By Dr. Rusty Lavender – Lavender Family Chiropractic, Sarasota, FL
Living with the hypermobile type of Ehlers-Danlos syndrome (hEDS) often means living with a body that feels a little too flexible in all the wrong places. Joints slip and shift, connective tissue stretches farther than it should, and the everyday work of holding your body together can feel like a full-time job. For many people with hEDS and related hypermobility spectrum disorders, the challenges do not stop at the shoulders, hips, and fingers. Some of the most confusing and life-altering symptoms trace back to a small but critically important region at the very top of the spine: the craniocervical junction, where the skull meets the upper neck.
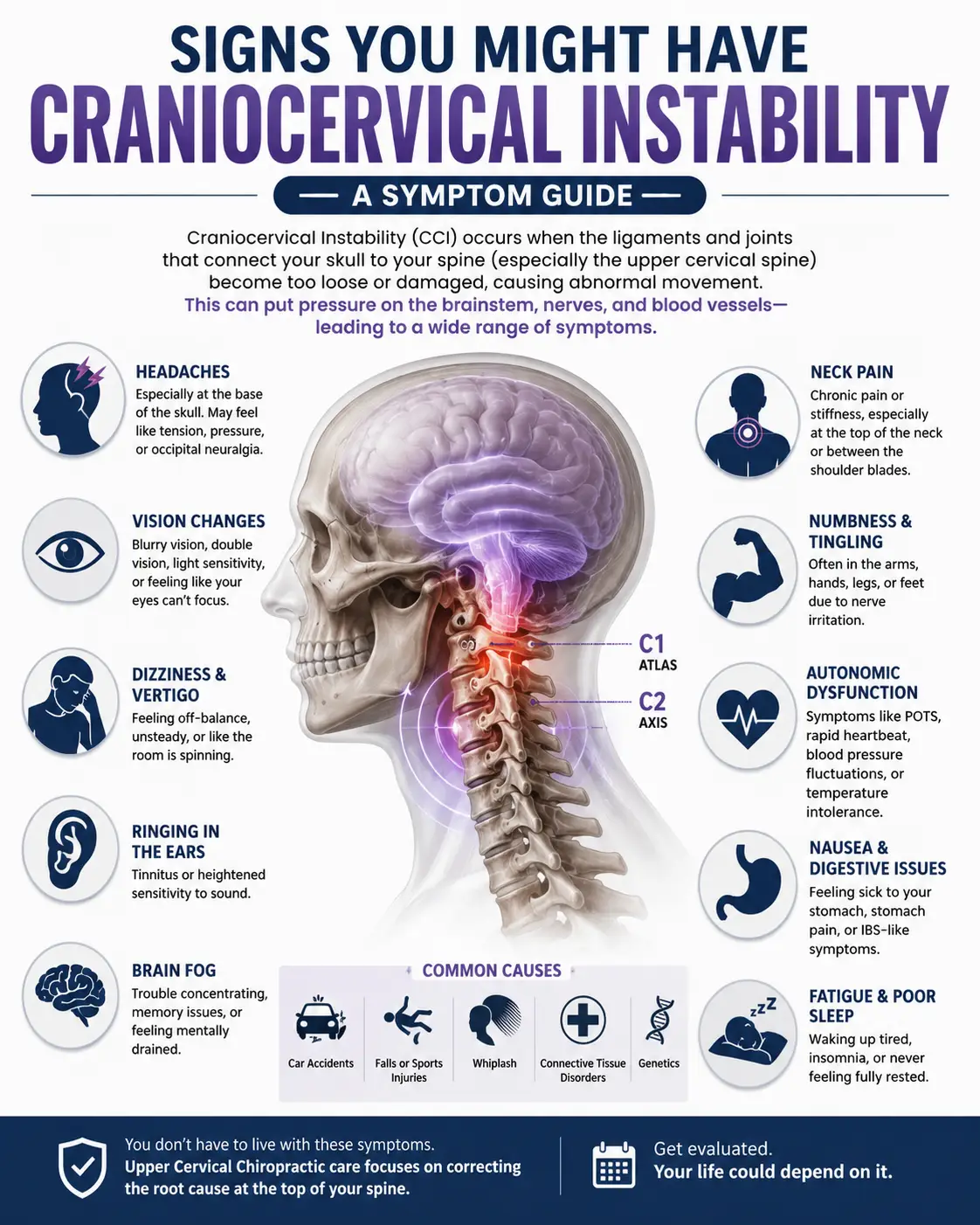
When the ligaments that stabilize this junction are more elastic than average, the head can move in ways it is not designed to move relative to the neck. This is the essence of craniocervical instability (CCI), a condition that shows up disproportionately in people with connective-tissue disorders. Headaches at the base of the skull, a heavy head that feels hard to hold up, brain fog, dizziness, and a constellation of autonomic symptoms such as those seen in POTS and dysautonomia can all be tangled up with what is happening at the top of the neck. If you have hEDS and you have ever felt like your head does not sit securely on your neck, you are not imagining things, and you are not alone.
At Lavender Family Chiropractic in Sarasota, Florida, Dr. Rusty Lavender and Dr. Jacob Temple focus specifically on the upper cervical spine, the atlas (C1) and axis (C2), using the precise, low-force Knee Chest Upper Cervical technique. This article explains how connective-tissue laxity affects the upper neck in hEDS, what the research says about craniocervical instability in Ehlers-Danlos syndrome, and how gentle, individualized upper cervical care may support people navigating these complex conditions, always in coordination with your medical team. We will also be clear and honest about what conservative care can and cannot do, because trust matters more than hype when your health is on the line.
Ehlers-Danlos syndrome: What Is the Connection Between hEDS and Craniocervical Instability?
Ehlers-Danlos syndrome is a group of heritable connective-tissue disorders that affect collagen, the protein that gives structure and strength to skin, tendons, ligaments, blood vessels, and the tissues that hold your joints in place. In the hypermobile type (hEDS), the most common form, the collagen that forms your ligaments tends to be more lax and extensible than typical. That laxity is exactly what produces the joint hypermobility, easy bruising, soft or stretchy skin, and frequent joint subluxations that many people with hEDS know all too well.
The problem is that ligaments do far more than let joints bend. Ligaments are the passive stabilizers of the body, the ropes and straps that quietly keep bones in their proper relationship to one another. When those straps are stretchier than average everywhere in the body, the joints that depend most heavily on ligamentous support become the most vulnerable. Nowhere is this dependence greater than at the craniocervical junction, the transition zone between the base of the skull (occiput), the first cervical vertebra (atlas, C1), and the second cervical vertebra (axis, C2).
Unlike the lower spine, which is stabilized by large interlocking bones, thick discs, and heavy musculature, the upper neck is built for mobility. Roughly half of the rotation of your head happens at the C1-C2 joint alone. To allow that remarkable range of motion, the region relies heavily on a set of specialized ligaments rather than bony blocks. In a person with normal collagen, those ligaments hold the head snugly in place while still permitting movement. In a person with hEDS, those same ligaments may allow slightly more motion than the anatomy was designed to tolerate. Over time, and especially after whiplash, repetitive strain, or the cumulative wear of a lifetime of hypermobility, that extra motion can translate into craniocervical instability.
A systematic review of craniocervical instability in Ehlers-Danlos syndrome published in Global Spine J examined the diagnostic and surgical treatment criteria used for CCI in EDS patients and highlighted how connective-tissue laxity contributes to instability at the craniocervical junction. The connection between hypermobility disorders and upper cervical instability is now well recognized in the medical literature, even as researchers continue to refine how it is best diagnosed and measured. To understand the broader picture of this condition, our detailed craniocervical instability resource page walks through the full landscape of CCI, its causes, and its evaluation.
It is worth emphasizing from the start: craniocervical instability in the true, structural sense is a medical diagnosis. It requires appropriate imaging, clinical evaluation, and often the input of specialists such as neurologists and neurosurgeons. Upper cervical chiropractic care does not diagnose or treat structural instability in place of that medical evaluation. What precise upper cervical care can offer is a different and complementary role, which we will explain in detail below.
The Mechanisms: Ligamentous Laxity at the Craniocervical Junction
To appreciate why the upper neck is so important in hEDS, it helps to understand the actual anatomy holding your head onto your spine. The craniocervical junction is stabilized by an elegant network of ligaments, each with a specific job.
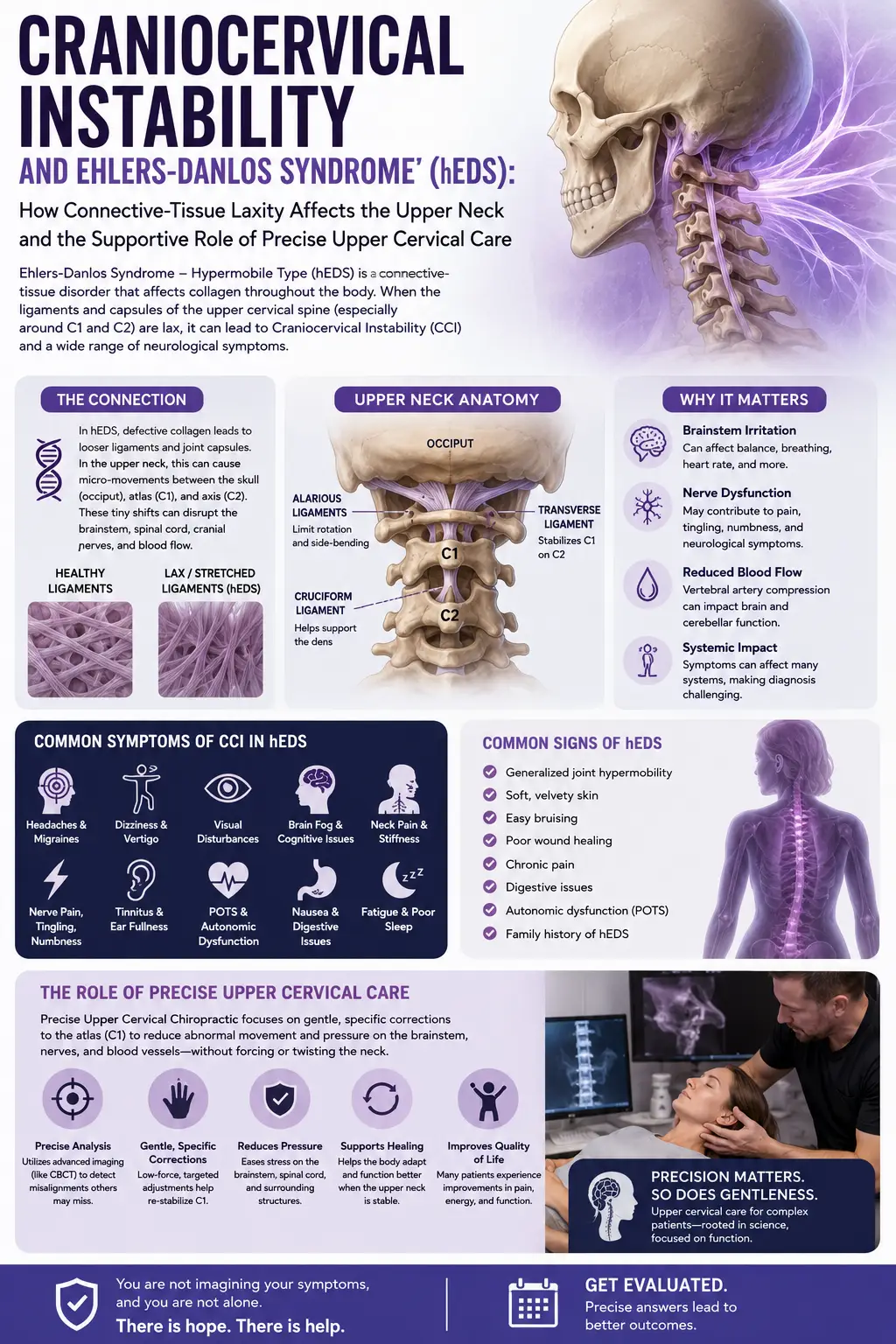
The alar ligaments run from the tip of the odontoid process (the peg-like projection of the axis, C2) up to the occiput on either side. They act like check-reins, limiting how far the head can rotate and side-bend relative to the neck. The transverse ligament of the atlas is arguably the single most important stabilizer at the top of the spine. It stretches across the ring of the atlas and holds the odontoid process snugly against the front arch of C1, preventing the peg from drifting backward toward the spinal cord and brainstem. Supporting these are the tectorial membrane, the apical ligament, the cruciate ligament complex, and the accessory ligaments, all working together to keep the head securely positioned while still allowing the wide range of motion the neck needs.
A thorough anatomic, functional, and radiographic review of the ligaments of the craniocervical junction published in the Journal of Craniovertebral Junction and Spine details how these ligaments contribute to stability and what happens when they are compromised. When collagen is more extensible than normal, as in hEDS, these check-reins simply do not check quite as firmly. The alar ligaments may permit excess rotation, and the transverse ligament may allow the odontoid to translate slightly more than it should. Individually, small increases in laxity may be tolerable. Cumulatively, and especially in the setting of a lifetime of connective-tissue laxity, they can add up to meaningful instability.
Why does this matter so much? Because of what sits directly behind these ligaments. The craniocervical junction is the anatomical doorway to the brainstem and the upper spinal cord. The brainstem is home to the control centers for breathing, heart rate, blood pressure, swallowing, and countless other automatic functions. The vagus nerve, the great highway of the parasympathetic nervous system, exits the skull in this same neighborhood. When the bones and ligaments of the upper neck are not holding their proper relationships, the surrounding neural structures can be affected in ways that produce far-reaching symptoms.
This is where the striking overlap between hEDS, craniocervical instability, and dysautonomia comes into focus. Postural orthostatic tachycardia syndrome (POTS) and other forms of dysautonomia are strikingly common in people with hEDS. The autonomic nervous system, which regulates blood pressure, heart rate, digestion, and temperature, is heavily represented in the brainstem and upper cervical region. A review of the neurological manifestations of Ehlers-Danlos syndrome published in the Iranian Journal of Neurology catalogs the wide range of neurological and autonomic features seen across the EDS spectrum, including headaches, dysautonomia, and the effects of craniocervical instability. For patients whose autonomic symptoms are a major part of their daily struggle, our pages on dysautonomia and POTS and vagus nerve dysfunction explore this connection in greater depth.
In the most serious situations, structural instability at the craniocervical junction can lead to ventral brainstem compression and a cluster of symptoms known as cervical medullary syndrome. A five-year follow-up study of cervical medullary syndrome secondary to craniocervical instability published in Neurosurgical Review documented patients with hereditary hypermobility connective-tissue disorders who required surgical craniocervical reduction, fusion, and stabilization, and it described the craniometric measurements used to identify these severe cases. This underscores an important point: when instability is severe and neurological structures are being compressed, this is a surgical and neurosurgical concern, not something conservative care addresses. Recognizing which situation you are in is one of the most important parts of navigating hEDS wisely.
Why the Upper Neck (Atlas/Axis, C1/C2) Matters in hEDS
If the craniocervical junction is the doorway to the brainstem, the atlas and axis are the hinges on that door. The atlas (C1) is a delicate ring of bone that cradles the base of the skull and lets your head nod and rotate. The axis (C2) provides the odontoid pivot around which the atlas turns. Together, these two vertebrae carry the entire weight of the head, roughly ten to twelve pounds, while permitting an extraordinary range of motion. It is a beautiful piece of biomechanical engineering, but it is also inherently dependent on soft-tissue stabilization, which is precisely why hEDS can complicate it.
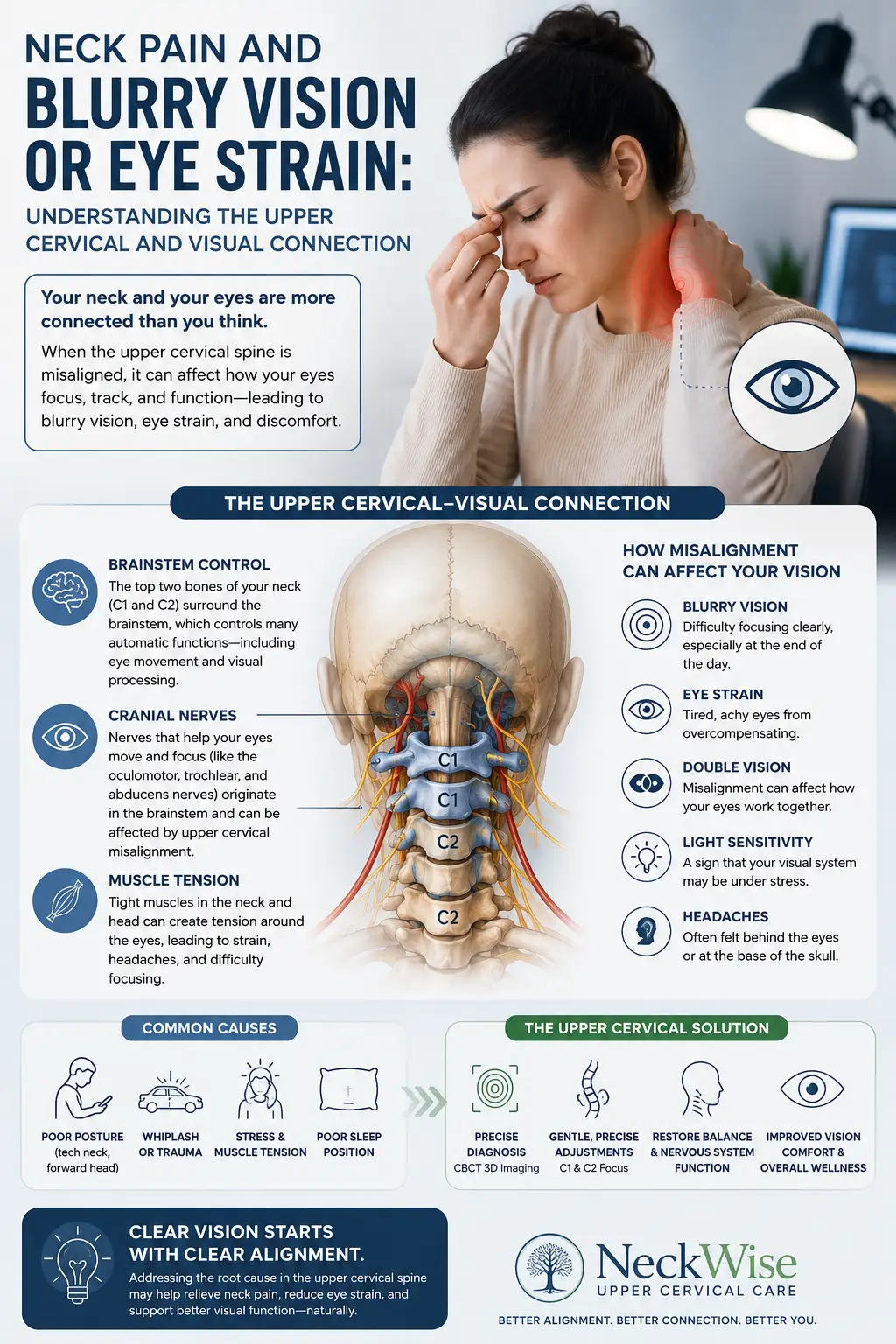
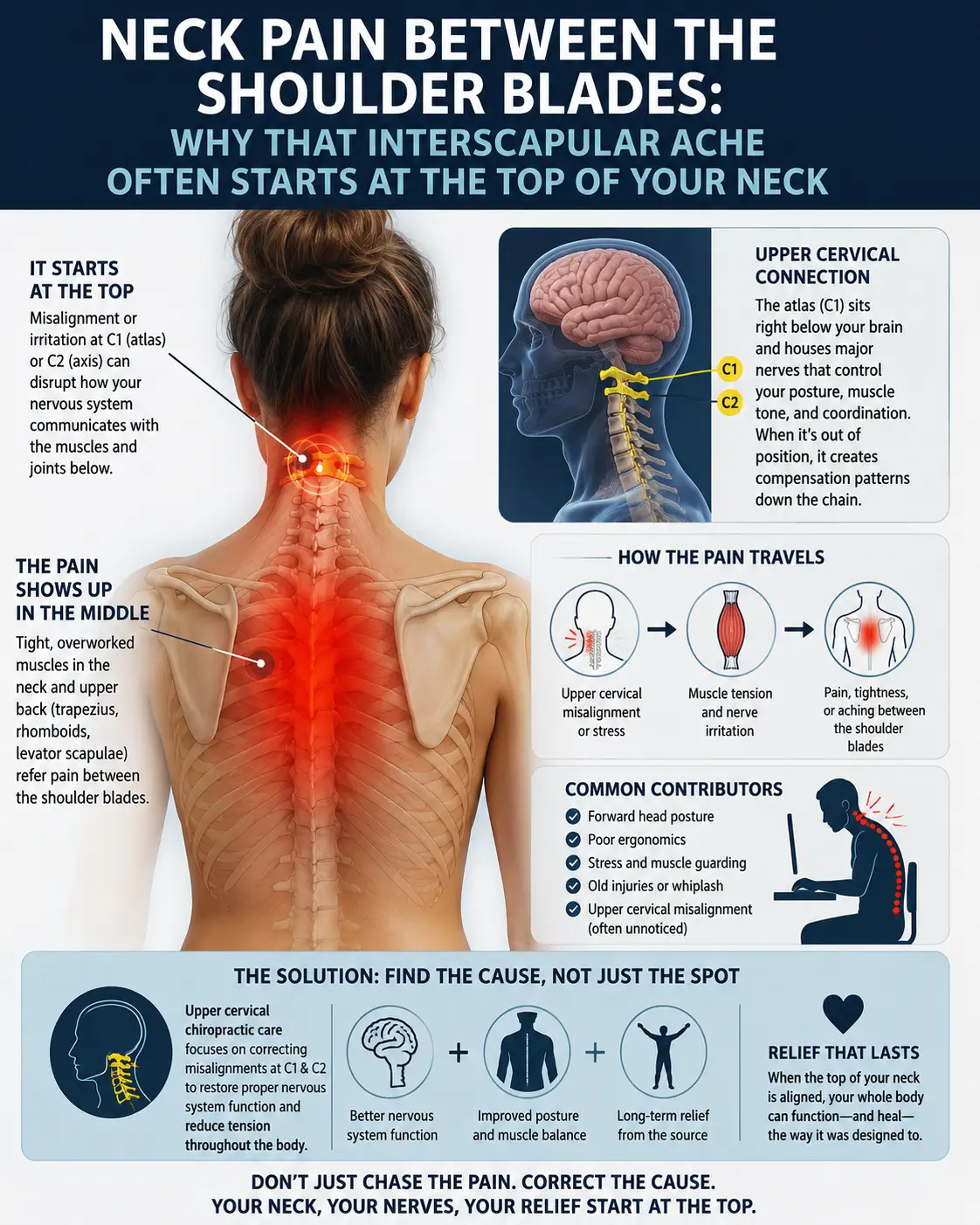
When the atlas and axis are positioned well and moving in balance, the head sits comfortably centered over the spine, the muscles of the neck can relax rather than constantly bracing, and the neural structures passing through the region have the room they need. When the relationship between C1, C2, and the skull is disturbed, even subtly, a cascade of secondary effects can follow. The small muscles of the suboccipital region may go into protective guarding, which can produce the deep, aching headaches at the base of the skull that so many hEDS patients describe. The proprioceptive signals from the upper neck, which the brain relies on to know where the head is in space, can become distorted, contributing to dizziness, unsteadiness, and visual disturbances. And the constant effort of stabilizing a hypermobile upper neck can leave the muscles fatigued and the whole region feeling fragile.
For people with hEDS, the upper neck often becomes the site where hypermobility hurts the most, because it is the one place where a little extra motion has such outsized consequences. This is also why the upper neck deserves such careful, precise, and gentle attention rather than aggressive intervention. A hypermobile craniocervical junction does not need to be forced, twisted, or cranked. It needs to be understood, measured, and supported with the lightest effective touch. That philosophy is the entire foundation of the upper cervical chiropractic care that Dr. Lavender and Dr. Temple provide.
It is also important to recognize how the upper neck ties into whole-body symptoms that hEDS patients frequently report. Chronic fatigue, unrefreshing sleep, and a persistent sense of being wired-yet-tired often accompany connective-tissue disorders and their autonomic features. Many patients who live with these overlapping conditions find our page on chronic fatigue syndrome and ME/CFS helpful for understanding how upper cervical function, autonomic regulation, and energy are interconnected.
How Precise Upper Cervical Care Fits at Lavender Family Chiropractic
Let us be direct and honest, because you deserve nothing less. Upper cervical chiropractic care does not physically repair torn or lax ligaments, and it does not reverse the underlying collagen differences that define hEDS. We do not claim to cure Ehlers-Danlos syndrome or craniocervical instability, and any provider who promises to do so is not telling you the truth. What precise, low-force upper cervical care offers is something more modest and, for many patients, meaningfully valuable: a careful effort to improve the position and balance of the atlas and axis so that the head is better centered, the surrounding muscles are less strained, and the nervous system has a better environment in which to regulate itself. For someone whose upper neck is working overtime, that supportive role may make a real difference in daily comfort and function.
Here is how the process works at Lavender Family Chiropractic in Sarasota.
A Thorough Consultation and Screening
Everything begins with listening. Dr. Lavender and Dr. Temple take the time to understand your full history, your hEDS diagnosis, your symptoms, your prior imaging, and what you have already tried. This is also where we screen carefully for red flags. If your presentation suggests true structural instability or neurological compromise, our role is to help make sure you are connected with the appropriate medical specialists. Good care starts with knowing which problems belong to which providers, and we take that responsibility seriously. Learn more about the doctors on our meet the team page.
Precise 3D CBCT Imaging
You cannot correct what you cannot see, and the upper cervical spine is far too important to approach with guesswork. We use 3D cone beam computed tomography (CBCT) imaging to visualize the atlas and axis in three dimensions with remarkable detail. This lets us understand the unique architecture of your upper neck and design a correction specific to your anatomy rather than a generic, one-size-fits-all approach. For patients with connective-tissue disorders, this precision matters even more, because the last thing a hypermobile upper neck needs is a nonspecific, forceful intervention.
Tytron Paraspinal Infrared Thermography
To understand how your nervous system is functioning, not just how your bones are arranged, we use Tytron paraspinal infrared thermography. This non-invasive scan measures subtle patterns of heat along the spine that reflect autonomic nervous system activity. Because dysautonomia is so common in hEDS, this objective measurement helps us track how your system is responding over time and whether the care is having a supportive effect on autonomic balance.
The Precise, Low-Force Knee Chest Upper Cervical Correction
The heart of our care is the Knee Chest Upper Cervical technique, a precise, gentle, low-force correction of the atlas and axis. This is essential to understand, especially for anyone with hEDS or possible instability: our correction is not high-velocity, twisting manipulation, and it is not the forceful, cracking style of adjustment that many people picture when they think of a chiropractor. Those aggressive, high-velocity manipulations are exactly what people with connective-tissue laxity and possible upper cervical instability are typically advised to avoid, and we agree. That is not what we do.
The Knee Chest Upper Cervical correction is deliberately light, specific, and controlled. It is designed to gently guide the atlas toward a better position based on your individual CBCT measurements, using the least force necessary. For hypermobile patients, this gentle-by-design philosophy is not a limitation; it is the entire point. The goal is to work with your anatomy, not against it, and to support better balance without adding strain to already-lax tissue.
Customized Care Plans and Coordination With Your Medical Team
Because no two people with hEDS are alike, we build customized care plans around your specific findings, symptoms, and goals. Some patients respond quickly, others more gradually, and some conditions require a slower, lighter, and more conservative pace. We would rather do less and do it well than push a hypermobile system too hard.
Just as importantly, we see our role as one part of a larger team. If you are working with a geneticist, neurologist, cardiologist, physical therapist, or neurosurgeon, we want to coordinate with them, not replace them. Ehlers-Danlos syndrome is a whole-body condition, and the best outcomes tend to come from collaboration. If your situation calls for medical management that is outside the scope of chiropractic care, we will say so plainly and help you get there.
Take the Next Step Toward Support in Sarasota
If you are living with hEDS and struggling with upper neck symptoms, headaches at the base of the skull, dizziness, or autonomic issues, you do not have to figure it all out alone. Dr. Rusty Lavender and Dr. Jacob Temple offer a careful, gentle, and honest approach to upper cervical care that may support your journey alongside your medical team.
Call Lavender Family Chiropractic at (941) 243-3729 to ask questions or schedule a consultation. You can also book your new patient appointment online anytime. Our office is located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, at the corner of University and Whitfield, convenient to Sarasota, Bradenton, and Lakewood Ranch.
What the Research Says
Science should guide expectations, and we believe in pointing you to the primary literature so you can read it for yourself. Here are five peer-reviewed sources that inform our understanding of craniocervical instability and Ehlers-Danlos syndrome. Note that much of this research focuses on severe, structural, and surgical cases; it is included to build an accurate picture of the condition, not to suggest that conservative upper cervical care treats structural instability.
- Craniocervical Instability in Ehlers-Danlos Syndrome — A Systematic Review of Diagnostic and Surgical Treatment Criteria (Lohkamp, Marathe, and Fehlings, Global Spine Journal, 2022). This systematic review examines how craniocervical instability is diagnosed and surgically managed in patients with Ehlers-Danlos syndrome, highlighting the role of connective-tissue laxity and the ongoing effort to standardize diagnostic criteria.
- Neurological Manifestations of Ehlers-Danlos Syndrome(s): A Review (Castori and Voermans, Iranian Journal of Neurology, 2014). This review surveys the broad range of neurological and autonomic features associated with the EDS spectrum, including headaches, dysautonomia, and complications related to craniocervical instability.
- Anatomic, Functional, and Radiographic Review of the Ligaments of the Craniocervical Junction (Fiester, Rao, Soule, Orallo, and Rahmathulla, Journal of Craniovertebral Junction and Spine, 2021). This paper details the anatomy and stabilizing function of the ligaments at the craniocervical junction, including the alar and transverse ligaments, and how their compromise contributes to instability.
- Cervical Medullary Syndrome Secondary to Craniocervical Instability and Ventral Brainstem Compression in Hereditary Hypermobility Connective Tissue Disorders (Henderson and colleagues, Neurosurgical Review, 2019). This five-year follow-up study describes patients with hypermobility connective-tissue disorders and severe craniocervical instability who underwent surgical reduction, fusion, and stabilization, and it outlines the craniometric measurements used to identify these cases.
- Ehlers-Danlos Syndrome: Not Just Joint Hypermobility (Bregant and Klopcic Spevak, Case Reports in Medicine, 2018). This report illustrates that Ehlers-Danlos syndrome extends well beyond flexible joints, affecting multiple body systems and underscoring the importance of a whole-person, multidisciplinary approach to care.
Lifestyle and Self-Care with hEDS
Beyond any professional care, the daily habits you build have a real influence on how your upper neck and your whole body feel. With hEDS, the guiding principle is gentleness and consistency rather than intensity. Here are approaches many hypermobile patients find supportive, always to be individualized with your own care team.
First and most important: avoid aggressive self-cracking of your own neck. When your neck feels tight or stuck, the temptation to twist it forcefully until it pops can be almost irresistible, and the relief afterward feels real. But for a hypermobile craniocervical junction, repeatedly forcing that motion tends to stretch already-lax ligaments even further and can reinforce a cycle of instability and tightness. The muscles tighten precisely because they are trying to stabilize a joint that moves too much, and forcing the pop only prompts them to guard again. If you find yourself needing to crack your neck constantly, that is a signal worth discussing with a provider rather than a habit to lean into.
Gentle, targeted strengthening is often the cornerstone of managing hypermobility. Because ligaments cannot be made tighter, the muscular system has to take on more of the stabilizing role. Working with a physical therapist experienced in hypermobility, especially on the deep neck flexors and the postural muscles that support the head, can help build the active stability that lax ligaments cannot provide on their own. The key is slow, controlled, low-load work rather than aggressive stretching, since people with hEDS are usually flexible enough already and benefit far more from stability than from added range of motion.
Pay attention to posture and daily ergonomics, particularly how you hold your head during screen time. Prolonged forward head posture asks the upper neck to bear the weight of the head at a mechanical disadvantage, which is especially taxing on hypermobile tissue. Setting screens at eye level, taking frequent movement breaks, and supporting your head and neck well during sleep can meaningfully reduce the cumulative strain.
Support your nervous system as a whole. Because dysautonomia so often travels with hEDS, strategies that support autonomic balance can help: adequate hydration and, when your physician recommends it, appropriate salt intake for those with POTS; gentle, graded activity that respects your energy envelope; good sleep hygiene; and stress-regulation practices such as slow breathing that engage the calming parasympathetic system. For a deeper look at how upper cervical function relates to energy and fatigue in these overlapping conditions, our article on chronic fatigue and the upper cervical connection offers additional perspective.
Finally, honor your body’s signals. Hypermobile bodies often push through pain and fatigue because the alternative feels like giving up too much. But pacing, rest, and gentleness are not weakness; they are strategy. The people who tend to do best with hEDS are those who learn to work with their bodies patiently rather than fighting them.
Serving Sarasota and Surrounding Communities
Lavender Family Chiropractic is proud to serve patients from across the greater Sarasota region who are seeking precise, gentle, upper cervical care. Because upper cervical care and the conditions surrounding hEDS and craniocervical instability are so specialized, patients often travel a good distance to work with us, and we welcome them warmly.
We serve individuals and families throughout Sarasota, Bradenton, Lakewood Ranch, Venice, Palmer Ranch, Osprey, Siesta Key, Longboat Key, Lido Key, University Park, Parrish, Ellenton, Myakka City, Punta Gorda, and St. Petersburg. Our office sits at the corner of University and Whitfield, making it easy to reach from communities to the north, south, and east. If you are living with hEDS anywhere in the region and wondering whether gentle upper cervical care might support you, we would be glad to talk. You can always reach us through our contact page or by phone at (941) 243-3729.
Top 15 Questions About hEDS and Craniocervical Instability
1. What is craniocervical instability in the context of hEDS?
Craniocervical instability refers to excess motion between the skull, the atlas (C1), and the axis (C2) due to insufficient ligamentous support. In hEDS, the collagen that forms the stabilizing ligaments of the upper neck tends to be more lax, which can allow the head to move more than it should relative to the neck. True structural CCI is a medical diagnosis that requires appropriate imaging and specialist evaluation.
2. Why is the upper neck especially vulnerable in Ehlers-Danlos syndrome?
The craniocervical junction relies heavily on ligaments rather than bony blocks for stability, because it is built for a wide range of motion. When those ligaments are more extensible, as in hEDS, the region that depends most on ligamentous support becomes the most affected by connective-tissue laxity.
3. Can upper cervical chiropractic care cure my hEDS or craniocervical instability?
No. We want to be completely honest about this. Upper cervical care does not cure Ehlers-Danlos syndrome, does not reverse the underlying collagen differences, and does not physically repair torn or lax ligaments. What precise, low-force care may do is support better positioning and balance of the atlas and axis, which for some patients is associated with improved comfort and function. Any provider promising a cure is not being truthful.
4. Is your adjustment the forceful, twisting kind of neck cracking?
No. The Knee Chest Upper Cervical technique we use is a precise, gentle, low-force correction. It is specifically not high-velocity, twisting manipulation and not the forceful cracking style of adjustment. This gentle-by-design approach is one reason it is so well suited to hypermobile patients, since it works with your anatomy rather than forcing it.
5. When should I see a physician or neurosurgeon instead of pursuing conservative care?
Certain red-flag symptoms warrant urgent medical evaluation rather than conservative care. These include progressive weakness, problems with coordination or balance, changes in speech or swallowing, fainting, or symptoms that are rapidly changing or worsening. These can signal serious neurological involvement and require prompt attention from the appropriate medical specialists. When in doubt, seek medical care first.
6. How do you know whether my upper neck problem is structural instability or something conservative care can support?
That is exactly what our consultation and screening process is designed to explore. We take a careful history, review your imaging, and screen for red flags. If your presentation suggests true structural instability or neurological compromise, we help connect you with the appropriate medical specialists. Recognizing which problems belong to which providers is a core part of responsible care.
7. Why do so many people with hEDS also have POTS or dysautonomia?
The autonomic nervous system, which controls heart rate, blood pressure, and digestion, is heavily represented in the brainstem and upper cervical region, and connective-tissue laxity can affect blood vessels and autonomic regulation throughout the body. This is why dysautonomia and POTS are so common in hEDS. Our pages on dysautonomia and POTS and vagus nerve dysfunction explore this relationship in more depth.
8. What imaging do you use, and why does it matter for hypermobile patients?
We use 3D cone beam CT (CBCT) imaging to visualize the atlas and axis in three-dimensional detail. This precision lets us tailor a correction to your unique anatomy rather than using a generic approach, which is especially important when working with a hypermobile upper neck that needs a specific, gentle touch.
9. What is Tytron thermography and why do you use it?
Tytron paraspinal infrared thermography is a non-invasive scan that measures heat patterns along the spine reflecting autonomic nervous system activity. Because autonomic dysfunction is common in hEDS, this objective measurement helps us monitor how your nervous system is responding over the course of care.
10. Do you take insurance?
We are a cash-pay, out-of-network practice and do not bill insurance directly. This allows us to focus on individualized, unhurried care rather than being constrained by insurance requirements. We provide superbills that you can submit to your insurance company for potential out-of-network reimbursement, depending on your specific plan.
11. What are superbills and how do they work?
A superbill is an itemized receipt of the care you received, including the appropriate codes your insurance company may need. While we do not bill insurance on your behalf, we provide superbills so you have the documentation to seek any out-of-network reimbursement your plan may offer. Reimbursement depends entirely on your individual insurance coverage.
12. How long will I need care, and what does a care plan look like?
Every person with hEDS is different, so we build customized care plans around your specific findings, symptoms, and goals. Some patients respond quickly and others more gradually, and hypermobile systems often benefit from a slower, gentler, more conservative pace. We would rather do less and do it well than push too hard.
13. Is upper cervical care safe if I have hEDS or suspected instability?
Our care is built around precision and the lightest effective force, which is a very different thing from aggressive, high-velocity manipulation. That said, safety starts with proper screening. If you have suspected or confirmed structural instability, we coordinate with your medical team and adjust our approach accordingly, and in some cases we may recommend that medical management take the lead. Honest screening is how we help keep care appropriate for your situation.
14. Should I stop cracking my own neck?
For hypermobile patients, repeatedly forcing your own neck to pop tends to stretch already-lax ligaments further and reinforce a cycle of instability and muscle guarding. If you feel a constant need to self-crack, that is a signal worth discussing with a provider rather than a habit to continue. Gentle strengthening and professional evaluation are usually more supportive paths.
15. Can you work together with my other doctors?
Yes, and we prefer to. Ehlers-Danlos syndrome is a whole-body condition, and the best outcomes tend to come from collaboration. If you are working with a geneticist, neurologist, cardiologist, physical therapist, or neurosurgeon, we want to coordinate with them as one part of your larger care team, not as a replacement for medical management.
Closing: A Gentle, Honest Path Forward
Living with hEDS and the upper neck challenges that can come with it is genuinely hard, and you deserve providers who are both skilled and honest with you. At Lavender Family Chiropractic, Dr. Rusty Lavender and Dr. Jacob Temple offer precise, low-force upper cervical care that may support your comfort and function, always with clear eyes about what conservative care can and cannot do, and always in coordination with your medical team. We will never overpromise, and we will always point you toward urgent medical care when that is what your situation calls for.
If you are ready to explore whether gentle upper cervical care might have a supportive role in your journey, we would be honored to talk with you. Call (941) 243-3729 to ask questions or schedule a consultation, or book your appointment online at your convenience. You will find us at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, at the corner of University and Whitfield.
Related Articles
- Craniocervical Instability (CCI): The Complete Guide — Our comprehensive pillar resource on craniocervical instability, its causes, evaluation, and the role of precise upper cervical care. Start here for the full picture.
- Dysautonomia and POTS — How autonomic dysfunction connects to the upper cervical spine, a common concern for people with hEDS.
- Chronic Fatigue Syndrome and ME/CFS in Sarasota — Exploring the links between upper cervical function, energy, and persistent fatigue.
- Vagus Nerve Dysfunction — Understanding the vagus nerve, the parasympathetic system, and the upper neck.