-documented, this form appears with no clear motion trigger. Patients describe waking up one day with the rocking sensation, or developing it gradually without any cruise, flight, or travel history.
Common symptoms of MdDS include:
- A constant rocking, bobbing, or swaying sensation
- Feeling like the floor is moving or undulating beneath you
- Feeling like you’re still on a boat even while standing on solid ground
- Walking that feels unsteady or staggering
- Fatigue and brain fog
- Difficulty concentrating
- Heightened sensitivity to visual motion (busy stores, scrolling, large screens)
- Increased motion sickness susceptibility
- Sensitivity to light, noise, and crowds
- Anxiety, depression, or mood changes from the chronic nature of the condition
One of the most unusual diagnostic features of MdDS is that symptoms often improve temporarily when the patient is in motion again — riding in a car, on a train, or back on a boat — and then return when the motion stops. This is the opposite of most balance disorders, where motion typically worsens symptoms.
According to current literature, MdDS predominantly affects women aged 30 to 60, though it can occur in anyone. The connection between MdDS and migraines is well documented — people with a history of migraines are significantly more likely to develop MdDS. Symptoms can last anywhere from days to months to years, and in some cases the condition becomes chronic and life-altering.
Critically, MdDS often gets dismissed or misdiagnosed because routine vestibular and neurological tests come back normal. MRIs show nothing abnormal. ENT specialists confirm the inner ear looks fine. And yet the rocking continues. This is part of what makes this condition so isolating — patients know something is wrong, but the standard medical workup can’t show what.
How MdDS Affects Your Nervous System and Sensory Processing
To understand why MdDS is so persistent — and why upper cervical chiropractic care can make a meaningful difference — you have to look at what’s actually happening in the brain.
Your sense of balance and self-motion depends on the brain integrating three sensory inputs:
- Vestibular input from your inner ear
- Visual input from your eyes
- Proprioceptive input from your joints and muscles, especially in the neck
When you’re on a boat or plane for an extended period, your brain adapts to the constant motion. It recalibrates the vestibulo-ocular reflex (VOR) — the reflex that stabilizes your vision during head movement — and adjusts what’s called velocity storage, a functional component of the vestibular system that handles ongoing motion perception. This adaptation is helpful while you’re in motion; it’s why most people stop feeling seasick after a day or two on a cruise.
The problem with MdDS is that the brain fails to readapt when the motion ends. The velocity storage and VOR remain in their “boat mode,” continuing to generate a sense of motion even though the body is now perfectly still. According to recent research published in Frontiers in Neurology, MdDS appears to be caused by maladaptation of the velocity storage mechanism — and the most effective specialized treatments aim to readapt that mechanism through targeted visual-vestibular protocols.
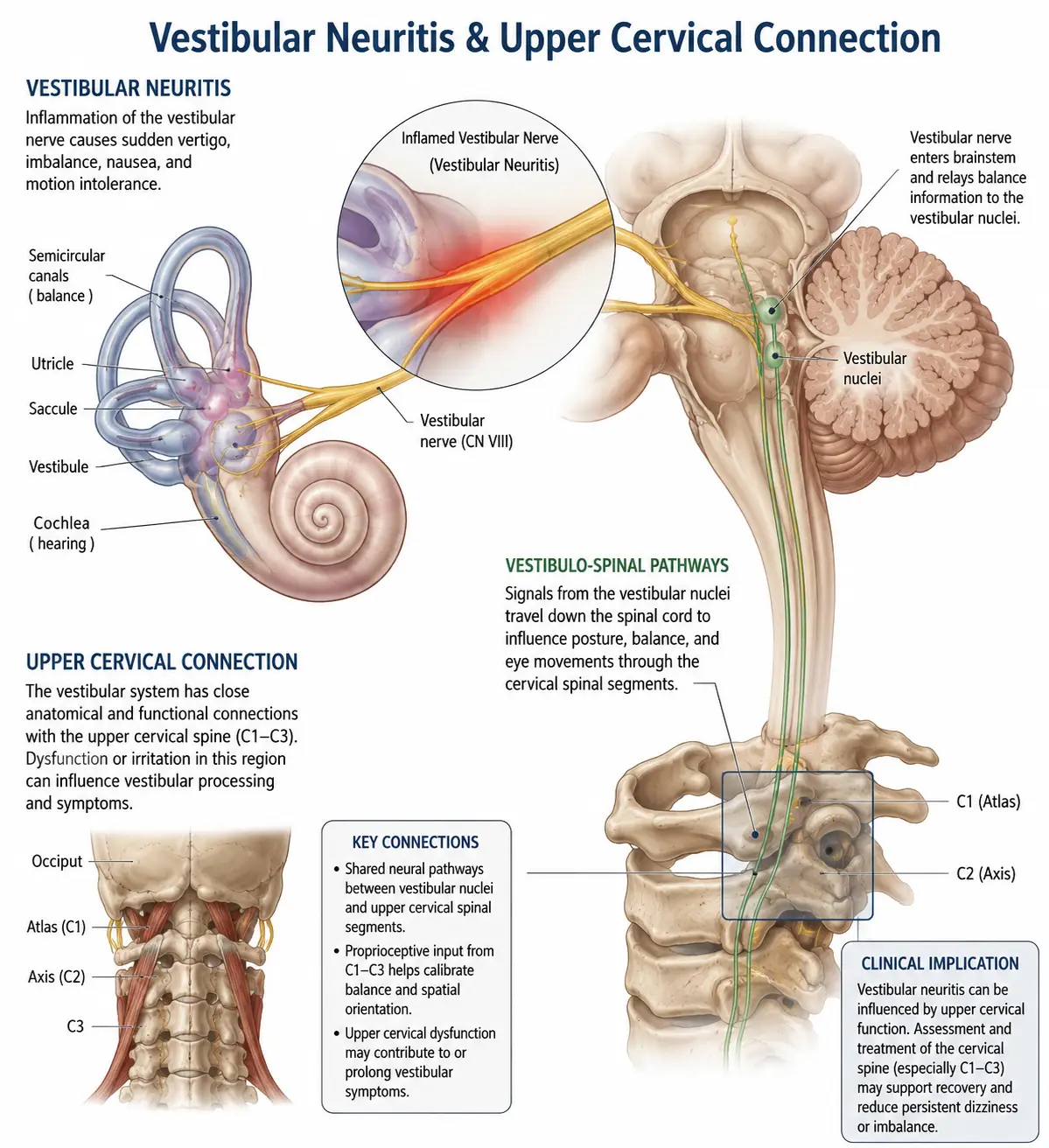
But here’s where the upper cervical spine comes in. The velocity storage mechanism and VOR are coordinated in the brainstem and cerebellum — exactly the structures that sit immediately adjacent to your upper cervical spine. Dysfunction in the upper neck affects this region through several pathways:
1. Proprioceptive input. The upper neck contains the highest density of mechanoreceptors anywhere in the spine. These sensors feed positional data directly to the vestibular nuclei and cerebellum — the same regions that need to readapt for MdDS recovery. Faulty neck proprioception interferes with the brain’s ability to recalibrate.
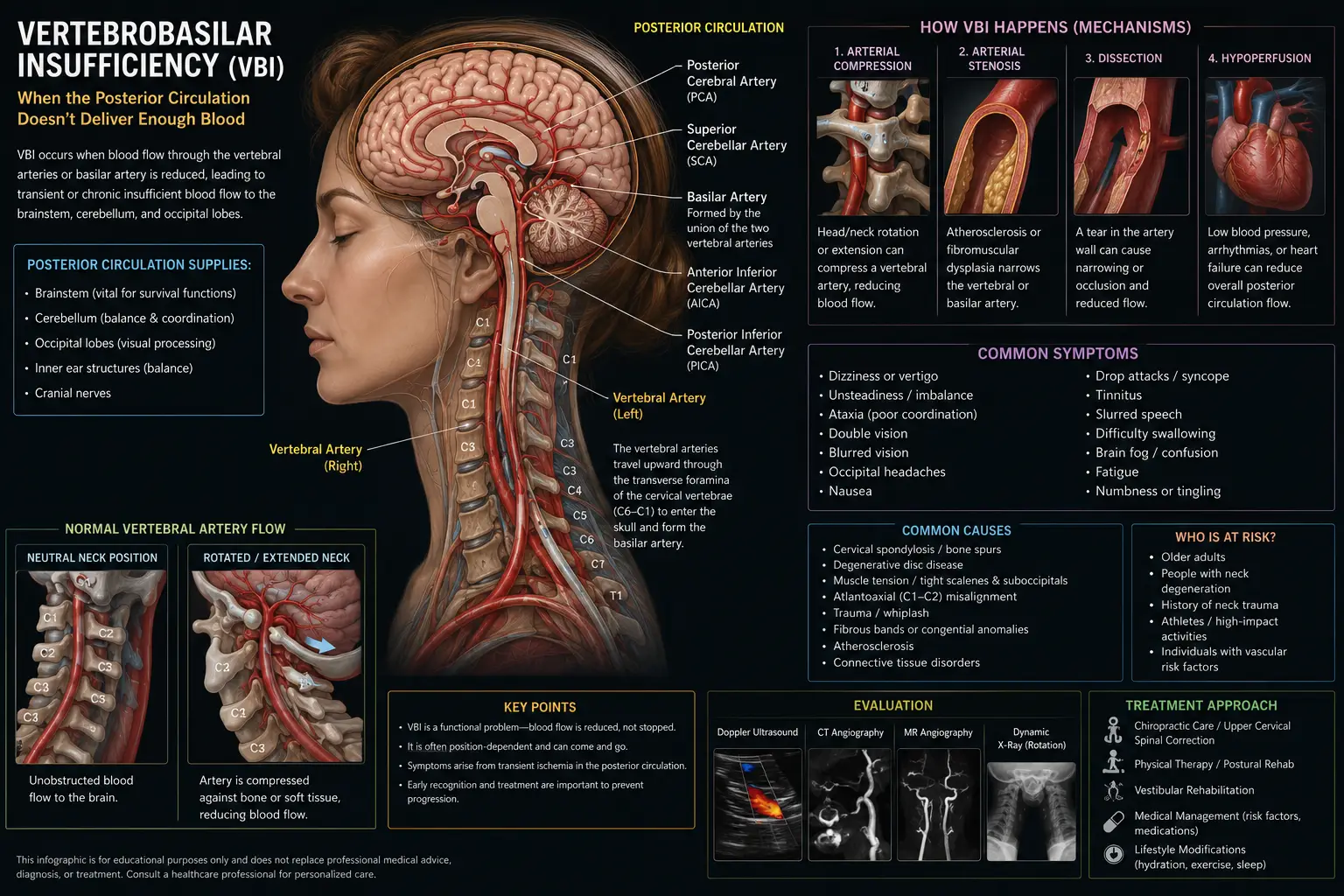
2. Brainstem signaling and vascular supply. The vertebral arteries pass through the bones of the upper cervical spine before supplying the brainstem, cerebellum, and inner ear. Upper cervical misalignment can subtly compromise blood flow to the very structures that need to reorganize for MdDS recovery.
3. Vagus nerve and autonomic regulation. The vagus nerve exits the skull right next to the atlas (C1). Patients frequently experience autonomic symptoms — fatigue, brain fog, anxiety, light and sound sensitivity, and digestive disruption — many of which trace back to vagal dysregulation. Upper cervical dysfunction directly affects vagal tone.
4. Trigeminocervical complex. The upper cervical spine and the trigeminal nerve share a sensory hub in the brainstem. When this hub is irritated by upper cervical dysfunction, the brain becomes hypersensitive to motion, light, sound, and visual complexity — exactly the pattern MdDS patients describe.
In short: MdDS is fundamentally a brain-adaptation problem, and the upper cervical spine plays a major role in whether the brain can successfully readapt.
Why the Upper Cervical Spine Matters in MdDS Recovery
A common question we hear from MdDS patients is: “If my MdDS started after a cruise, why does my neck have anything to do with my recovery?”
The answer comes down to two main factors: what the upper cervical spine does for balance signaling, and what often happens to the neck during the triggering event.
What the upper neck does for balance signaling: The atlas (C1) and axis (C2) house an extraordinary density of position sensors and connect directly to the brainstem’s vestibular processing centers. When these sensors send clean, accurate data, the brain has reliable input to recalibrate after a motion experience. When they send faulty data — because of misalignment, joint dysfunction, or muscle tension — the brain’s recalibration stalls. The “boat mode” stays on.
What often happens during the trigger event: This is the piece most MdDS patients never get explained to them. The triggering event — a cruise, flight, long drive — often involves significant upper cervical strain:
- Sleeping in awkward positions on a boat or plane
- Bracing your neck against the constant motion for days
- Sitting in cramped airplane or car seats with forward head posture
- Lifting heavy luggage
- Carrying tension and stress associated with travel
- For boats specifically, constantly stabilizing the head against rolling motion using deep neck muscles
By the time the trip ends, the upper cervical spine is in a different state than when it started. The brain now has to readapt to stable ground using a neck that’s also sending altered signals. Recalibration stalls. The rocking continues.
For spontaneous-onset MdDS, the upper cervical involvement is often even more important — because there’s no obvious external trigger, the source of dysfunction is more likely internal: long-standing postural patterns, prior injuries, hormonal shifts, or migraine biology that has affected the cervicovestibular system over time.
Upper cervical chiropractic care is one of the most direct ways to give the brain clean proprioceptive input again — which is exactly what MdDS recovery requires. It doesn’t replace VOR readaptation therapy. It works alongside it, by giving the brain a stable foundation to readapt from.
Upper Cervical Chiropractic Care for MdDS: What to Expect
At Lavender Family Chiropractic, we approach MdDS care in a careful, gentle, and measured way. Many of our MdDS patients have been searching for help for months or years. They’ve often tried multiple approaches with limited or temporary success. We treat that history with the seriousness it deserves.
Here’s what your journey looks like at our Sarasota office.
Step One: Comprehensive Consultation
Your first visit starts with a real conversation. Dr. Lavender or Dr. Temple will sit down with you and learn the full story — when the rocking started, what triggered it (if anything), what diagnoses you’ve received, what treatments you’ve tried, what’s helped, what hasn’t, and how MdDS has impacted your life. This isn’t a five-minute intake. MdDS is complex, and details matter.
Step Two: 3D CBCT Imaging and Neurological Scanning
Next, we use 3D CBCT X-ray technology to take precise three-dimensional images of your upper cervical spine. This imaging shows us — down to the millimeter — exactly how your atlas (C1) and axis (C2) are positioned, allowing us to calculate the precise corrective vector your spine needs.
We pair this with paraspinal infrared thermography to assess nervous system function along your spine. This is particularly useful for MdDS patients because it reveals patterns of autonomic stress and nervous system overactivity that often correspond to the rocking, sensitivity, and fatigue you’re experiencing.
Step Three: A Gentle, Specific Correction
When you receive your upper cervical correction, you’ll likely be surprised at how gentle it is. There is no twisting, popping, or cracking. We use the Advanced HIO Knee Chest Upper Cervical Technique (AHKC), one of the gentlest and most precise methods of upper cervical correction available.
For MdDS patients especially, gentleness matters. Your nervous system has been on high alert for some time, and anything aggressive or forceful around your head and neck can set you back. Our technique is built to work with your nervous system, not against it.
Step Four: Monitoring and Stabilizing Your Recovery
The goal of upper cervical care isn’t to adjust you over and over again. The goal is to help your spine hold its corrected position, so your brain can finally complete the readaptation it’s been struggling to make. We track your progress visit by visit — symptoms, alignment, and nervous system function — and adjust your care plan as you stabilize.
Most MdDS patients begin noticing small but meaningful changes within the first few weeks: less constant rocking, better tolerance to visual motion, reduced fatigue, clearer thinking, and improved sleep. MdDS recovery is often gradual and stepwise — but the trajectory is almost always positive when the upper cervical piece is addressed.
Has MdDS taken over your life since that cruise, flight, or long drive? Call us at (941) 243-3729 or book a complimentary consultation online. We’ll help you figure out whether upper cervical care is the missing piece for you.
What the Research Says About MdDS
The scientific literature on MdDS has expanded meaningfully in the past few years. Here are the most relevant findings.
A 2024 paper published in Frontiers in Neurology established the first standardized treatment guideline for MdDS based on vestibulo-ocular reflex (VOR) readaptation therapy. The study demonstrated an overall success rate of approximately 64 percent in patients treated with this protocol — including both motion-triggered and spontaneous-onset cases. Researchers concluded that VOR readaptation is currently the most effective dedicated treatment for MdDS, though it does not work for everyone, and some patients experience symptom return after subsequent travel.
Earlier clinical research published through the National Institutes of Health (clinicaltrials.gov) reported success rates as high as 75 percent immediately after VOR readaptation treatment for motion-triggered MdDS, with some patients achieving complete remission. However, the same research noted that the brain remains susceptible to retriggering, which is why post-treatment lifestyle support matters so much.
The American Brain Foundation describes MdDS as a rare neurologic disorder thought to stem from issues with the vestibular system, with no current cure but a growing body of effective management strategies. Stress management, regular exercise, healthy eating, sleep hygiene, and low-dose anti-seizure medications (such as clonazepam) are sometimes used as supportive treatments.
What’s striking across the literature is the consistent finding that MdDS is not a structural disorder — it’s a functional problem with how the brain processes and adapts to motion. This is exactly the type of condition where supporting the nervous system through gentle, precise upper cervical correction can produce meaningful benefit, particularly when combined with VOR-based rehabilitation when available.
The takeaway: MdDS is real, it’s treatable, and recovery often requires a layered approach. Upper cervical chiropractic care addresses one of the most overlooked layers — the role of the upper neck in feeding accurate proprioceptive data to the brainstem during the readaptation process.
Lifestyle Habits That Support Recovery from MdDS
Beyond upper cervical care, daily habits make a major difference in MdDS recovery. Here’s what we recommend most often to our patients.
Move regularly, but mindfully. MdDS instincts will tell you to hold still or avoid anything that feels triggering. The opposite is what your nervous system needs. Gentle, daily walking — outside on stable ground — gives your brain consistent, accurate sensory input to recalibrate from.
Reduce visual overload — gradually. Scrolling phones, watching action movies on large screens, and prolonged exposure to busy visual environments can flare MdDS. But complete avoidance also strengthens visual dependency. Gradual exposure within tolerance helps build resilience.
Sleep well. Your brain does most of its readaptation work during sleep. Aim for 7–9 hours per night and use a supportive pillow that maintains proper upper cervical alignment. Stomach sleeping is particularly disruptive and should be avoided.
Stay hydrated. Inner ear fluid balance and overall nervous system function depend on hydration, and Florida’s heat and humidity make dehydration a daily risk. Half your body weight in ounces of water per day is a solid target.
Manage stress and anxiety. MdDS and anxiety often reinforce each other. Breathing exercises, walks outside, time off screens, and when appropriate, professional support are all powerful interventions. Many MdDS patients find significant relief by addressing the autonomic and emotional layer of the condition alongside the physical one.
Be cautious about retriggering. After MdDS has resolved or significantly improved, future travel — especially cruises and long flights — can retrigger symptoms. Many patients learn to plan ahead with hydration, sleep, gentle movement, and post-travel recovery time to reduce the risk of relapse.
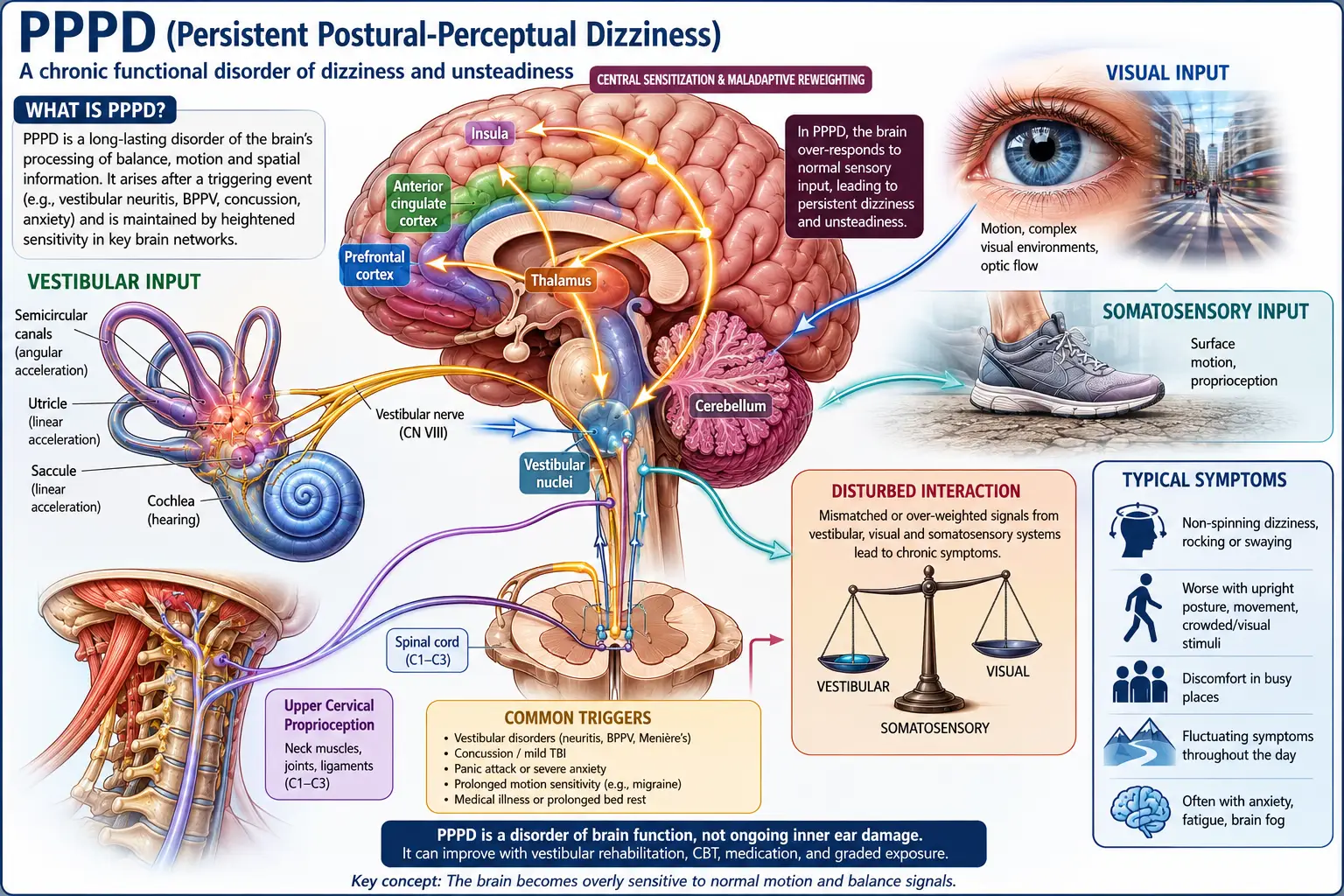
Address related conditions. MdDS frequently overlaps with vestibular migraine, PPPD, and motion sickness. For a deeper look at how vestibular conditions and motion sensitivity overlap, our blog on whether vertigo and motion sickness are the same thing is an excellent companion read.
Be patient. MdDS recovery is rarely linear. Good days are followed by hard days. The trajectory matters more than any single day. With the right combination of care, support, and time, most patients see meaningful improvement.
Serving Sarasota and Surrounding Areas
Lavender Family Chiropractic is located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — right at the corner of University and Whitfield. We are easy to reach from anywhere in the greater Sarasota region.
We proudly serve MdDS patients and others dealing with chronic balance disorders from across the area, including:
- Sarasota, FL
- Bradenton, FL
- Lakewood Ranch, FL
- Venice, FL
- Osprey, FL
- Parrish, FL
- Ellenton, FL
- Siesta Key, FL
- Longboat Key, FL
- St. Pete, FL
- Tampa, FL
To learn more about the full region we serve, visit our areas we service page. No matter where you’re driving from, we’re set up to help.
Top 15 FAQs About MdDS
What is MdDS in simple terms?
MdDS is a chronic balance disorder where you feel like you’re constantly rocking, bobbing, or swaying — often as if you’re still on a boat — even when you’re standing on solid ground. It usually starts after a cruise, flight, or long drive, but can also begin without any clear trigger.
How is MdDS different from regular sea legs?
After a cruise or boat trip, most people feel a brief rocking sensation that resolves within minutes to a couple of days. MdDS is when that feeling doesn’t go away — lasting weeks, months, or years. It’s the body’s failure to fully readapt to stable ground after extended motion.
Is MdDS the same as vertigo?
No. True vertigo involves a spinning sensation. MdDS involves rocking, bobbing, or swaying — no spinning. Both are forms of dizziness, but they feel very different and have different underlying mechanisms.
Can MdDS be diagnosed with imaging?
Not directly. MdDS is a clinical diagnosis based on the pattern of symptoms and history. MRIs, CT scans, and standard vestibular tests typically come back normal, which is part of what makes MdDS so frustrating to live with.
Who typically gets MdDS?
MdDS most commonly affects women aged 30 to 60, although it can occur in anyone. People with a history of migraines are at higher risk. The connection between hormones and MdDS is still being studied.
How long does MdDS last?
Some cases resolve within days to weeks, especially in younger people. Others persist for months or years, and a subset becomes chronic. With targeted care — including VOR readaptation therapy when available, upper cervical correction, and lifestyle support — most patients see meaningful improvement.
Why do I feel better when I’m in motion again?
This is one of the hallmark features of MdDS. Because your brain is stuck in “motion mode,” being back in motion temporarily matches what the brain expects — which paradoxically eases symptoms. Symptoms return when the motion stops because the brain is still maladapted.
Can upper cervical chiropractic actually help MdDS?
Yes. While upper cervical care doesn’t directly readapt the VOR, it addresses one of the most overlooked contributors to the condition — faulty proprioceptive input from the upper neck. Clean neck signaling gives the brainstem and cerebellum the stable input they need to recalibrate.
Is upper cervical care safe for MdDS?
Yes. Upper cervical chiropractic is one of the gentlest forms of chiropractic care available. There is no twisting, popping, or cracking. Corrections are precise, light, and calculated from advanced imaging — appropriate even for the most motion-sensitive patients.
How soon should I seek care after my MdDS started?
The sooner the better. The longer MdDS persists, the more entrenched the maladaptation becomes in the brain. That said, it’s never too late — patients with multi-year MdDS frequently see meaningful improvement once the upper cervical piece is addressed.
Should I avoid cruises and flights forever after MdDS?
Not necessarily. Many MdDS patients return to travel successfully once their symptoms have stabilized, especially with planning, hydration, sleep, and recovery time on either side. But because retriggering is possible, post-recovery travel deserves thoughtful preparation.
Are medications helpful for MdDS?
Some patients benefit from low-dose anti-seizure medications such as clonazepam, although these are typically used short-term to reduce symptom intensity rather than to address the underlying mechanism. Long-term use of vestibular suppressants is generally discouraged because they can interfere with the brain’s readaptation.
Can stress make my MdDS worse?
Yes. Stress increases sympathetic nervous system activity, tightens the muscles around the upper neck, and amplifies dizziness and sensory sensitivity. Stress management is an important part of MdDS recovery.
Is MdDS related to migraine?
Yes — there’s a well-documented overlap. People with a history of migraines are more likely to develop MdDS, and the underlying brain biology shares features (heightened sensory sensitivity, brainstem involvement). Many MdDS patients benefit from migraine management strategies alongside MdDS-specific care.
How do I know if Lavender Family Chiropractic is right for me?
If you’ve been told you have MdDS, suspect you have MdDS, or have a persistent rocking or swaying sensation that started after travel and won’t fully resolve, you’re an excellent candidate for an evaluation. Call (941) 243-3729 to schedule a complimentary consultation and we’ll help you figure out whether upper cervical care fits into your recovery plan.
You Don’t Have to Live on the Boat Forever
MdDS is one of the most isolating dizziness conditions to live with. It’s invisible to other people. Standard tests come back normal. And the rocking, the swaying, the constant motion that nobody else can see — it wears on you over time. Many of our MdDS patients describe years of feeling unheard, dismissed, or told it’s “just anxiety.”
It’s not anxiety. It’s a real, neurological adaptation problem — and there are real ways to support recovery.
At Lavender Family Chiropractic, Dr. Rusty Lavender and Dr. Jacob Temple have helped many patients across Sarasota and beyond finally find their land legs again. If you’ve been stuck on the boat for too long, we’d be glad to help you understand whether upper cervical care can be part of your way back to solid ground.
📞 Call us today at (941) 243-3729 📅 Or book your complimentary consultation online
You don’t have to keep rocking.
Related Articles
- Vertigo Sarasota: Dr. Jake’s #1 Way to Resolve Dizziness
- Are Vertigo and Motion Sickness the Same Thing? Our #1 Guide to Proven Results
- Alternative Doctor for Vertigo in Sarasota and Manatee County: Our #1 Proven Method to Resolve Dizziness
By Dr. Rusty Lavender and Dr. Jacob Temple — Lavender Family Chiropractic, Sarasota, FL
Related Posts
Popular Posts