By Dr. Rusty Lavender
Hormones and Vertigo: Many women notice that their dizziness is not random. It shows up in the days before a period, deepens during pregnancy, or arrives for the first time in the run-up to menopause. If your vertigo seems to track with your hormones, you are not imagining it — the balance system and the endocrine system are more closely linked than most people realize, and shifts in estrogen in particular can change how steady you feel.
This article explains how hormonal changes across a woman’s life can influence vertigo, why conditions like BPPV become more common around menopause, how to tell ordinary hormonal dizziness from causes that need medical attention, and where upper cervical chiropractic care may fit for the right person. At Lavender Family Chiropractic in Sarasota, we help women sort out the moving parts behind their dizziness so they can find steadier ground.
Hormones and Vertigo: How Hormones and the Balance System Are Connected
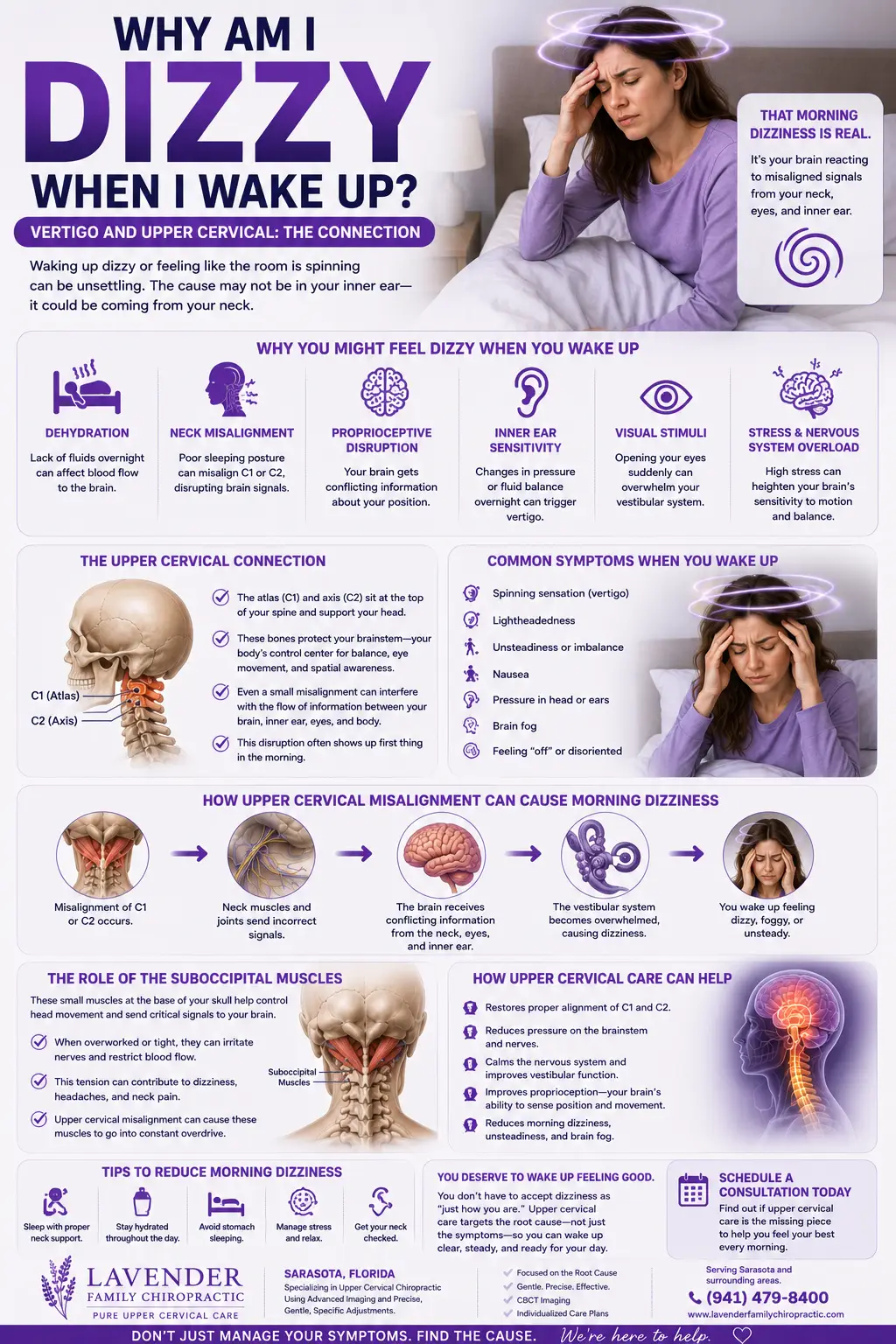
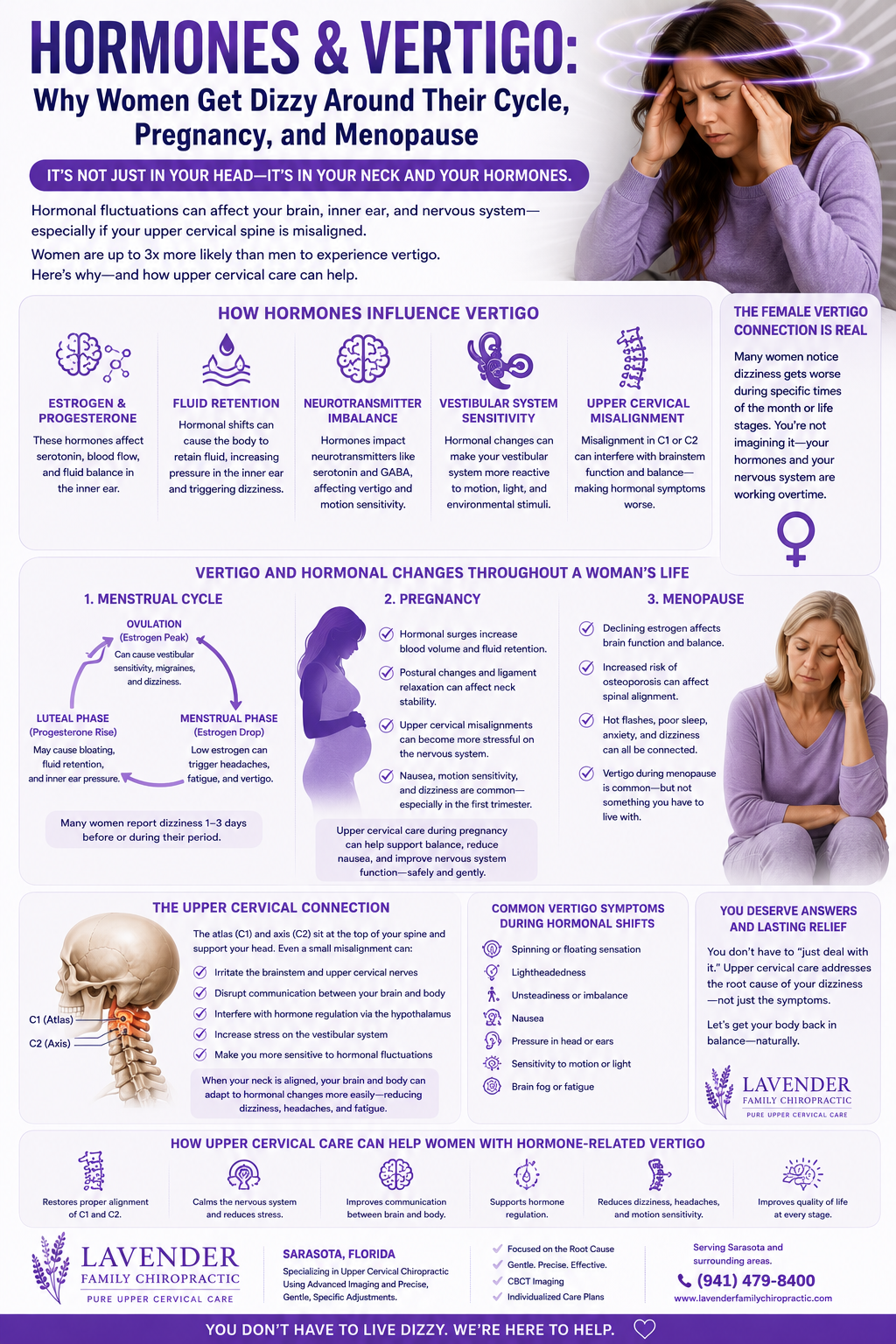
Your sense of balance depends on the inner ear, the eyes, and the position sensors in your neck, all integrated by the brain. Estrogen influences several links in that chain. Receptors for estrogen are found in inner-ear tissue, and the hormone affects fluid balance, blood flow, and how nerve signals are processed. When estrogen rises and falls — as it does across the menstrual cycle, in pregnancy, and through the menopausal transition — the inner ear and the circulatory system it depends on can become more reactive, and dizziness can surface.
Estrogen also affects blood pressure regulation and fluid retention, both of which feed into how steady you feel. And because the hormone plays a role in bone and calcium metabolism, its decline around menopause has been linked to changes in the tiny calcium crystals of the inner ear — a connection that helps explain why positional vertigo becomes more common in midlife women. None of this means hormones are the whole story, but for many women they are a meaningful part of it.
Vertigo Across the Phases of a Woman’s Life
The menstrual cycle. Some women experience dizziness in the days before menstruation, when estrogen drops sharply. This premenstrual dizziness can travel with the headaches, fluid shifts, and fatigue of the premenstrual phase, and for women prone to migraine it can overlap with vestibular migraine, in which the balance system is drawn into the migraine process.
Pregnancy. Dizziness is common in pregnancy, especially early on. Blood-vessel changes, shifts in blood pressure, a growing demand on blood volume, and occasional low blood sugar all contribute. Most pregnancy-related dizziness is benign, but it should always be discussed with your obstetric provider, particularly if it is severe or comes with other symptoms.
Perimenopause and menopause. This is the phase when many women first notice significant vertigo. As estrogen declines and fluctuates, the inner ear and circulatory system become more reactive, and the risk of benign paroxysmal positional vertigo (BPPV) rises. Hot flashes, disrupted sleep, migraine changes, and blood-pressure shifts can all layer on top of one another, making midlife dizziness feel especially complicated.
BPPV, Estrogen, and Bone Metabolism
Benign paroxysmal positional vertigo — the brief, intense spinning triggered by head movement — is the most common cause of vertigo overall, and it disproportionately affects women, especially after menopause. The leading explanation involves the otoconia, the tiny calcium-carbonate crystals in the inner ear that normally help you sense gravity. When these crystals become dislodged and drift into a semicircular canal, they generate false spinning signals with certain head positions.
Estrogen supports calcium and bone metabolism, and its decline around menopause is associated with lower bone density and changes in calcium handling. Researchers have proposed that these same metabolic shifts may make the otoconia more fragile or more prone to becoming dislodged, which would help explain why BPPV climbs in postmenopausal women. The overlap between osteoporosis and BPPV in this population supports the idea that bone and inner-ear calcium metabolism are linked. This is an area of active research rather than settled fact, but it offers a plausible reason why so many women meet positional vertigo for the first time in midlife.
When Hormonal Dizziness Is a Red Flag
Most hormone-associated dizziness is benign, but some patterns need prompt medical evaluation regardless of where you are in your cycle or life stage. Seek urgent care if dizziness comes with slurred speech, double or lost vision, weakness or numbness on one side, a severe or unusual headache, trouble swallowing, fainting, chest pain, or a fast or irregular heartbeat. Dizziness that is constant rather than tied to movement, that steadily worsens, or that arrives with new one-sided hearing loss also warrants a medical workup. In pregnancy, always report significant or persistent dizziness to your obstetric provider. Being honest about these possibilities comes first; upper cervical chiropractic care is appropriate only once serious causes have been ruled out. If you are unsure whether your symptoms warrant imaging, our overview of when to get an MRI for dizziness can help you think it through.
The Upper Neck: The Piece That Often Gets Missed
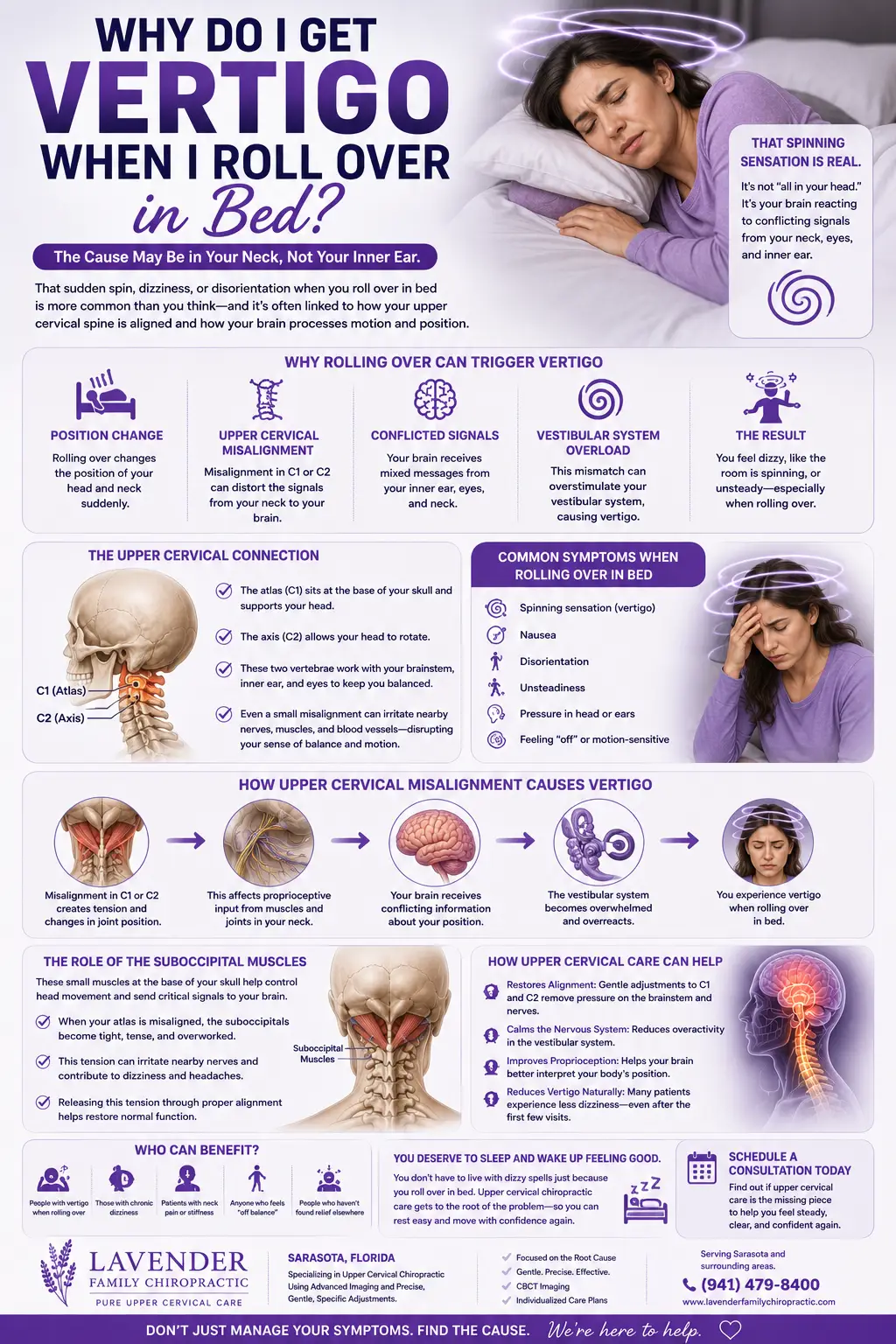
Hormones get most of the attention in conversations about women’s dizziness, but there is a contributor that is easy to overlook: the upper neck. The top two vertebrae, the atlas and axis, are densely packed with position sensors that tell the brain where your head is. The brain blends those neck signals with input from the inner ears and eyes to build a stable sense of balance. When the neck is misaligned, it sends distorted signals, and the brain has to reconcile that distortion — a mismatch felt as dizziness or unsteadiness. Research on cervicogenic dizziness describes how disturbed neck proprioception can produce these symptoms even when the inner ear is structurally normal.
Here is why this matters for hormonal vertigo. When estrogen shifts have already made the inner ear more reactive, an unreliable neck signal on top of that gives the balance system even less solid ground to stand on. Two modest problems can combine into a noticeable one. Addressing the neck does not change your hormones, but it can remove one of the inputs that is compounding the dizziness — which is why some women who have chased hormonal explanations for years find that the neck was quietly part of the picture. Our article on whether neck pain can cause dizziness explores this connection in more depth.
How Upper Cervical Chiropractic Care May Help
Upper cervical chiropractic focuses specifically on the alignment of the atlas and axis and their influence on the nervous system. If a misalignment in the upper neck is feeding the brain unreliable position information, correcting it may allow the balance system to receive cleaner signals — and that can matter most when hormonal changes have already made the system more reactive.
At Lavender Family Chiropractic, we practice a precise, gentle approach called the Knee Chest Upper Cervical technique. It uses a specific, low-force correction rather than the twisting or cracking many people associate with chiropractic. Before any correction, we map your alignment with 3D CBCT imaging and evaluate nervous-system function with paraspinal infrared thermography, so our care is guided by objective findings.
It is important to be candid: upper cervical care does not adjust your hormones and does not reposition inner-ear crystals — the repositioning maneuvers that treat BPPV do that. What it addresses is a different, frequently overlooked contributor: the neck’s role in balance. For many women, hormonal vertigo has more than one cause, and the neck is one piece worth evaluating. You can learn more about our overall approach on our upper cervical chiropractic care page.
If your dizziness seems to track with your cycle, pregnancy, or the menopausal transition, call Lavender Family Chiropractic at (941) 243-3729 to talk through whether an upper cervical evaluation makes sense for you.
What the Research Says
Research increasingly recognizes the connection between hormonal changes and vertigo in women.
A study examining risk factors for positional vertigo found associations between BPPV and perimenopausal status in women, reinforcing that the menopausal transition is a period of heightened vulnerability to positional dizziness.
A review titled Balance in Transition explores the relationship between menopause, estrogen, and vestibular symptoms, summarizing how declining estrogen may influence the inner ear and balance during midlife.
Research from a large population study found that estrogen replacement was associated with reduced age-related BPPV, supporting a link between estrogen and inner-ear positional vertigo.
A further study examined BPPV recurrence in postmenopausal women, adding to the evidence that hormonal status influences the course of positional vertigo.
Finally, research on proprioceptive cervicogenic dizziness describes how disturbed neck input can generate dizziness and unsteadiness, supporting the rationale for evaluating the upper neck when balance feels off.
Practical Steps That Support Steadier Balance
Alongside professional care, several habits can help you weather hormonal shifts with less dizziness.
Track the timing. Noting when your dizziness appears relative to your cycle or other hormonal changes helps both you and your providers see the pattern and target the right contributors.
Stay well hydrated. Fluid balance affects both the inner ear and blood pressure, and hormonal shifts can amplify swings in both. Steady hydration matters year-round in Florida’s heat.
Support blood sugar and sleep. Regular meals steady blood sugar, and consistent sleep calms a nervous system that hormonal changes can already leave on edge — both raise your threshold for dizziness.
Mind your pillow and neck posture. Support that keeps the neck near neutral gives the upper-neck position sensors a calmer baseline, which is worth attending to when the balance system is already more reactive.
Rise and turn gradually. Slow, deliberate position changes give the inner ear, circulation, and neck time to update together, reducing the intensity of episodes.
Loop in your medical team. For cycle-, pregnancy-, or menopause-related symptoms, your gynecologic or obstetric provider is an essential partner. Upper cervical care works best alongside, not instead of, appropriate medical care.
Sorting Hormonal Dizziness From Everything Else
One of the challenges of hormone-related vertigo is that it rarely arrives alone. Around the cycle, in pregnancy, and especially through menopause, dizziness often shows up alongside fatigue, headaches, sleep trouble, and mood changes — and it can be hard to tell what is driving what. Paying attention to a few patterns helps you and your providers untangle the threads.
Does it track with your hormones or with movement? If your dizziness clusters in the days before your period, deepens in pregnancy, or emerged as you entered the menopausal transition, a hormonal influence is likely part of the picture. If instead it fires with a specific head movement — rolling over, tipping your head back — that points toward inner-ear positional vertigo, which itself becomes more common as estrogen declines. Often both are true at once.
Does it spin or does it sway? True rotational spinning points toward the inner ear. A floating, off-balance, or top-heavy sensation without vivid rotation is more suggestive of a blood-pressure pattern or a neck contribution. Naming the quality of your dizziness is one of the most useful things you can do before an appointment.
What travels with it? Note whether your dizziness comes bundled with migraine or headache, ear fullness or ringing, hot flashes, a stiff and achy upper neck, or tension at the base of the skull. Vestibular migraine, Meniere’s-type symptoms, and cervical contributions each leave different fingerprints, and the company your dizziness keeps helps identify the source.
Has it changed with a life-stage shift? Dizziness that began or worsened as you entered perimenopause, started a new medication, or changed hormonal contraception is worth flagging, because the timing itself is a clue.
Keeping a simple log — where you are in your cycle or life stage, whether it spun or swayed, how long it lasted, and what came with it — turns a confusing, multi-layered experience into information your medical team and ours can actually use. Because hormonal vertigo so often has several contributors, this kind of pattern-spotting is where clarity usually begins.
What to Expect at Your First Visit
If dizziness has left you cautious, knowing what a first visit involves can make the decision to come in easier.
We begin with an unhurried conversation about your history, including how your dizziness relates to your cycle, pregnancy, or menopausal transition. We want to understand whether it truly spins or simply sways, how long it lasts, what triggers it, and what else comes with it. These details help us separate inner-ear positional vertigo and vestibular migraine from a cervical contribution or a red-flag pattern that belongs in a medical setting.
Next, we gather objective data. The 3D CBCT imaging shows us the precise position of your atlas and axis, and paraspinal infrared thermography helps us assess nervous-system function. Together they guide whether an upper cervical correction is appropriate or whether we should refer you for further evaluation first.
If care is indicated, we explain our findings in plain language and outline a customized treatment plan built around your goals. We practice on a cash-pay basis and review the details with you in advance. We will always be clear about where upper cervical care fits and where medical or gynecologic care belongs. If you would like to talk anything through before scheduling, call us any time at (941) 243-3729.
Areas We Serve Around Sarasota
Lavender Family Chiropractic is located at 5899 Whitfield Avenue, Suite 107, in Sarasota, at the corner of University and Whitfield. We care for women seeking natural vertigo relief from across the region, including Bradenton, Lakewood Ranch, Palmetto, Ellenton, Ruskin, Venice, Osprey, Myakka, Tampa, and St. Pete.
Top 15 Frequently Asked Questions About Hormonal Vertigo in Women
1. Can hormones really cause vertigo? Yes. Estrogen influences the inner ear, fluid balance, blood pressure, and calcium metabolism, so its rise and fall across the cycle, pregnancy, and menopause can affect how steady you feel.
2. Why do I get dizzy before my period? The sharp drop in estrogen in the days before menstruation can affect the inner ear and circulation, and for migraine-prone women it can overlap with vestibular migraine.
3. Is dizziness normal in pregnancy? Mild dizziness is common, especially early on, due to blood-vessel and blood-pressure changes and occasional low blood sugar. Always report significant or persistent dizziness to your obstetric provider.
4. Why did my vertigo start around menopause? Declining estrogen makes the inner ear and circulation more reactive and is linked to changes in inner-ear calcium crystals, which is why BPPV rises in postmenopausal women.
5. What is BPPV? Benign paroxysmal positional vertigo is brief, intense spinning triggered by head movement, caused by loose calcium crystals (otoconia) drifting into a semicircular canal.
6. Why is BPPV more common in women? Women, especially after menopause, develop BPPV more often than men. The leading explanation involves estrogen’s role in calcium and bone metabolism affecting the inner-ear crystals.
7. Can a chiropractor fix the inner-ear crystals? No. Repositioning maneuvers, not chiropractic adjustments, move the crystals. Upper cervical care addresses a different contributor — the neck’s position signals — and can be part of a coordinated approach.
8. How does my neck fit in if this is hormonal? The upper neck supplies a large share of your head-position sense. When hormones have already made the inner ear reactive, an unreliable neck signal on top of that can tip you into noticeable dizziness.
9. Is hormonal vertigo dangerous? Usually not, but dizziness with slurred speech, double vision, one-sided weakness or numbness, a severe headache, fainting, or chest pain is a red flag that warrants urgent care.
10. Will hormone therapy help my vertigo? Some research links estrogen replacement with reduced age-related BPPV, but hormone therapy is a decision for you and your physician based on your full health picture. It is not something we prescribe.
11. What testing do you perform? We use 3D CBCT imaging to assess upper cervical alignment and paraspinal infrared thermography to evaluate nervous-system function, alongside a history and screening to help distinguish cervical from inner-ear and other causes.
12. Can stress and poor sleep make it worse? Yes. Hormonal transitions often disrupt sleep and raise stress, and a nervous system on high alert heightens the perception of dizziness.
13. Does hydration matter? Yes. Fluid balance affects both the inner ear and blood pressure, both of which hormonal shifts can amplify. Steady hydration helps year-round in Florida’s heat.
14. Should I see my gynecologist too? For cycle-, pregnancy-, or menopause-related symptoms, yes. Upper cervical care works best alongside appropriate medical and gynecologic care, not instead of it.
15. Where are you located and who do you serve? We are at 5899 Whitfield Avenue, Suite 107, in Sarasota, serving patients from Bradenton, Lakewood Ranch, Venice, Palmetto, Ellenton, and the surrounding area.
Ready to Understand What’s Behind Your Dizziness?
If your vertigo seems tied to your hormones, understanding whether your inner ear, your circulation, your upper neck, or some combination is involved is the first step toward steadier ground. If you are ready to find out, call Lavender Family Chiropractic at (941) 243-3729 or book your consultation online at https://intake.chirohd.com/new-patient-scheduling/724/lavender-family-chiropractic. Our Sarasota team is here to help you pursue natural vertigo relief as part of a comprehensive plan.