By Dr. Rusty Lavender and Dr. Jacob Temple
If you have myalgic encephalomyelitis/chronic fatigue syndrome — ME/CFS — you already know what it is to be exhausted at a level that other people cannot quite comprehend. The fatigue that does not lift with rest. The post-exertional malaise that means a single load of laundry can put you in bed for two days. The brain fog that makes reading a paragraph an act of will. The orthostatic intolerance that makes standing up feel like a punishment. The unrefreshing sleep that leaves you more tired in the morning than when you went to bed. The slow erosion of your career, your relationships, and the version of yourself you used to recognize. And, in many cases, the diagnostic odyssey of being told by provider after provider that your labs look fine, that maybe it is depression, that maybe you should try harder, that maybe you just need to exercise.
At Lavender Family Chiropractic in Sarasota, Florida, we see ME/CFS patients regularly. They are among the most misunderstood, undertreated, and disbelieved patient populations in modern medicine. Many also carry diagnoses of POTS, hypermobile Ehlers-Danlos syndrome, fibromyalgia, MCAS, or long COVID — and almost none of them have ever been thoroughly evaluated for what may be one of the most important mechanical contributors to their illness: the alignment and stability of the upper cervical spine, where the brainstem, the cerebrospinal fluid flow pathways, and the autonomic nervous system all converge.
This guide is for anyone in Sarasota, Bradenton, Lakewood Ranch, or the surrounding areas who has been carrying ME/CFS — diagnosed or suspected, mild or severe, recent-onset or decades-long — and who is searching for an angle that has not yet been offered. Through the precise, gentle Knee Chest Upper Cervical technique used by Dr. Rusty Lavender and Dr. Jacob Temple, we work to address the structural and neurological dysfunction at the craniocervical junction that recent research has identified as a meaningful contributor to ME/CFS symptoms in a substantial subset of patients.
What Is ME/CFS?
Myalgic encephalomyelitis/chronic fatigue syndrome is a complex, multi-system, chronic illness characterized by severe, disabling fatigue that is not relieved by rest, post-exertional malaise (PEM), unrefreshing sleep, cognitive dysfunction, and orthostatic intolerance. The official name combines two historical terms — myalgic encephalomyelitis, which emphasizes the neurological and inflammatory features, and chronic fatigue syndrome, which emphasizes the cardinal symptom. The modern consensus accepts both names as referring to the same condition and uses ME/CFS as the umbrella term.
The defining feature that separates ME/CFS from ordinary fatigue or general deconditioning is post-exertional malaise — a delayed worsening of symptoms following physical, cognitive, or emotional exertion, often disproportionate to the exertion and sometimes lasting days to weeks. This is not “feeling tired after activity.” This is a measurable, multi-system flare in which fatigue, pain, brain fog, sleep disruption, autonomic symptoms, and sometimes flu-like symptoms all worsen together, often after a delay of 12 to 48 hours. PEM is the cardinal feature, and it is what distinguishes ME/CFS from depression, deconditioning, and most other fatigue-producing conditions.
The associated symptom profile is wide. Patients commonly report cognitive dysfunction (“brain fog”), unrefreshing sleep, orthostatic intolerance (frequently formal POTS), widespread pain, headaches, sensory hypersensitivities, gastrointestinal symptoms, immune-type symptoms (sore throat, tender lymph nodes, flu-like flares), temperature dysregulation, and a profound exercise intolerance that often leads patients to learn the hard discipline of pacing.
How common is ME/CFS? The numbers vary by definition and methodology. According to NCHS data from the U.S. National Center for Health Statistics during 2021–2022, 1.3% of U.S. adults reported having ME/CFS — corresponding to roughly 3.35 million adults. A 2025 PMC scoping review on the burden of ME/CFS estimated U.S. adult prevalence at approximately 0.42% using more stringent definitions and noted that prevalence is expected to rise significantly due to the COVID-19 pandemic and the substantial overlap between long COVID and ME/CFS criteria. A 2020 meta-analysis estimated global prevalence at approximately 0.89% with women affected approximately three times more often than men.
Translated to a region like Sarasota and the surrounding communities, the numbers mean tens of thousands of people locally are carrying some form of ME/CFS — many undiagnosed, many misdiagnosed, and many cycling through the medical system without ever receiving care that addresses the underlying mechanisms driving their illness.
The economic burden is substantial — estimated to exceed $20 billion annually in the United States alone — and the personal burden is often catastrophic. Many ME/CFS patients are unable to work, unable to maintain social or family obligations, and confined to home or bed for years on end. This is a serious, legitimate, biologically rooted illness, and any provider who treats it otherwise is failing the patient.
The Brainstem and Craniocervical Connection to ME/CFS
For a long time, the dominant medical model treated ME/CFS as a “functional” disorder of unclear etiology. That has been changing. Over the past decade, the research community has increasingly recognized ME/CFS as a neuroimmune, multi-system illness with measurable abnormalities in autonomic function, brain perfusion, neuroinflammation, and — critically for our purposes here — craniocervical structural factors.
The single most important paper that brought the craniocervical angle into mainstream ME/CFS research was a 2020 study by Bragée and colleagues published in Frontiers in Neurology. The investigators retrospectively analyzed 229 patients meeting Canada Consensus Criteria for ME/CFS at a specialist referral clinic and assessed them for hypermobility, signs of intracranial hypertension, and craniocervical obstructions on MRI. The findings were striking. Hypermobility was identified in 50% of patients, signs of possible intracranial hypertension were present in 83% of those who underwent brain MRI, and a substantial proportion showed craniocervical obstructions consistent with mechanical contributions to their symptoms. The authors concluded that hypermobility, intracranial hypertension, and craniocervical obstructions may be substantially overrepresented in patients with ME/CFS and may explain many of the symptoms.
This is not a fringe finding from a single small study. The Bragée paper has been broadly cited and built upon. The Karolinska Institutet, where the study was conducted, has continued to investigate the structural and mechanical contributions to ME/CFS, and active research programs at multiple institutions — including the Bragée Clinic’s follow-up ME-SH study with Harvard collaborators — are pursuing the brainstem and craniocervical hypothesis with increasing rigor.
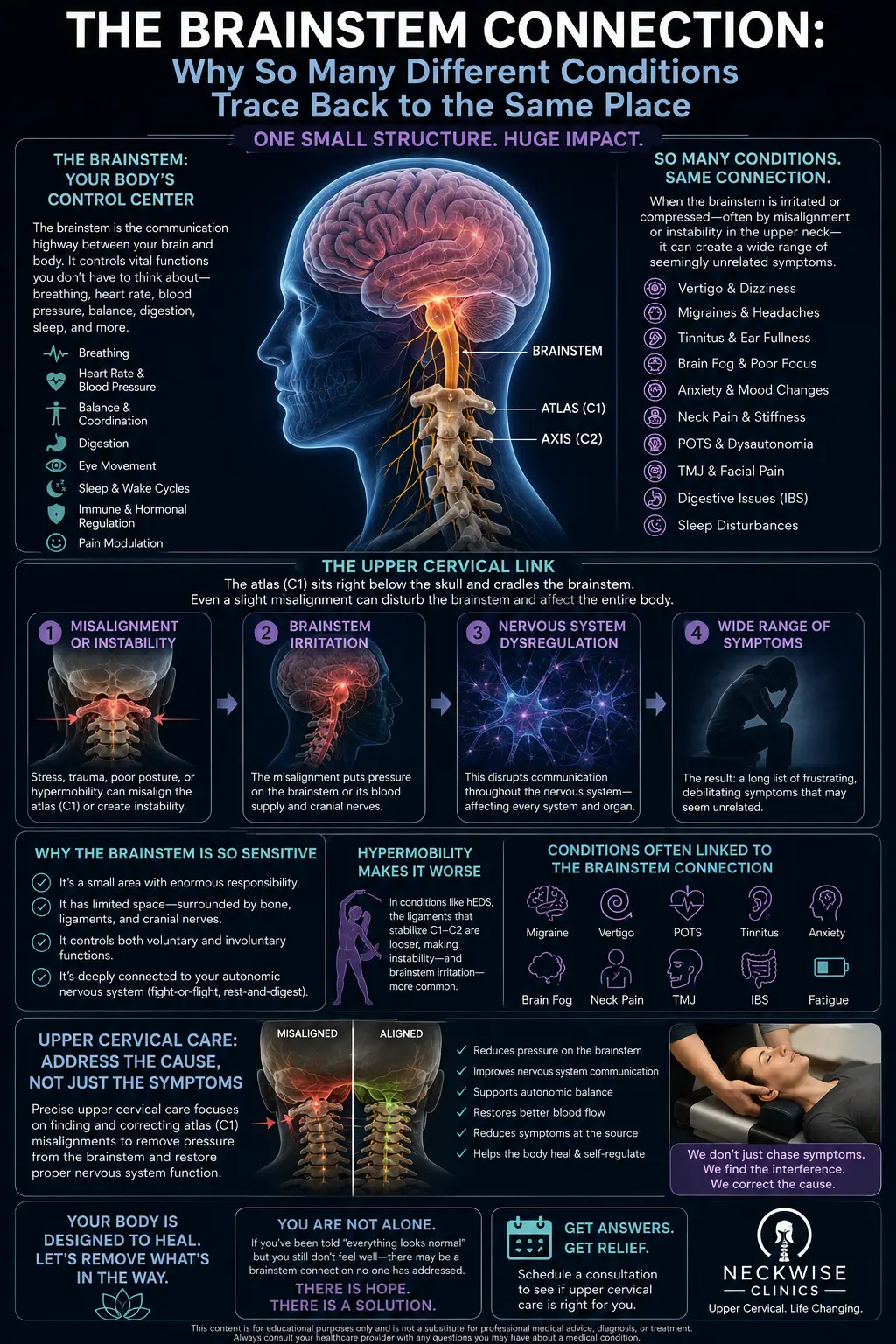
What does this mean clinically? It means that for a substantial subset of ME/CFS patients, the structural environment around the brainstem is part of the picture. The craniocervical junction houses the brainstem, the upper portion of the spinal cord, and the major cerebrospinal fluid (CSF) flow pathways that connect the brain to the rest of the central nervous system. The atlas (C1) and axis (C2) are the bony foundation of this region. The ligaments that hold the head onto the neck — the alar ligaments, the transverse ligament, the apical ligament, and the tectorial membrane — provide structural stability. When these ligaments are lax (often in hypermobility-spectrum patients), or when there is misalignment of C1 and C2, the mechanical environment around the brainstem is compromised.
The downstream consequences read like a checklist of ME/CFS symptoms. Brainstem compression or irritation disrupts autonomic regulation — producing the orthostatic intolerance, temperature dysregulation, and heart rate variability abnormalities that ME/CFS patients commonly report. Impaired CSF flow contributes to intracranial pressure abnormalities and the cognitive symptoms, headaches, and visual disturbances that come with them. Compromised proprioceptive input from the upper cervical joints disrupts the brainstem’s calibration of balance, pain modulation, and sympathetic-parasympathetic balance. The dural attachments at C1 and C2 transmit tension into the brainstem and upper spinal cord, contributing to the diffuse neurological dysfunction characteristic of the condition.
This is not the only mechanism in ME/CFS. The illness clearly involves immune dysregulation, mitochondrial dysfunction, neuroinflammation, and other processes that operate independently of craniocervical mechanics. But for the substantial subset of patients in whom the craniocervical component is meaningful, addressing it is one of the few interventions that targets the upstream structural cause rather than the downstream symptoms.
This is also why so many ME/CFS patients are now being evaluated for craniocervical instability — and why our service page on that condition is so frequently relevant to the ME/CFS patient population.
The ME/CFS, POTS, MCAS, EDS Cluster
One of the most striking patterns in ME/CFS is how often it travels with related conditions. Many patients carry multiple diagnoses — ME/CFS plus POTS plus mast cell activation syndrome plus hypermobile Ehlers-Danlos syndrome. The patient community often refers to this cluster as the “trifecta” or the “tetrad,” and the constellation has become increasingly recognized in the medical literature.
The connection is not coincidence. All of these conditions involve some combination of connective tissue dysfunction, autonomic dysregulation, immune dysfunction, and — for the substantial subset who fit the mechanical pattern — craniocervical involvement. Hypermobile EDS produces ligamentous laxity that can predispose to upper cervical instability. Upper cervical instability disrupts brainstem function, which contributes to autonomic dysregulation and POTS. Autonomic dysregulation impairs vagal tone, which weakens the cholinergic anti-inflammatory pathway and predisposes to mast cell instability and MCAS. The post-exertional malaise of ME/CFS, the orthostatic intolerance of POTS, and the flares of MCAS often share the same triggers and follow the same patterns.
This is why patients with one of these conditions are statistically far more likely to have at least one of the others, and why a clinician who treats only the symptom in front of them — only the fatigue, only the heart rate, only the histamine — often misses the structural and autonomic drivers connecting them all.
For an ME/CFS patient who also has POTS, EDS, or MCAS, the upper cervical evaluation is even more clinically relevant. The mechanical contribution may be a single thread that, when pulled, helps multiple conditions begin to settle simultaneously.
Why Upper Cervical Care Matters for ME/CFS Patients
Let us be clear, as we have been with every patient we see: upper cervical chiropractic does not cure ME/CFS. The condition is multifactorial, often severe, and frequently involves processes that no manual therapy can directly correct. What upper cervical care can offer is improvement of one of the most important and consistently overlooked mechanical contributors to ME/CFS — and for many patients, that improvement produces meaningful, sustained reduction in symptoms.
At Lavender Family Chiropractic, we use the Knee Chest Upper Cervical technique — a precise, gentle approach to correcting atlas and axis misalignments without any twisting, popping, or forceful manipulation. For ME/CFS patients specifically, this gentleness is essential. The nervous systems of ME/CFS patients are often in a hypervigilant, sympathetically dominant state, and aggressive manipulation can provoke significant post-exertional flares. The Knee Chest technique avoids those forces entirely while still delivering sub-millimeter precision in the correction.
For ME/CFS patients, upper cervical care can matter in several specific ways. First, restoring proper upper cervical alignment supports vagal tone and parasympathetic function — addressing the autonomic dysregulation that drives so many ME/CFS symptoms. Second, improving the mechanical environment at the craniocervical junction can support the cerebrospinal fluid flow and intracranial pressure dynamics that, per the Bragée research, are abnormal in a substantial portion of ME/CFS patients. Third, reducing the chronic noxious input from a misaligned upper cervical spine removes one of the inputs that has been feeding the neuroinflammation and central sensitization that characterize the condition. Fourth, for the subset of ME/CFS patients with concurrent POTS or hypermobility, the upper cervical work directly addresses one of the most clinically meaningful structural contributors.
The honest reality is that ME/CFS patients vary widely in their response to upper cervical care. Some experience meaningful improvement in fatigue, orthostatic intolerance, brain fog, sleep, and pain within weeks to months. Others experience more gradual or partial improvement. A minority do not respond meaningfully — and we are honest with these patients when we do not see what we hoped to see. What we can promise is a thorough evaluation, a clear explanation of what we find, and an honest assessment of whether upper cervical care is likely to be a meaningful part of your overall strategy.
We pace care very carefully for ME/CFS patients. The standard frequency we recommend for the general patient population is often too much for someone with severe ME/CFS and post-exertional malaise, and we adjust accordingly. Slower, gentler, more spaced visits are often better tolerated and produce better long-term outcomes than aggressive initial loading.
What Care Looks Like at Lavender Family Chiropractic
If you come to our Sarasota office for evaluation related to ME/CFS, here is what to expect.
Your first visit begins with a thorough consultation. Dr. Lavender or Dr. Temple will sit down with you and review your full history — onset story (gradual vs. post-infectious vs. post-traumatic), symptom profile, comorbid diagnoses, medications, supplements, previous providers, what has helped, what has not, and your specific PEM thresholds. ME/CFS patients have usually been through extensive medical workups, and we want all of that context. Critically, we ask about activity tolerance and pacing so we can structure care in a way that does not provoke post-exertional crashes.
The examination is adapted for ME/CFS patients. We use advanced 3D imaging to visualize your upper cervical alignment with sub-millimeter precision, autonomic function testing to objectively measure your nervous system state, postural and gait analysis, and a careful neurological examination. For patients with concurrent POTS, we incorporate orthostatic testing. For patients with severe PEM, we may schedule shorter initial visits and break the evaluation into multiple sessions to avoid triggering a crash.
If the examination reveals upper cervical findings consistent with someone who is likely to benefit, we will explain our recommendations openly. If your situation calls for evaluation by a craniocervical instability specialist (often a neurosurgeon at a specialized center), we will tell you that directly. We are part of a broader care team for most ME/CFS patients — never a substitute for it.
Care is delivered through the Knee Chest Upper Cervical technique, with the extreme gentleness ME/CFS patients require. We offer customized treatment plans tailored to each patient’s specific situation, recognizing that no two ME/CFS patients present identically and that pacing is essential.
Because ME/CFS frequently overlaps with broader neurological dysregulation, our work with these patients often touches on the territory covered by our complex neurological conditions care — designed precisely for patients whose symptoms cross multiple systems and whose diagnoses do not fit neatly into a single specialty.
📞 Call (941) 243-3729 to schedule your complimentary consultation 📅 Book your consultation online 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
What the Research Says About ME/CFS, Craniocervical Function, and the Brainstem
The research landscape on ME/CFS is evolving rapidly, and the craniocervical mechanism is one of the most active areas of investigation.
The 2023 NCHS Data Brief from the U.S. National Center for Health Statistics established the most current U.S. prevalence figures, documenting that 1.3% of U.S. adults reported having ME/CFS during 2021–2022, with women affected nearly twice as often as men and prevalence peaking in the 50–69 age range — establishing ME/CFS as a major and increasingly recognized public health condition.
The seminal 2020 study by Bragée and colleagues in Frontiers in Neurology provides the strongest evidence base for the craniocervical mechanism. In 229 patients meeting Canada Consensus Criteria for ME/CFS, the investigators documented hypermobility in 50%, signs of possible intracranial hypertension in 83% of those imaged, and craniocervical obstructions consistent with mechanical contributions to symptoms — a finding that the authors explicitly proposed could explain many of the symptoms of the condition.
A 2020 meta-analysis in PMC reported a global pooled estimate of ME/CFS prevalence of approximately 0.89%, with women affected more than men and significant variation by age and study setting — establishing the epidemiological context for the condition worldwide and highlighting that prevalence is likely to rise substantially due to post-COVID sequelae.
A 2024 JAMA Network Open cohort study from the RECOVER initiative examined ME/CFS-like illness following SARS-CoV-2 infection and found that the weighted prevalence of ME/CFS-like illness was 4.5% or less at 3 to 12 months after the index illness, with no significant difference between COVID-positive and COVID-negative groups — establishing that post-infectious ME/CFS is a real phenomenon and is not limited to COVID-19 specifically.
A 2025 PMC scoping review on the burden of ME/CFS confirmed the substantial health, social, and economic burden of the condition, with U.S. adult prevalence estimated at approximately 0.42% under stringent definitions, women affected three times as often as men, and prevalence expected to increase due to the COVID-19 pandemic — establishing the magnitude of the public health challenge and the urgency of effective treatment approaches.
This body of research does not prove that upper cervical chiropractic resolves ME/CFS. What it does establish is that the craniocervical mechanism is a legitimate, research-supported angle in a substantial portion of ME/CFS patients — and that the upper cervical evaluation we provide is targeting a real, measurable contributor to the condition rather than a hypothetical one.
Lifestyle Factors That Support ME/CFS Management
Upper cervical chiropractic care is one tool among many. For ME/CFS patients, the lifestyle scaffolding around care is essential, and the patients who do best tend to be the ones working multiple angles simultaneously and patiently.
Pacing. This is the single most important skill in ME/CFS management. Post-exertional malaise is real, predictable, and avoidable with disciplined pacing. The goal is to stay within your “energy envelope” — doing less than you think you can on good days so you do not crash later. Many patients find heart rate monitoring, step counting, or HRV-based pacing tools genuinely helpful.
Sleep optimization. Unrefreshing sleep is a cardinal feature of ME/CFS, and improving sleep quality often produces broader symptom improvement. Seven to nine hours, dark and cool room, consistent timing. Work with your medical provider on sleep medications if needed — sleep is medical intervention, not luxury.
Orthostatic support. For ME/CFS patients with concurrent POTS or orthostatic intolerance, salt and fluid loading, compression garments (waist-high are most effective), and gradual recumbent-to-upright conditioning can provide meaningful symptomatic improvement. Your treating physician can guide this in detail.
Anti-inflammatory eating. While there is no single “ME/CFS diet” with strong research support, minimizing processed foods, refined sugars, and inflammatory seed oils while emphasizing whole foods, omega-3-rich fish, and adequate protein supports general nervous system function. Many patients also benefit from identifying individual food triggers, especially if MCAS is part of the picture.
Hydration. Critical for any patient with orthostatic intolerance, autonomic dysregulation, or POTS. The Florida climate makes this even more relevant. Aim for at least half your body weight in ounces of water daily, often with added electrolytes.
Stress management and vagal tone work. Chronic sympathetic activation worsens nearly every ME/CFS symptom. Slow diaphragmatic breathing, gentle restorative yoga, time in nature, social connection with safe people, and trauma-informed therapy when relevant all support the parasympathetic recovery state your nervous system desperately needs.
Gentle, paced movement. Exercise is one of the most controversial topics in ME/CFS care — graded exercise therapy has been debunked and is no longer recommended as a primary intervention. What does work is gentle, recumbent-friendly, carefully paced movement that does not provoke PEM. Some patients tolerate water exercise, recumbent cycling, or short walks. Many do better with simply increasing daily movement gradually rather than structured exercise.
Medical management. Continue working with your treating physicians. Low-dose naltrexone, antivirals, mast cell stabilizers, beta blockers, and other targeted prescriptions have legitimate roles for various ME/CFS subtypes. Upper cervical care complements this work — it does not replace it.
If you found this guide useful, you may also want to read about mast cell activation syndrome — a common comorbidity in ME/CFS patients that shares many of the autonomic and vagus nerve mechanisms we work with here.
Serving Sarasota and the Surrounding Communities
Lavender Family Chiropractic is located in Sarasota, Florida, at 5899 Whitfield Avenue, Suite 107 — at the corner of University and Whitfield. From this central location, we serve patients throughout the region, including Bradenton, Lakewood Ranch, Palmetto, Parrish, Venice, Osprey, Nokomis, Ellenton, Ruskin, Myakka City, North Port, and the greater Tampa Bay area. Patients also travel from St. Pete, Riverview, and Manatee County to receive specialized upper cervical care here.
ME/CFS is the kind of condition where patients are often willing to travel — though we recognize that travel itself can be a major burden for ME/CFS patients. We work with patients on care schedules that accommodate severe energy limitations, including longer intervals between visits when needed and shorter session lengths for those with significant PEM. If you have been searching for a provider who understands the structural and autonomic components of your illness and who will work within your real-world limits, we encourage you to reach out.
Top 15 FAQs About ME/CFS and Upper Cervical Chiropractic Care
1. Can chiropractic care cure ME/CFS? No. ME/CFS is a complex, multi-system illness with no single cause and no curative treatment in modern medicine. What upper cervical care can do is address the craniocervical mechanism that the 2020 Bragée research and other studies have identified as a substantial contributor in a significant subset of ME/CFS patients.
2. Is upper cervical chiropractic safe for ME/CFS patients? The Knee Chest Upper Cervical technique is exceptionally gentle and avoids the forceful manipulation that can trigger flares in sensitive patients. We also pace care thoughtfully for ME/CFS patients, recognizing that post-exertional malaise is real and that hypersensitive nervous systems benefit from slow, gentle care.
3. What is the connection between ME/CFS and the upper cervical spine? The 2020 Bragée study published in Frontiers in Neurology found that 50% of ME/CFS patients had hypermobility, 83% had signs of possible intracranial hypertension, and a substantial proportion had craniocervical obstructions. The upper cervical spine surrounds and protects the brainstem, where autonomic function, pain processing, and cerebrospinal fluid flow are all regulated.
4. Will an upper cervical adjustment trigger post-exertional malaise? This is a real concern for ME/CFS patients, and we take it seriously. The Knee Chest technique is significantly gentler than most chiropractic adjustments and is usually well tolerated. We start slowly, pace carefully, and watch for individual responses. Most ME/CFS patients tolerate the technique well.
5. What is the relationship between ME/CFS and craniocervical instability? For patients with significant ligamentous laxity (often related to hypermobile EDS), the upper cervical ligaments can be lax enough that the head moves abnormally on the neck, putting pressure on the brainstem. This is craniocervical instability, and it has been identified as a contributor to ME/CFS in a meaningful subset of patients. Severe cases may require surgical evaluation; many can be managed conservatively.
6. Should I see a chiropractor or a craniocervical surgeon? That depends on the severity of your situation. Most ME/CFS patients do not require surgery and benefit from a conservative approach to upper cervical care. For patients with severe instability, structural abnormalities on imaging, or progressive neurological deterioration, surgical evaluation at a specialized center may be appropriate. We can help you understand which path your situation calls for.
7. Will my ME/CFS doctor approve of chiropractic care? Most ME/CFS specialists are now familiar with the craniocervical literature and are open to upper cervical evaluation as part of a multidisciplinary approach. We encourage open communication with your treating physicians and do not ask patients to stop any other treatment.
8. How long does it take to see results? This varies enormously among ME/CFS patients. Some notice subtle changes in orthostatic tolerance, sleep, or brain fog within the first few weeks. Others experience more gradual or partial improvement over months. We give honest timelines based on your examination findings and what we observe along the way.
9. What if I also have POTS, EDS, or MCAS? That is extremely common in ME/CFS patients, and it does not change our willingness to work with you. In fact, the autonomic and craniocervical components common to these conditions are often particularly responsive to upper cervical care. We have meaningful experience with this patient population.
10. Is the post-COVID version of ME/CFS the same as classic ME/CFS? The clinical presentations overlap substantially, and many long COVID patients meet ME/CFS criteria. The underlying mechanisms may share some features (immune dysregulation, mitochondrial dysfunction, autonomic dysregulation) while differing in others. Upper cervical evaluation is potentially relevant for both populations.
11. Will I need to stop my medications? No. Continue all medications as prescribed by your treating physicians. Upper cervical care is complementary, not a replacement. If your medical team eventually wants to taper based on clinical improvement, that is a discussion for you and them.
12. Why have I never been told about the craniocervical connection? Because the research is relatively recent and most ME/CFS clinicians have not yet incorporated it into their evaluation. The Bragée 2020 paper is the most influential single contribution, and it is still working its way into mainstream practice. We are early adopters of this mechanism in our work, not outliers.
13. Can my fatigue really come from my neck? For a substantial subset of ME/CFS patients, yes — at least in part. The brainstem regulates so many functions (autonomic tone, sleep, pain modulation, cerebrospinal fluid flow) that compromising its mechanical environment produces wide-ranging symptoms that look exactly like ME/CFS. This is not the whole picture for every patient, but it is part of the picture for many.
14. How will I know if upper cervical care is right for me? The only way to know definitively is to come in for an evaluation. Our examination will identify whether your upper cervical findings are consistent with someone who is likely to benefit. If they are not, we will tell you that honestly.
15. How do I get started? Call our Sarasota office at (941) 243-3729 or book your consultation online. We will sit down with you, review your full history, perform a thorough examination, and give you a straight answer about whether upper cervical care is a good fit for your specific situation.
Take the Next Step Toward Recovery
ME/CFS is one of the most isolating, undertreated, and disbelieved illnesses in modern medicine. The patients who do best are the ones who build a broad multidisciplinary team, address the condition from multiple angles, and refuse to accept “we don’t know what to do for you” as the final answer. The craniocervical mechanism is one part of that broader picture — and for the substantial subset of ME/CFS patients whose illness is being driven, in meaningful part, by an unidentified upper cervical contributor, addressing it can shift the trajectory of the condition.
If you are in Sarasota, Bradenton, Lakewood Ranch, or anywhere in the surrounding region and you are carrying ME/CFS — diagnosed or suspected, mild or severe, recent or chronic — Dr. Rusty Lavender and Dr. Jacob Temple at Lavender Family Chiropractic are here to help you understand whether the upper cervical and craniocervical piece is the missing part of your healing puzzle. It will not solve everything. It may be one of the most important pieces nobody has yet offered you.
📞 Call (941) 243-3729 today to schedule your complimentary consultation 📅 Book online here 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield