By Dr. Rusty Lavender
Why Do I Get Vertigo When I Roll Over in Bed? You turn onto your side in the middle of the night, and suddenly the whole room is spinning. It lasts only a few seconds, but it is violent enough to jolt you awake, grip the mattress, and lie perfectly still until it fades. Maybe it happens again when you lie back down, or when you sit up in the morning. If rolling over in bed reliably sets off a wave of spinning, you are describing one of the most recognizable patterns in all of balance medicine — and it points squarely at the inner ear and the upper neck.
At Lavender Family Chiropractic in Sarasota, “the room spins when I roll over” is one of the most common stories we hear from people searching for natural vertigo relief. The specific trigger — a change in head position while lying down — is a meaningful clue. This guide explains what actually happens in your inner ear when you roll over, why the upper neck is part of the picture, when this pattern needs medical evaluation, and how upper cervical chiropractic care may fit into a comprehensive plan.
Why Do I Get Vertigo When I Roll Over in Bed? First, the Most Common Cause: BPPV
When vertigo is triggered specifically by rolling over, lying down, or sitting up, the leading suspect is benign paroxysmal positional vertigo, or BPPV. It is the single most common cause of position-triggered spinning, and understanding it is the starting point.
Deep in your inner ear are tiny crystals of calcium carbonate called otoconia. Normally they sit in a gel-like membrane where they help you sense gravity and linear motion. In BPPV, some of these crystals break loose and drift into one of the fluid-filled semicircular canals — the loops that detect rotation. When you change head position, gravity pulls the loose crystals through the canal fluid, which bends the sensory hairs and sends the brain a sudden, intense signal that you are spinning, even though you are not.
That is why the vertigo is so tied to movement and so brief. Roll onto your side and the crystals shift; the canal fires; the room spins for a few seconds to under a minute; then the crystals settle and it stops — until the next position change. The two canals most often involved are the posterior canal (classically triggered by tipping the head back or lying down) and the horizontal canal (classically triggered by rolling from side to side while lying flat). Rolling over in bed is a textbook trigger for both.
The reassuring part is right there in the name: BPPV is benign. It is not dangerous in itself, and it is typically identified with a specific positional test and addressed with a repositioning maneuver that guides the crystals back where they belong. Our guide on whether vertigo and motion sickness are the same thing can help you sort out how positional vertigo differs from other dizzy sensations.
When Rolling-Over Vertigo Needs Medical Attention
Before going further, an honest word about safety. The overwhelming majority of rolling-over vertigo is benign positional vertigo. But certain features are red flags that call for prompt medical evaluation rather than a chiropractic appointment.
Seek urgent care if your dizziness comes with slurred speech, double vision, weakness or numbness on one side, difficulty swallowing, a severe or unusual headache, trouble walking that persists between episodes, or loss of consciousness. Vertigo that is constant rather than brief and positional, or that is accompanied by new hearing loss or ringing in one ear, also deserves a medical workup. These patterns can point to inner-ear, neurological, or circulatory conditions that need to be ruled out first. Our article on when to get an MRI for dizziness walks through when imaging and further evaluation make sense. A careful evaluation is what separates simple positional vertigo from something that needs a different kind of care.
Where the Upper Neck Comes In
If BPPV is an inner-ear problem, why does an upper cervical chiropractor have anything to offer? The answer lies in how your brain builds a sense of balance, and in a second, often-overlooked source of positional dizziness.
Your sense of stability depends on three information streams agreeing: the inner ear, which senses head motion and gravity; the eyes, which report what is moving around you; and the neck and body, which report the position of your head relative to your torso. The brain fuses these three inputs into one steady picture. When they disagree, you feel dizzy.
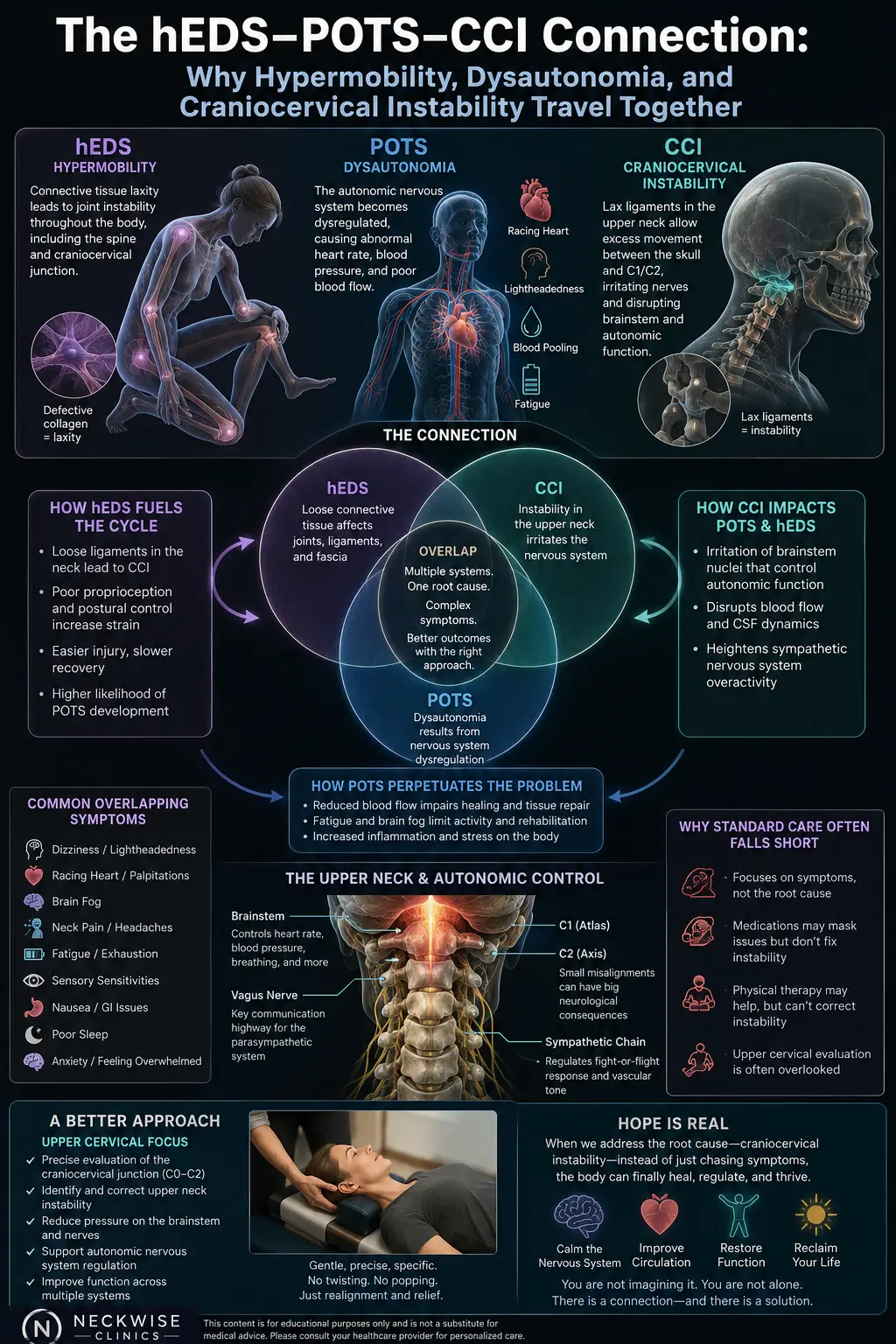
The upper cervical spine — the atlas (C1) and axis (C2) at the very top of the neck — carries a remarkable share of that job. This small region sits just below the brainstem and holds one of the densest concentrations of position-sensing receptors in the body; roughly half of the neck’s proprioceptors for head orientation are clustered here. When you roll over, these receptors are supposed to tell the brain exactly how your head moved. If the upper neck is misaligned or chronically tense, the signal they send becomes inaccurate — and that faulty neck input can create or worsen a sense of dizziness on its own, a pattern known as cervicogenic dizziness.
There is also an interaction worth understanding. When the inner ear is already sending confusing signals — as in BPPV — a neck that is also feeding the brain unreliable position data gives the balance system even less solid ground to stand on. Some people find that lingering unsteadiness between the brief spinning episodes tracks more with the neck than with the crystals. Our article on whether neck pain can cause dizziness explores this connection in more depth.
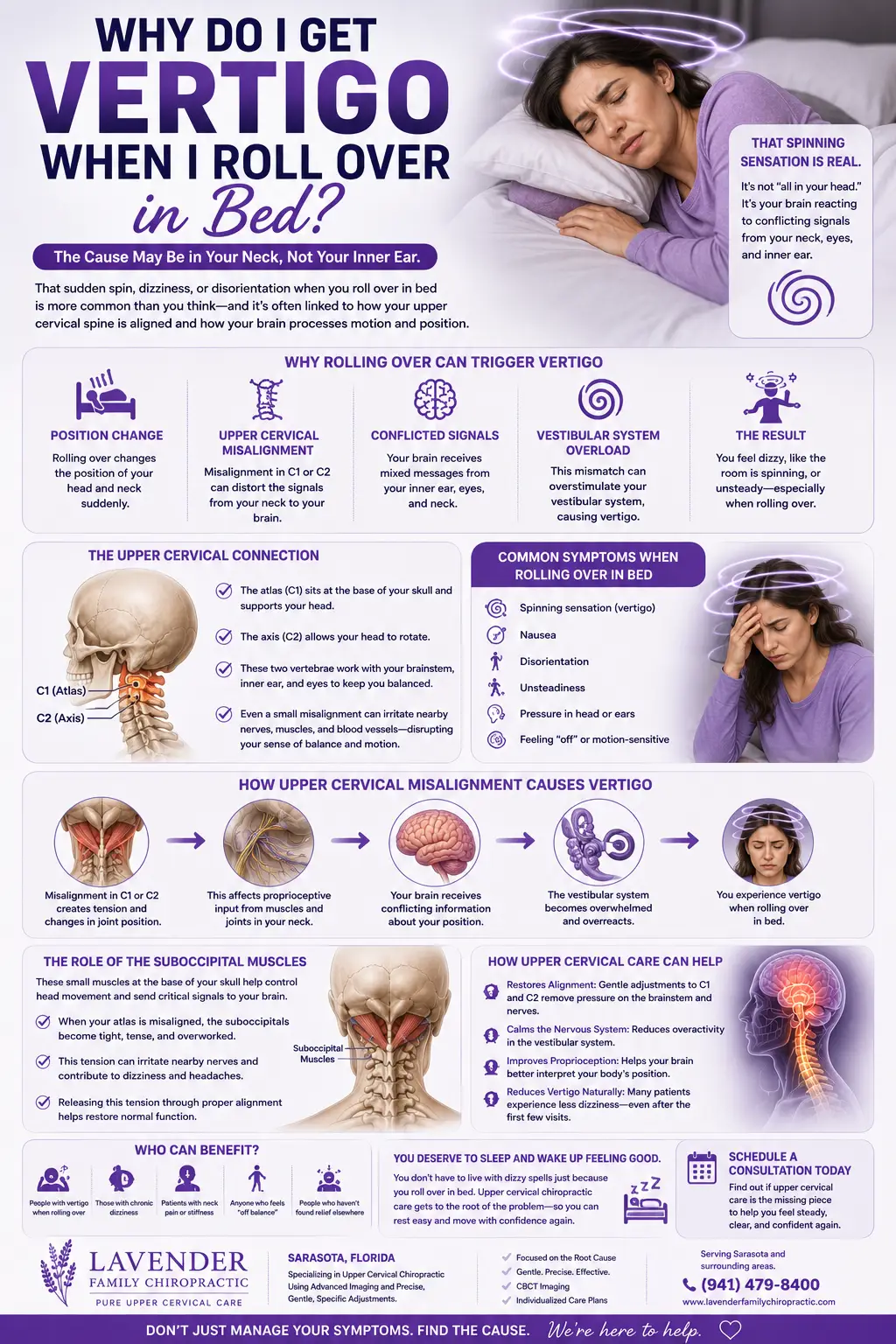
Why Rolling Over Specifically Triggers It
Rolling over in bed is such a reliable trigger because of the exact combination of motions it involves.
It changes head orientation relative to gravity. Turning from your back to your side rotates the head into a new position, and in BPPV that is precisely the movement that sends loose crystals sliding through a canal.
It happens quickly and often without visual reference. In the dark, with your eyes closed or unfocused, the brain leans even more heavily on the inner ear and neck to know where your head is. If either of those inputs is faulty, the mismatch is sharper.
It loads the upper neck. Turning your head on the pillow moves the atlanto-occipital and atlanto-axial joints — the same joints most affected by an upper cervical misalignment. In a guarded, misaligned neck, that movement adds a distorted proprioceptive signal on top of whatever the inner ear is doing.
It repeats. Because we shift position many times a night, the trigger recurs, which is why rolling-over vertigo so often disrupts sleep and leaves people anxious about lying down at all.
Put together, rolling over is almost a perfect provocation: a rapid change in head position, with little visual input, loading both the inner ear and the upper neck at once.
Upper Cervical Care at Lavender Family Chiropractic
At Lavender Family Chiropractic in Sarasota, we take a root-cause approach to dizziness rather than simply chasing the symptom. When rolling over triggers your vertigo, our first job is careful evaluation — helping distinguish inner-ear BPPV, which is addressed with repositioning maneuvers, from a cervical contribution or a red-flag pattern that belongs in a medical setting.
Our evaluation is detailed and individualized. We use 3D CBCT imaging to precisely assess the position of your atlas and axis, and paraspinal infrared thermography to evaluate how your nervous system is functioning. Because the upper neck contributes so heavily to head-position sense, this objective look at alignment and nervous-system function is especially valuable when positional dizziness lingers or keeps returning.
When a correction is indicated, we use the Knee Chest Upper Cervical technique to restore upper cervical alignment gently and precisely, without forceful twisting or cracking. The goal is to help the upper neck send accurate position signals to the balance centers, so that changing position no longer produces an unnecessary sensory mismatch. From there we develop customized treatment plans built around your specific goals.
We are also clear about scope. Upper cervical care addresses the cervical contributors to dizziness; it is not a treatment for the loose crystals of BPPV, which respond to repositioning maneuvers, and it is not a substitute for medical evaluation when red-flag symptoms are present. For many people, the most effective path is a coordinated one, and we are glad to work alongside your other providers.
Take the First Step Toward Steadier Nights
If rolling over in bed has turned sleep into something you approach with dread, we would like to help you understand the physical side of the picture. Call Lavender Family Chiropractic at (941) 243-3729 to schedule a consultation, or book online here: https://intake.chirohd.com/new-patient-scheduling/724/lavender-family-chiropractic. We will examine your upper cervical spine and help determine whether it may be contributing to your symptoms.
What the Research Says About Positional Vertigo When Rolling Over
Positional vertigo is one of the most thoroughly studied balance conditions. Here are five studies that illuminate the mechanisms behind rolling-over vertigo.
A comprehensive review of benign paroxysmal positional vertigo explains how loose otoconial crystals in the semicircular canals produce brief, position-triggered spinning, and why changes in head position — including rolling over in bed — are the hallmark provocation. It establishes the mechanical basis for the pattern most people describe.
Research on the management of lateral semicircular canal BPPV focuses on the horizontal-canal form of positional vertigo, which is classically brought on by turning from side to side while lying down. This directly addresses the rolling-in-bed trigger and how clinicians identify and reposition crystals in that canal.
A study on the supine roll test in horizontal semicircular canal BPPV examined the specific eye-movement patterns produced when the head is rolled to each side while lying flat. It shows how carefully the direction and intensity of the response are used to pinpoint which ear and canal are involved — the very movement that provokes symptoms in bed.
Research on vertical position tests for posterior canal BPPV illustrates how tipping the head back and lying down are used to provoke and diagnose the most common form of positional vertigo. This underscores that both lying down and rolling over are classic, well-documented triggers of inner-ear positional vertigo.
Finally, connecting the neck to the picture, a review of cervicogenic dizziness explains how dysfunction in the upper cervical spine can generate dizziness through faulty proprioceptive input to the balance centers. This is relevant because the upper neck helps report head position during every roll and turn, and an inaccurate neck signal can add to the unsteadiness.
Lifestyle Strategies to Ease Rolling-Over Vertigo
Alongside professional care, a few habits can make nights easier while the underlying cause is addressed.
Move slowly through position changes. When you turn over or sit up, do it deliberately rather than quickly. Giving the balance system a moment to update reduces the intensity of an episode.
Sit up in stages in the morning. Rather than springing upright, roll to your side, pause, then push up to sitting and rest a moment before standing. This is gentler on both the inner ear and blood pressure.
Reconsider your pillow and sleep posture. A pillow that props the neck into an awkward angle can aggravate both the inner ear and the upper neck. Support that keeps the neck closer to neutral is generally preferable; our guide on the best pillow for vertigo covers this in detail.
Keep a small light within reach. A dim, easy-to-reach light gives your eyes a reference point when you wake, which can lessen the mismatch that fuels nighttime spinning.
Release upper-neck tension. Gentle mobility within a comfortable range, warm compresses at the base of the skull, and awareness of jaw and neck clenching can reduce the muscle guarding that distorts position signals.
Support the basics. Adequate hydration — which matters year-round in Florida’s heat — steady sleep, and stress management all raise your threshold for dizziness and help the nervous system stay calmer.
Telling Inner-Ear and Cervical Vertigo Apart at Night
Because rolling over can provoke both inner-ear positional vertigo and a neck-driven form of dizziness, it helps to know the patterns that distinguish them. No single feature is proof on its own, but together they point toward the likely source and guide the right next step.
True spinning versus a floating sway. Classic BPPV produces a strong sense that the room is rotating. Cervical dizziness more often feels like unsteadiness, floating, or a sense that your head is disconnected from your body, without the vivid rotation. If you would describe your experience as swaying rather than spinning, the neck is more likely to be involved.
How the episode starts and stops. BPPV comes on within a second or two of a specific head movement, peaks quickly, and fades within a minute if you hold still. Cervical dizziness tends to build more gradually, track with neck stiffness and posture, and linger longer after you settle. Timing the arc of your episodes is one of the most useful things you can note before an appointment.
What else moves with it. Positional inner-ear vertigo usually travels alone, or with nausea. A neck contribution frequently comes bundled with a stiff or achy upper neck, tension headaches at the base of the skull, and a history of whiplash, a fall, or long hours at a screen. When dizziness and neck symptoms rise and fall together, that pattern is worth taking seriously.
Whether repositioning holds. If a repositioning maneuver clears your spinning but the unsteadiness keeps drifting back over the following days, an underlying neck contribution may be keeping the balance system on edge. This is a common reason people feel they are “almost better” yet never fully steady, and it is exactly the situation upper cervical care is designed to address.
Keeping a brief log — what you were doing, which direction you turned, how long it lasted, and what came with it — turns a confusing nightly experience into information we can actually use. You can read more about how the neck feeds into these symptoms in our overview of whether neck pain can cause dizziness.
What to Expect at Your First Visit
If rolling-over vertigo has made you wary, it helps to know exactly what your first visit involves so there are no surprises.
We start with an unhurried conversation about your history. We want to understand exactly which movements set off your spinning, how long each episode lasts, whether it truly spins or simply sways, and what other symptoms accompany it. These details help us distinguish inner-ear positional vertigo from a cervical contribution or a red-flag pattern that belongs in a medical setting — an important first step, because the right answer guides everything that follows.
Next, we gather objective data. The 3D CBCT imaging shows us the precise position of your atlas and axis, while paraspinal infrared thermography helps us evaluate nervous-system function. These findings guide whether an upper cervical correction is appropriate, or whether we should refer you for further evaluation first.
If care is indicated, we explain what we found in clear terms and outline a customized treatment plan built around your goals. We practice on a cash-pay basis and review the details with you in advance. We will always be candid about where upper cervical care fits and where inner-ear repositioning or medical evaluation belongs. If you would like to talk through anything before scheduling, call us any time at (941) 243-3729.
Areas We Serve Around Sarasota
Lavender Family Chiropractic is located at 5899 Whitfield Avenue, Suite 107, in Sarasota, at the corner of University and Whitfield. We care for patients seeking natural vertigo relief from throughout the region, including Bradenton, Lakewood Ranch, Palmetto, Ellenton, Ruskin, Venice, Osprey, Myakka, Tampa, and St. Pete. If nighttime vertigo has left you anxious about travel, tell us when you call and we will help you plan a comfortable first visit.
Top 15 Frequently Asked Questions About Vertigo When Rolling Over in Bed
1. Why does the room spin when I roll over in bed? The most common reason is BPPV — loose calcium crystals in the inner ear that shift when you change head position, sending a brief, intense spinning signal. Rolling over is a classic trigger. An unreliable upper-neck position signal can add to the unsteadiness.
2. How long should the spinning last? Positional vertigo from BPPV is brief — usually seconds to under a minute — and settles when you hold still. Vertigo that is constant, rather than brief and tied to movement, deserves a medical evaluation.
3. Is this dangerous? BPPV itself is benign. However, dizziness with slurred speech, double vision, weakness, numbness, trouble swallowing, a severe headache, or new one-sided hearing loss is a red flag that warrants urgent medical care.
4. What are the crystals everyone mentions? They are otoconia — tiny calcium-carbonate crystals that normally help you sense gravity. In BPPV they drift into a semicircular canal and trigger false spinning signals when your head moves.
5. Why does it happen more on one side? BPPV usually affects one ear and one canal, so rolling toward the affected side often provokes the strongest response. Identifying which side is involved guides the repositioning maneuver.
6. Can a chiropractor fix BPPV crystals? Repositioning maneuvers, not chiropractic adjustments, are what move the crystals. Upper cervical care addresses a different contributor — the neck’s position signals — and can be part of a coordinated approach, especially when unsteadiness lingers between episodes.
7. How does my neck play a role if this is an inner-ear problem? The upper neck supplies a large share of your head-position sense. If it is misaligned, it sends faulty signals that can add to dizziness, and it can leave the balance system less stable while the inner ear is also misbehaving.
8. Why does it wake me up at night? We shift position many times while sleeping, so the trigger recurs whenever the head turns into a provoking position. That is why rolling-over vertigo so often disrupts sleep.
9. Should I sleep propped up? Some people find that sleeping slightly elevated reduces episodes, but a pillow that forces the neck into an awkward angle can aggravate symptoms. Support that keeps the neck near neutral is generally best.
10. Will it go away on its own? BPPV sometimes settles over days to weeks as crystals reabsorb, but it commonly recurs. Proper diagnosis and repositioning tend to clear episodes faster, and addressing neck contributors can help with lingering unsteadiness.
11. What testing do you perform? We use 3D CBCT imaging to assess upper cervical alignment and paraspinal infrared thermography to evaluate nervous-system function, alongside a history and screening to help distinguish cervical from inner-ear and other causes.
12. Can anxiety make it worse? Yes. The fear of triggering another episode keeps the nervous system on high alert, which can heighten the perception of dizziness and lead to guarded, tense movement that adds its own strain.
13. Does dehydration matter? Staying well hydrated supports inner-ear fluid balance and blood pressure, both of which affect dizziness. In Florida’s heat, hydration matters year-round.
14. How soon might I feel steadier? It varies with the cause. Inner-ear positional vertigo often improves quickly with repositioning, while cervical contributions are addressed gradually over a plan of care.
15. Where are you located and who do you serve? We are at 5899 Whitfield Avenue, Suite 107, in Sarasota, serving patients from Bradenton, Lakewood Ranch, Venice, Palmetto, Ellenton, and the surrounding area.
Ready to Sleep Without the Spin?
When rolling over triggers your vertigo, understanding whether your inner ear, your upper neck, or both are involved is the key to steadier nights. If you are ready to find out, call Lavender Family Chiropractic at (941) 243-3729 or book your consultation online at https://intake.chirohd.com/new-patient-scheduling/724/lavender-family-chiropractic. Our Sarasota team is here to help you pursue natural vertigo relief as part of a comprehensive plan.