By Dr. Rusty Lavender
Cervical Herniated Disc Treatment and Relief in Sarasota Florida: Few words land harder than “herniated disc.” For many people, the diagnosis arrives with an MRI image and a grim explanation: a disc in your neck has ruptured, the soft inner material is pushing out, and it is pressing on something it should not. It sounds like structural failure, like a part has broken and the only real fix is surgery. That fear is understandable, and it is also, in most cases, larger than the reality warrants.
If you are in Sarasota, Bradenton, Lakewood Ranch, or anywhere along the Gulf Coast and you have been told you have a cervical herniated disc, here is the single most important thing to understand from the outset: the great majority of cervical disc herniations improve without surgery, many of them resorb and shrink on their own over time, and herniated discs are common even in people who have no pain at all. The herniation is real, but it is rarely the catastrophe it sounds like, and the path forward for most people is conservative care, not the operating room.
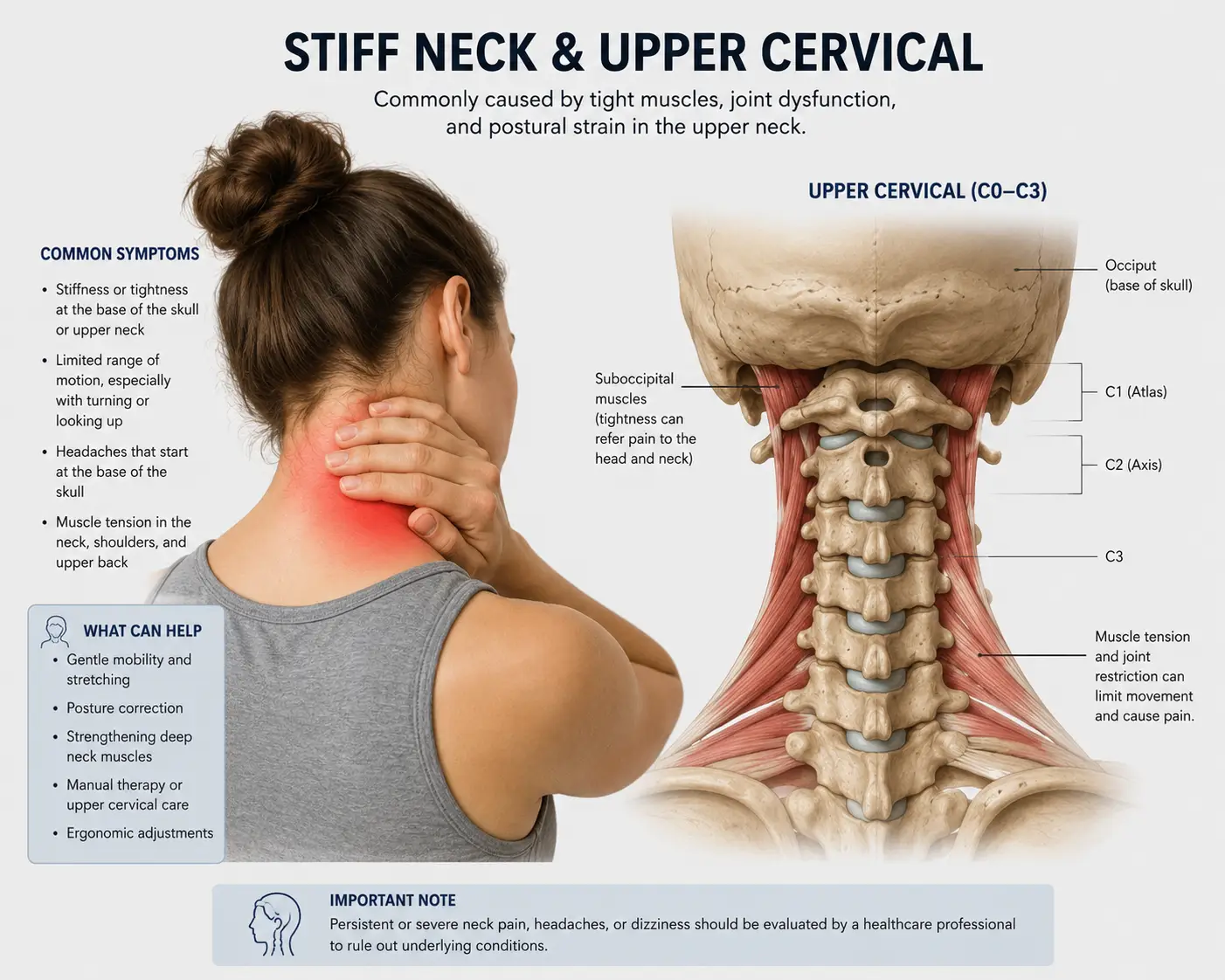
At Lavender Family Chiropractic in Sarasota, our entire focus is the upper cervical spine, the atlas (C1) and axis (C2) at the very top of the neck. We use 3D CBCT imaging and paraspinal infrared thermography to understand your cervical spine as a whole system, and we correct upper cervical misalignment with the gentle, precise Knee Chest Upper Cervical technique, with no twisting, popping, or forceful manipulation of an injured, sensitive neck. We want to be honest with you from the first sentence, because honesty is the foundation of good care: we do not claim that an upper cervical adjustment repairs a herniated disc or pushes it back into place. No provider who is being straight with you would. What we can do is explain what a herniation actually is, why most of them get better, where upper cervical care genuinely fits into a recovery strategy, and how to support your body’s own well-documented capacity to heal.
What Is a Cervical Herniated Disc?
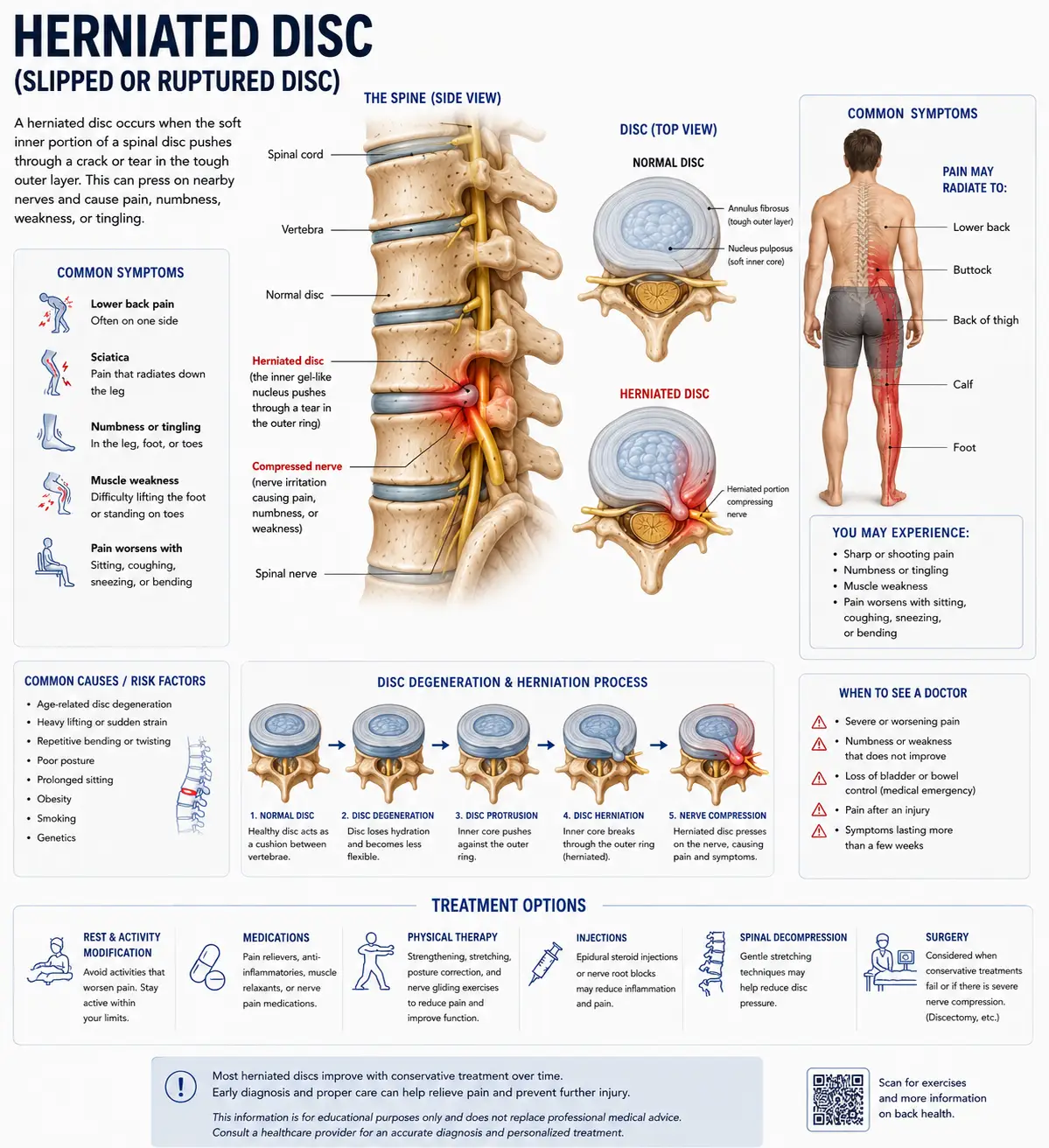
To understand a herniation, you first have to understand the disc. Between each pair of vertebrae in your neck sits an intervertebral disc, a cushion that absorbs shock and allows movement. Each disc has two parts: a tough, fibrous outer ring called the annulus fibrosus, and a soft, gel-like center called the nucleus pulposus. Think of it loosely like a jelly donut, a firm outer shell surrounding a softer center.
A herniated disc occurs when the soft inner material pushes outward through a weakened or torn area of the outer ring. Depending on how far it goes, clinicians use different terms. A bulge is a broad, generalized extension of the disc beyond its normal margin. A protrusion is a more focal pushing-out where the outer ring is still intact. An extrusion is when the inner material breaks through the outer ring. A sequestration is when a fragment separates entirely. These distinctions matter, because, as we will see, the more dramatic-sounding extrusions and sequestrations are often the ones most likely to resorb on their own.
When a herniation causes symptoms, it is usually because the displaced material does one of two things, or both. It can mechanically press on a nearby structure, a nerve root or, less commonly, the spinal cord. And it can provoke a local chemical inflammatory reaction, which irritates the surrounding tissues. This is a key point: much of the pain from a herniated disc comes not from the mechanical pressure alone but from inflammation, which is one reason symptoms so often settle even when the disc itself is still present on imaging.
It is essential to understand that a herniated disc is not the same thing as the symptoms it can cause. When a cervical herniation irritates a nerve root, producing arm pain, numbness, tingling, or weakness, that downstream nerve problem is called cervical radiculopathy, which we cover in depth in our guide on pinched nerve in the neck. This blog is about the disc itself. The herniation is the structural event; the radiculopathy is one possible consequence of it. Many herniations produce only local neck pain, and many produce no symptoms at all.
How Common Are Herniated Discs, Really?
This is where the picture becomes far more reassuring than the diagnosis usually sounds, because the prevalence data reframes everything. Herniated and bulging discs are extraordinarily common in people who have no pain whatsoever.
A landmark systematic review of imaging findings in asymptomatic individuals, published in the American Journal of Neuroradiology by Brinjikji and colleagues, pooled data from 33 studies covering more than 3,000 pain-free people. It found that disc degeneration was present in 37% of asymptomatic 20-year-olds, rising to 96% of asymptomatic 80-year-olds, with disc bulges increasing from 30% of 20-year-olds to 84% of 80-year-olds, and disc protrusions present in 29% of 20-year-olds rising to 43% of those aged 80. Read that carefully: these are people with no symptoms at all, and yet bulges and protrusions are present in a large and rising share of them.
The clinical significance of this is enormous, and it is something we want every patient to absorb. Because herniations and bulges are so common in people without any pain, the appearance of a herniation on your MRI cannot, by itself, prove that the herniation is the cause of your pain. Imaging findings and symptoms correlate imperfectly. This is genuinely liberating news, because it means your pain is not a simple, direct readout of how bad your disc looks on a scan, and it means that the presence of a herniation does not doom you to a lifetime of pain or to surgery.
Cervical disc herniation as a symptomatic condition tends to appear in adulthood, most commonly affecting people in their thirties through fifties, with the inner gel-like material pushing out and provoking a combination of mechanical pressure and inflammation. But the headline remains: many discs that look herniated on imaging are causing no trouble at all.
The Body Heals Herniated Discs: What the Research Shows
Here is the part of the story that most people are never told, and it changes everything about how to approach this diagnosis. Herniated discs frequently shrink, resorb, and even disappear on their own, without any surgery.
A 2026 review in the American Journal of Medicine on the pathophysiology, diagnosis, and management of cervical disc herniation concluded plainly that the majority of cases improve with nonsurgical care, with 80 to 85% resolving within 8 to 12 weeks without surgery, and that surgical evaluation is reserved for cases involving myelopathy, progressive neurologic deficits, or chronic treatment-refractory symptoms. Eighty to eighty-five percent, getting better within roughly three months, without an operation. That is the natural history of this condition for most people.
How does the body accomplish this? The mechanism is well studied. A literature review in Surgical Neurology International describes how spontaneous regression of a herniated cervical disc occurs through several processes: dehydration and shrinkage of the herniated material, retraction of the protruded disc, and enzymatic degradation and phagocytosis of the extruded material driven by an inflammatory and neovascularization response. In plain terms, when disc material pushes out far enough to be exposed to the body’s blood supply, the immune system recognizes it as foreign and gradually clears it away, like cleaning up debris. Strikingly, the review notes that larger, more dramatic herniations, the extrusions and sequestrations, are often the most likely to regress, precisely because they are more exposed to that vascular clean-up process.
This is the honest, evidence-based reason we are optimistic with herniated disc patients, and it is also why we are careful never to overclaim. We do not need to tell you that an adjustment “sucks the disc back in,” because that is not how recovery works and it would not be true. The truth is better: your body has a genuine, documented capacity to heal a herniated disc on its own, and the role of good conservative care is to support that process, manage the symptoms while it unfolds, and address the mechanical factors that influenced the disc in the first place.
The Upper Cervical Connection: Where Alignment Fits Into the Picture
If most herniations heal on their own, why involve the upper cervical spine at all? The answer is about influencing the mechanical environment in which the disc sits, both to support recovery and to reduce the risk of recurrence and the stress on neighboring discs.
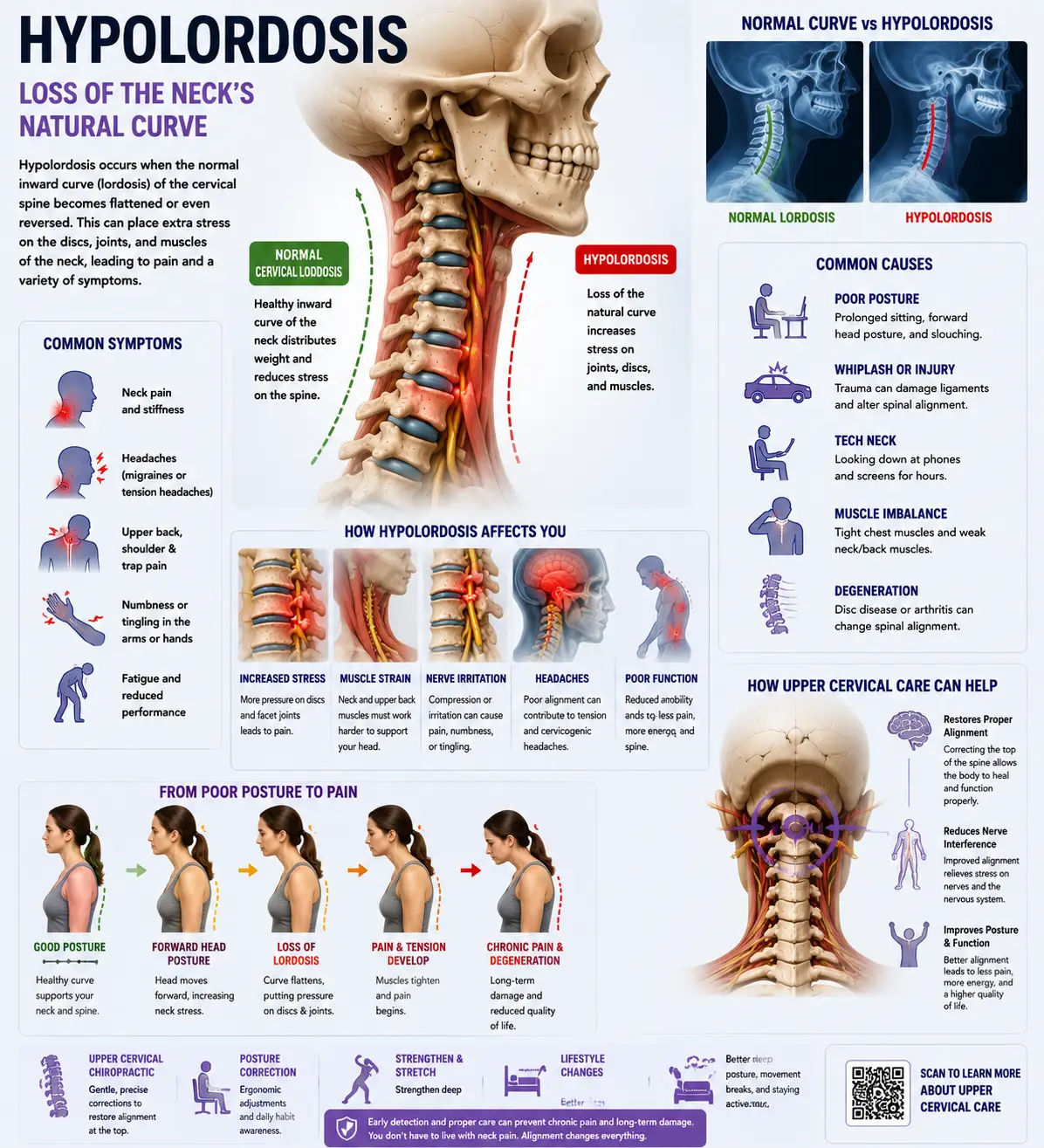
The cervical spine functions as a single, integrated system, and the alignment of the atlas and axis sets the mechanical baseline for every disc below them. The atlas and axis form the craniocervical junction at the top of the neck, the region responsible for keeping your head level and your eyes oriented to the horizon. When the atlas sits even slightly out of position, your body compensates by side-bending and rotating the vertebrae below to bring the head back toward horizontal. Those compensations propagate downward through the lower cervical spine, the very region, especially C5/C6 and C6/C7, where most cervical herniations occur.
The consequence over time is that a chronic upper cervical misalignment loads the lower cervical discs unevenly. One side of a disc bears more pressure than it was designed to handle, year after year. Uneven, excessive loading is one of the mechanical factors that weakens the annulus and sets the stage for a herniation in the first place, and it is also a factor that can slow recovery and drive herniations at adjacent levels after one disc has already failed. This is why addressing the loading pattern matters even though we are not touching the herniated disc directly.
By restoring proper upper cervical alignment, the goal is to allow the lower cervical spine to be loaded more evenly going forward, which reduces the chronic, asymmetric stress on the injured disc and its neighbors. This does not “repair” the herniation. What it does is improve the mechanical environment so that the body’s natural resorption process can proceed with less ongoing mechanical aggravation, and so that the discs above and below the injured level are not pushed toward the same fate.
There is a second dimension worth understanding. The upper cervical spine is densely supplied with proprioceptors and surrounds the brainstem, which means its alignment influences muscle tone regulation and the protective guarding response throughout the neck. When the upper cervical region is misaligned, the muscles around an injured disc tend to guard more persistently, and that guarding is itself a meaningful source of the pain and stiffness people experience. If you also find yourself with a constant urge to crack or pop your neck, that often reflects this guarding pattern around a stiff, irritated segment.
Why Upper Cervical Care Matters for a Cervical Herniated Disc
At Lavender Family Chiropractic in Sarasota, our approach to a herniated disc is built on honesty about what care can and cannot do. We cannot, and do not claim to, repair a herniation or force it back into place. What we can do is support your body’s own healing process and address the mechanical environment around the injured disc. Through the Knee Chest Upper Cervical technique, we correct atlas and axis misalignment with a precise, gentle, sub-millimeter adjustment that requires no twisting, no cracking, and no forceful rotation of the neck.
This gentleness is not a minor detail; it is central to why upper cervical care is appropriate for disc patients. A cervical spine with an acute herniation is exactly the kind of neck where aggressive, high-velocity rotational manipulation is inadvisable and can aggravate the injured disc and nerve. The upper cervical approach deliberately avoids those forces. We are not manipulating the herniated level at all. We are correcting the structural foundation above it, gently, to improve how the whole cervical spine is loaded.
For someone recovering from a cervical herniation, restoring upper cervical alignment can contribute in several ways. It reduces the asymmetric loading on the injured disc and its neighbors, supporting a less mechanically hostile environment for healing. It helps normalize the proprioceptive input and muscle tone regulation that influence protective guarding, which can ease pain and stiffness. And by improving whole-neck mechanics, it may help reduce the strain patterns that contributed to the herniation in the first place, lowering the risk that an adjacent disc follows suit.
What separates upper cervical care from a generic adjustment is the precision of the diagnosis and the specificity and gentleness of the correction. We see ourselves as one part of a recovery strategy that supports the body’s own, well-documented capacity to resorb herniated disc material over time, while we help manage symptoms and mechanics along the way.
What Care Looks Like at Lavender Family Chiropractic
If you come into our Sarasota office for evaluation of a cervical herniated disc, here is what to expect.
Your first visit begins with a thorough consultation. Dr. Lavender or Dr. Temple will sit down with you and review your full history: when symptoms began, what triggered them, the exact pattern of your pain and any arm symptoms, what imaging you have had, and what you have been told. We pay particular attention to red flags. If you have signs of cervical myelopathy, spinal cord involvement, such as changes in hand coordination, balance or gait problems, or progressive or profound weakness or numbness, we will tell you directly and ensure you get prompt medical and possibly surgical evaluation. Myelopathy and rapidly progressing neurological deficits are the situations where conservative care is not enough, and screening for them is part of our responsibility. Patient safety comes before everything else.
For appropriate patients, the examination includes a detailed neurological evaluation, testing reflexes, sensation, and strength, along with postural and range-of-motion assessment and advanced 3D CBCT imaging of your cervical spine. We also review any prior MRI, which remains the best tool for visualizing the disc and any nerve or cord involvement. We perform functional nervous system scans to objectively measure how your nervous system is operating before care begins.
If the examination reveals an upper cervical misalignment relevant to your situation, we will explain our findings and recommendations openly and honestly, including a frank conversation about what upper cervical care can realistically contribute to your recovery and what it cannot. If your situation calls for medical co-management, pain management, or surgical evaluation, we will tell you plainly and help coordinate that care. We coordinate with other providers rather than pretending we are the whole answer.
For patients who are appropriate candidates, care is delivered through the gentle Knee Chest Upper Cervical technique, with no popping, twisting, or rotational force, which is particularly important with an injured disc. We offer customized treatment plans tailored to the nature and severity of your herniation, and we are transparent about realistic timelines. Given that most herniations improve substantially within weeks to a few months, our role is to support that trajectory, manage symptoms and mechanics along the way, and keep a close eye out for the minority of cases that need more.
📞 Call (941) 243-3729 to schedule your complimentary consultation 📅 Book your consultation online 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
What the Research Says About Cervical Herniated Discs and Conservative Care
The research on cervical disc herniation carries a consistent and encouraging message: most herniations improve without surgery, the body has a real capacity to resorb herniated material, and conservative care should generally come first.
On prevalence and the imaging-symptom disconnect, the Brinjikji systematic review in the American Journal of Neuroradiology is definitive, documenting that disc bulges and protrusions are extremely common in completely asymptomatic people and become more common with age, with bulges present in 84% of pain-free 80-year-olds. The practical lesson for patients is that a herniation on a scan is not, by itself, proof of the source of your pain, and it is not a sentence.
On natural history and treatment, the 2026 American Journal of Medicine review found that the majority of cervical disc herniations improve with nonsurgical care, with 80 to 85% resolving within 8 to 12 weeks, and surgery reserved for myelopathy, progressive deficits, or refractory cases. On the mechanism of healing, the Surgical Neurology Internationalreview documents that herniated cervical discs spontaneously regress through dehydration, retraction, and an inflammatory resorption process in which the immune system clears the displaced material, with larger extruded herniations often the most likely to regress.
It is worth being honest about the limits of this evidence as it applies to upper cervical care specifically. The strong evidence here is about the natural history of herniations and the value of conservative care in general; it is not evidence that upper cervical correction resorbs discs. We think it reads as more credible, not less, to state plainly that the prevalence and natural-history data are very well established, while the role of upper cervical care is best understood as supporting the body’s own healing process and addressing the mechanical environment, rather than directly repairing the disc. What the literature clearly supports is starting conservatively, giving the body time, addressing the modifiable mechanical and lifestyle factors, and reserving surgery for the minority of cases that genuinely require it.
Lifestyle Factors That Support Disc Healing
Whether or not upper cervical care is part of your plan, the daily inputs you control have a real effect on how a herniated disc recovers and whether the next one develops. Since the body’s own resorption process is doing much of the work, your job is largely to create the conditions that support it.
Avoid aggressive neck manipulation and forceful stretching during the acute phase. An acutely herniated disc is not the time for high-velocity neck cracking or aggressive stretching, which can aggravate the injured disc and nerve. The Knee Chest Upper Cervical technique deliberately avoids these forces, which is part of why it is appropriate during recovery.
Screen ergonomics. Sustained forward head posture from phones, tablets, and laptops dramatically increases the load on the lower cervical discs, the same load that contributes to herniation. Bring screens to eye level and break up long stretches of looking down. This matters both for healing the current herniation and for protecting the discs above and below it.
Stay gently active. Prolonged immobility is not the answer; gentle, pain-respecting movement supports circulation, reduces guarding, and aids healing. Walk, move within your comfortable range, and avoid only the specific movements that sharply provoke radiating symptoms.
Sleep position and pillow. A pillow that keeps your neck in neutral alignment, supporting the natural curve without pushing the head forward or letting it drop, protects the injured disc during the hours you spend in bed. Back and side sleeping with proper support are kinder than stomach sleeping, which forces prolonged rotation.
Hydration. The discs are roughly 80% water, and their health and resilience depend on staying hydrated. In the Florida heat this is especially important. Aim for at least half your body weight in ounces of water daily.
Anti-inflammatory eating. Much of the pain from a herniation comes from inflammation, and the resorption process itself is an inflammatory one that the body manages. Supporting healthy inflammation regulation with whole foods, healthy fats, omega-3-rich fish, and adequate protein, while minimizing processed foods, refined sugars, and seed oils, supports recovery.
Smoking cessation. If you smoke, this is one of the most important things you can do. Smoking impairs the already-limited blood supply that nourishes the discs and is a well-documented risk factor for disc degeneration and poorer healing.
Avoid heavy lifting and high-load activity during the acute phase. While the disc is healing, avoid heavy lifting, overhead pressing, and high-impact activity that loads the injured segment. Gradually return as symptoms settle and you are cleared.
If you found this guide useful, you may also want to read our guide on pinched nerve in the neck (cervical radiculopathy), which explains what happens when a herniated disc irritates a nerve root and produces arm symptoms, and how care addresses that downstream nerve problem.
Serving Sarasota and the Surrounding Communities
Lavender Family Chiropractic is located in Sarasota, Florida, at 5899 Whitfield Avenue, Suite 107, at the corner of University and Whitfield. From this central location, we serve patients throughout the region, including Bradenton, Lakewood Ranch, Palmetto, Parrish, Venice, Osprey, Nokomis, Ellenton, Ruskin, Myakka City, North Port, and the greater Tampa Bay area. Patients also travel from St. Pete, Riverview, and Manatee County to receive specialized upper cervical care here.
A herniated disc diagnosis is the kind of news that sends people searching urgently for answers, often fearing surgery is inevitable. For the great majority, it is not. If you want a thorough, honest evaluation of where upper cervical care fits into supporting your recovery and protecting your neck going forward, we would be glad to help.
Top 15 FAQs About Cervical Herniated Discs and Upper Cervical Chiropractic Care
1. What exactly is a herniated disc in the neck? It is when the soft inner material of a cervical disc pushes out through a weakened or torn area of the tougher outer ring. Depending on how far it goes, it may be called a bulge, protrusion, extrusion, or sequestration. It can press on a nerve and provoke inflammation, but it does not always cause symptoms.
2. Does a herniated disc on my MRI mean that is what is causing my pain? Not necessarily. Bulges and protrusions are extremely common in people with no pain at all, so imaging findings correlate imperfectly with symptoms. Your herniation is real, but whether it is the source of your pain requires correlating the imaging with your clinical examination.
3. Will my herniated disc heal on its own? Very often, yes. Research shows 80 to 85% of cervical disc herniations improve with conservative care within 8 to 12 weeks, and herniated discs frequently shrink or resorb on their own as the body clears the displaced material. Most people never need surgery.
4. Can chiropractic repair or push my disc back into place? No, and we will never claim it can. No legitimate provider can push a herniation back in. What conservative care, including gentle upper cervical care, can do is support your body’s own healing process, manage symptoms, and address the mechanical environment around the disc.
5. Then why would upper cervical care help at all? Because the alignment of the top of your neck influences how the lower cervical discs are loaded. Correcting upper cervical misalignment can reduce the chronic, uneven stress on the injured disc and its neighbors, supporting a better environment for the body’s natural healing and helping protect adjacent discs.
6. Is upper cervical chiropractic safe with an acute herniation? Yes, this is one of its advantages. The Knee Chest Upper Cervical technique is gentle and precise, with no twisting, popping, or rotational force, which makes it appropriate where aggressive manipulation of an injured disc would be inadvisable. We always examine thoroughly first.
7. What is the difference between a herniated disc and a pinched nerve? The herniation is the structural event, the disc material pushing out. A pinched nerve (cervical radiculopathy) is one possible consequence, when the herniation irritates a nerve root and causes arm symptoms. Many herniations cause only neck pain or no symptoms at all.
8. When do I actually need surgery? Surgery is generally reserved for cervical myelopathy (spinal cord involvement), progressive neurological deficits, or symptoms that remain severe and refractory after a good course of conservative care. The large majority of patients do not meet these criteria.
9. When is a herniated disc an emergency? Seek prompt medical care if you develop signs of myelopathy, changes in hand coordination, balance or gait problems, or rapidly progressing weakness or numbness. These point to spinal cord involvement and require urgent evaluation. We screen carefully for these signs.
10. How long does recovery usually take? Most cervical herniations improve substantially within 8 to 12 weeks with conservative care, though timelines vary with the size and location of the herniation and individual factors. Larger extruded herniations sometimes resorb surprisingly well over several months.
11. Can a car accident cause a herniated disc? Yes. Whiplash and other cervical trauma are well-documented causes of disc herniation, sometimes appearing immediately and sometimes developing later. Our car accident chiropractic careaddresses the whole-cervical-spine picture that trauma patients need.
12. Should I avoid certain activities while it heals? Yes. During the acute phase, avoid heavy lifting, overhead pressing, aggressive neck stretching, forceful self-cracking, and any movement that sharply provokes radiating pain. Gentle movement, walking, and pain-free range of motion are generally beneficial.
13. Does posture really affect my disc? Significantly. Sustained forward head posture from devices dramatically increases load on the lower cervical discs, contributing to herniation and potentially slowing recovery. Addressing posture and the alignment that drives it is an important, modifiable factor.
14. How will I know if upper cervical care is right for me? The only way to know for certain is a thorough evaluation. Our examination, including 3D imaging, neurological testing, and review of any MRI, will show whether an upper cervical misalignment is relevant to your situation, and we will give you an honest assessment of what upper cervical care can and cannot contribute.
15. How do I get started? Call our Sarasota office at (941) 243-3729 or book your consultation online. We will review your history, perform a thorough examination, screen for red flags including myelopathy, and give you a straight answer about how upper cervical care fits into your recovery.
Take the Next Step Toward Natural Neck Pain Relief
A cervical herniated disc sounds like a structural catastrophe, but for the great majority of people it is a condition the body is genuinely capable of healing. Most herniations improve within weeks to a few months, many of them resorb and shrink on their own, and surgery is necessary for only a minority of cases. The people who recover best are the ones who understand this, resist the fear that pushes toward unnecessary surgery, and support their body’s natural healing with conservative care, sound mechanics, and attention to the daily factors that either help or hinder.
If you are in Sarasota, Bradenton, Lakewood Ranch, or anywhere in the surrounding region and you have been told you have a herniated disc in your neck, Dr. Rusty Lavender and Dr. Jacob Temple at Lavender Family Chiropractic are here to give you an honest evaluation of where upper cervical care fits into supporting your recovery, natural neck pain treatment focused on helping your body do what it is already designed to do.
📞 Call (941) 243-3729 today to schedule your complimentary consultation 📅 Book online here 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
Related Articles
Related Posts
Popular Posts