By Dr. Rusty Lavender
Sciatica: Few pains command your attention like sciatica. It starts somewhere deep in the low back or buttock and then shoots — sharp, electric, burning — down the back of the leg, sometimes all the way to the foot. It can make sitting unbearable, standing exhausting, and sleeping nearly impossible. It flares when you cough or sneeze. It turns a simple drive across Sarasota into an ordeal. And for many people, it does not resolve quickly. It lingers, recurs, and slowly reshapes how they move, work, and live.
At Lavender Family Chiropractic in Sarasota, Florida, we want to be straightforward with you from the very first sentence, because honesty is the foundation of good care: sciatica is fundamentally a lower spine problem. The sciatic nerve originates from nerve roots in the lumbar and sacral spine, and the overwhelming majority of sciatica is caused by lumbar disc herniation, lumbar spinal stenosis, or other pathology in the lower back. We are an upper cervical practice. We do not claim that adjusting the top of your neck directly repairs a herniated disc at L5-S1. Any provider who tells you otherwise is overselling.
What we can tell you, and what this guide will explain in detail, is that the spine functions as a single connected system — mechanically, neurologically, and through the continuous membrane that surrounds the entire central nervous system. The alignment of the upper cervical spine influences the posture, the neural tension, and the nervous-system environment of the entire spinal column, including the lower back where your sciatica originates. For the right patients, addressing the upper cervical foundation can be a meaningful part of a whole-spine recovery strategy. This guide is for anyone in Sarasota, Bradenton, Lakewood Ranch, or the surrounding areas who wants to understand what sciatica really is, what the evidence says about conservative care, and where upper cervical care does — and does not — fit into the picture.
What Is Sciatica?
Sciatica is not a diagnosis in itself. It is a symptom — a description of pain that radiates along the path of the sciatic nerve, the largest nerve in the body. The sciatic nerve is formed from nerve roots that exit the lumbar and sacral spine (primarily L4 through S3), travels through the buttock and down the back of the thigh, and branches below the knee to supply the lower leg and foot. When one of these nerve roots, or the sciatic nerve itself, is compressed or irritated, the result is the radiating pain, numbness, tingling, or weakness that people call sciatica.
The classic presentation is unmistakable: pain that originates in the low back or buttock and shoots down one leg, often below the knee and sometimes into the foot. The pain is frequently described as sharp, burning, or electric, and is typically worse with lumbar flexion, sitting, twisting, bending, coughing, or sneezing. Patients may also experience numbness, pins-and-needles, or weakness in a specific dermatomal pattern that follows the affected nerve root. An L5 radiculopathy, for example, may produce weakness in the muscles that lift the foot and numbness across the top of the foot, while an S1 radiculopathy may affect the calf and the outer foot and diminish the ankle reflex.
The underlying causes are predominantly structural and predominantly lumbar. The most common cause by far is lumbar disc herniation — the soft inner material of a disc pushes outward and compresses or irritates a nearby nerve root. Approximately 90% of disc herniations occur at the L4-L5 or L5-S1 levels. Other causes include lumbar spinal stenosis (narrowing of the spinal canal, more common in older adults), spondylolisthesis (slippage of one vertebra on another), bone spurs, and, less commonly, piriformis syndrome (in which the piriformis muscle in the buttock irritates the sciatic nerve directly). Rare but serious causes include tumors, infections, and cauda equina syndrome — a surgical emergency that we screen for carefully.
How common is sciatica? It is one of the most prevalent pain conditions in the world. According to a review summarized in StatPearls, the lifetime incidence of sciatica is reported to be between 10% and 40%, with an annual incidence of 1% to 5%, and peak incidence occurring in the fourth decade of life. A 2007 review in the British Journal of Anaesthesiaestimated that between 13% and 40% of people will experience an episode of lumbar radicular pain during their lifetime. Prevalence estimates across studies vary widely — from as low as 1.6% to as high as 43% — largely due to differences in how studies define and measure sciatica. Whatever the precise figure, the takeaway is clear: sciatica affects an enormous portion of the population, and a substantial number of people in the Sarasota region are dealing with it at any given moment.
The good news, and it is important news for anyone facing this condition, is that most sciatica improves. The majority of acute sciatica episodes resolve substantially within weeks to a few months with conservative care. The challenge is the subset of cases that become chronic, recurrent, or intractable — and it is for these patients especially that a thorough, whole-spine approach matters.
The Spine Is One Connected System: The Dural and Postural Connection
To understand where upper cervical care fits into sciatica, you have to understand that the spine does not function as a stack of independent segments. It functions as a single, integrated, biomechanical and neurological system — and the connection runs deeper than most people realize.
The most important structural concept here is the dura mater. The dura is the tough, continuous membrane that surrounds and protects the entire central nervous system. It attaches at the top to the inside of the skull and to the upper cervical vertebrae — specifically with firm attachments at the foramen magnum, C1, C2, and C3 — and it runs as a continuous sleeve all the way down the spinal canal to its anchor at the sacrum. This is a single, unbroken membrane from the skull to the tailbone. Tension applied at one end is transmitted along its length.
This is the foundation of the work of Alf Breig, the Swedish neurosurgeon whose landmark research established the concept of adverse mechanical tension in the central nervous system. In his seminal 1978 book, Adverse Mechanical Tension in the Central Nervous System, Breig used cadaver, animal, and clinical material to demonstrate how tension and mechanical stress in the dura and spinal cord at one level of the spine produce effects transmitted throughout the entire neural axis — showing that the brain, brainstem, spinal cord, and nerve roots form a mechanically continuous system in which tension is propagated along the length of the cord and its membranes. Breig’s work became the foundation for the modern fields of adverse neural tension, neural mobilization, and clinical neurodynamics that physical therapists and manual practitioners use today.
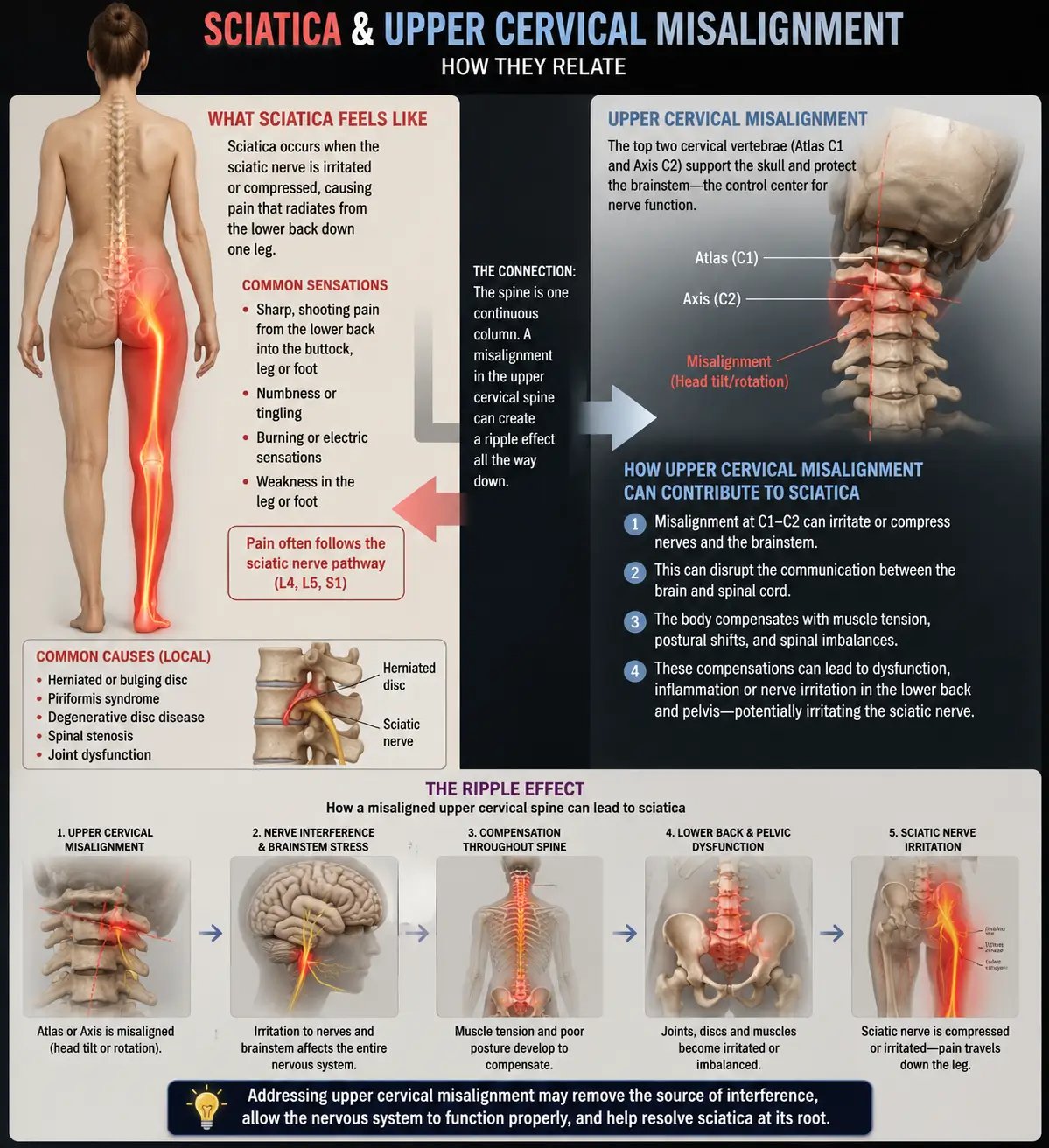
What does this mean practically? It means that when the upper cervical spine is misaligned — when the atlas and axis are not in proper position — the resulting changes in dural tension and spinal posture do not stay confined to the neck. The head shifts forward of the body’s center of gravity, the spine compensates with altered curves throughout its length, the dura experiences altered tension along its entire span, and the lumbar spine adapts to all of it. A chronic upper cervical misalignment is one of the inputs that determines how the whole spine is loaded, including the lumbar segments where sciatica originates.
There is also a postural dimension. The body’s righting reflexes work to keep the head level and the eyes oriented to the horizon. When the upper cervical spine is misaligned, the body produces a cascade of compensations down the entire spinal column to keep the head balanced — altering the position of the shoulders, the curve of the thoracic spine, the tilt of the pelvis, and the loading of the lumbar discs. Over years, these compensatory patterns contribute to the asymmetric loading that drives lumbar disc degeneration and creates the conditions for sciatica to develop.
We want to be careful and honest here, because this is exactly the kind of claim that is easy to oversell. The dural and postural connections are real and well-documented. They do not mean that an atlas adjustment is a substitute for addressing a significant lumbar disc herniation. What they mean is that the upper cervical spine is one legitimate, often-overlooked piece of the whole-spine picture — and that for patients whose sciatica is being perpetuated by global postural and neural-tension patterns, addressing the upper cervical foundation can be a meaningful part of a comprehensive strategy.
Where Upper Cervical Care Fits Into Sciatica Treatment
Let us be clear about our role. At Lavender Family Chiropractic, we are an upper cervical practice using the Knee Chest Upper Cervical technique — a precise, gentle method of correcting atlas and axis misalignments without twisting, popping, or forceful manipulation. We are not a substitute for the lumbar-focused care that many sciatica patients need, and we will tell you plainly when your situation calls for something we do not provide.
For the right sciatica patients, upper cervical care can contribute in several ways. First, by restoring proper upper cervical alignment, we reduce the abnormal dural tension and postural compensation patterns that propagate down the entire spine, which can reduce the global mechanical load on the lumbar spine. Second, upper cervical correction supports the autonomic nervous system and the body’s overall capacity to regulate inflammation, pain processing, and tissue healing — the environment in which an irritated nerve root either calms down or stays inflamed. Third, by improving whole-spine posture and balance, upper cervical care can help reduce the recurring strain patterns that cause sciatica to come back again and again in patients who have had multiple episodes.
It is also worth understanding what the broader chiropractic and manual therapy literature says about sciatica, because it is more encouraging than many patients have been led to believe. A landmark 2010 randomized controlled trial by McMorland and colleagues, published in the Journal of Manipulative and Physiological Therapeutics, compared spinal manipulation against surgical microdiskectomy in patients with sciatica from confirmed lumbar disc herniation who had failed at least three months of conservative care. The study found that 60% of patients who had failed other nonoperative treatment benefited from spinal manipulation to the same degree as if they had undergone surgical intervention — a remarkable finding suggesting that many surgical candidates may be able to avoid surgery with skilled manual care.
This does not mean upper cervical correction replaces lumbar care for sciatica. It means conservative, manual approaches to the spine have a strong evidence base, and that surgery should generally be reserved for the cases that genuinely require it. Our role is to evaluate the whole-spine picture, address the upper cervical component when it is relevant, and coordinate with other providers — including lumbar-focused chiropractors, physical therapists, and, when appropriate, surgeons — to give you the most complete care possible.
What Care Looks Like at Lavender Family Chiropractic
If you come to our Sarasota office for evaluation related to sciatica, here is what to expect, including an honest assessment of whether we are the right fit for your situation.
Your first visit begins with a thorough consultation. Dr. Lavender or Dr. Temple will sit down with you and review your full history — when the sciatica started, what triggered it, what makes it better or worse, the exact pattern of your pain and any numbness or weakness, what imaging you have had, and what treatments you have tried. We pay particular attention to red flags. If you have signs of cauda equina syndrome (loss of bowel or bladder control, saddle numbness, rapidly progressing weakness), profound or progressive neurological deficit, or other findings that suggest a surgical emergency or the need for immediate medical evaluation, we will tell you directly and help you get the right care immediately. Patient safety comes before everything else.
For appropriate patients, the examination includes a detailed neurological evaluation (reflexes, sensation, strength, nerve tension testing), postural and gait analysis, and advanced 3D imaging to assess your upper cervical alignment and overall spinal posture. We also perform functional nervous system scans to objectively measure how your nervous system is operating before care begins.
If the examination reveals an upper cervical component that is relevant to your whole-spine picture, we will explain honestly how upper cervical care fits into your overall recovery — and where it does not. We are direct about the fact that many sciatica patients will also benefit from lumbar-focused care, physical therapy, or other interventions, and we are happy to coordinate with those providers. We see ourselves as one part of your care team, not the whole of it.
Care is delivered through the gentle Knee Chest Upper Cervical technique. We offer customized treatment plans tailored to your specific situation, and we are transparent about expected timelines and what success looks like for your particular case.
📞 Call (941) 243-3729 to schedule your complimentary consultation 📅 Book your consultation online 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
What the Research Says About Sciatica and Conservative Care
The research on sciatica is extensive, and the dominant message is reassuring: most sciatica improves, conservative care should generally come first, and surgery is appropriate for a minority of cases.
The epidemiological foundation is well established. The StatPearls review documented that sciatica has a lifetime incidence between 10% and 40%, an annual incidence of 1% to 5%, and peak incidence in the fourth decade of life, with lumbar disc herniation being the most common cause. The 2007 British Journal of Anaesthesia review estimated the lifetime incidence of lumbar radicular pain at between 13% and 40%, noting that the majority of cases resolve with conservative measures but that a meaningful subset becomes chronic.
A 2026 observational study published in Frontiers on lumbar radiculopathy attributed to disc herniation reported an annual incidence of approximately 4.9 cases per 1,000 person-years with a lifetime risk of 3% to 5%, confirming lumbar disc herniation at the L4-S1 level as the most common cause and documenting measurable recovery of muscle strength over six months of treatment.
The most striking finding for patients hoping to avoid surgery comes from the 2010 McMorland randomized controlled trial in the Journal of Manipulative and Physiological Therapeutics. Among sciatica patients with confirmed lumbar disc herniation who had failed at least three months of nonoperative care and were surgical candidates, 60% benefited from spinal manipulation to the same degree as if they had undergone surgical microdiskectomy — and patients who did not respond to manipulation could subsequently undergo surgery with outcomes equivalent to those who had surgery first. This suggests that a trial of skilled manual care before surgery is reasonable for many patients.
The foundational mechanistic work remains Alf Breig’s Adverse Mechanical Tension in the Central Nervous System(1978), the neurosurgical text that established how mechanical tension is transmitted throughout the continuous dura and spinal cord — work reviewed in JAMA at the time as radical and revolutionary, and which became the basis for the modern fields of adverse neural tension and clinical neurodynamics. While Breig’s work is foundational theory rather than a clinical trial of upper cervical care for sciatica specifically, it provides the anatomical and biomechanical basis for understanding the spine as a single connected neural system.
This body of research does not establish that upper cervical chiropractic cures sciatica. What it establishes is that sciatica is largely a conservatively manageable condition, that manual approaches to the spine have meaningful evidence behind them, and that the whole-spine, continuous-dura model is well-founded.
Lifestyle Factors That Support Sciatica Recovery
Whether or not upper cervical care is part of your strategy, the daily inputs you control matter enormously for sciatica recovery. The patients who recover fastest and stay better longest are usually the ones who address these consistently.
Avoid prolonged sitting. Sitting increases intradiscal pressure in the lumbar spine more than standing or walking. Prolonged sitting — especially with poor posture — is one of the most common aggravators of sciatica. Get up and move every 30 minutes. If you have a desk job, alternate between sitting and standing.
Stay gently active. The old advice to rest in bed for sciatica has been thoroughly debunked. Prolonged bed rest worsens outcomes. Gentle, pain-respecting movement — walking, gentle mobility work, low-impact activity — supports circulation, reduces inflammation, and promotes healing. Move within the limits of your pain, but move.
Sleep position. Side sleeping with a pillow between the knees, or back sleeping with a pillow under the knees, takes pressure off the lumbar spine and irritated nerve roots. Avoid stomach sleeping, which extends the lumbar spine and can aggravate symptoms.
Anti-inflammatory eating. Nerve root irritation involves inflammation, and chronic systemic inflammation makes any nerve compression worse. Minimize processed foods, refined sugars, and seed oils; emphasize whole foods, healthy fats, omega-3-rich fish, and adequate protein. Omega-3 fatty acids and B vitamins support nerve health.
Hydration. The intervertebral discs are roughly 80% water, and chronic dehydration accelerates disc degeneration. In the Florida heat, this is especially important. Aim for at least half your body weight in ounces of water daily.
Smoking cessation. If you smoke, this is one of the most important things you can do. Smoking is a well-documented risk factor for disc degeneration and impairs disc healing by constricting the small blood vessels that supply the surrounding tissue.
Weight management. Excess body weight increases mechanical load on the lumbar spine. Even modest weight reduction can meaningfully reduce lumbar disc pressure.
Core and hip strength. Once you are past the acute flare, gradually building core stability and hip strength helps support the lumbar spine and reduce recurrence. Work with a qualified physical therapist or trainer who understands spinal conditions.
Avoid heavy lifting and twisting during flares. During an active sciatica episode, avoid heavy lifting, forward bending with rotation, and any movement that reproduces sharp radiating pain. These can worsen disc pathology.
If you found this guide useful, you may also want to read our blog on pinched nerve in the neck (cervical radiculopathy)— the cervical-spine equivalent of sciatica, which shares many of the same nerve-compression mechanisms and conservative care principles.
Serving Sarasota and the Surrounding Communities
Lavender Family Chiropractic is located in Sarasota, Florida, at 5899 Whitfield Avenue, Suite 107 — at the corner of University and Whitfield. From this central location, we serve patients throughout the region, including Bradenton, Lakewood Ranch, Palmetto, Parrish, Venice, Osprey, Nokomis, Ellenton, Ruskin, Myakka City, North Port, and the greater Tampa Bay area. Patients also travel from St. Pete, Riverview, and Manatee County to receive specialized upper cervical care here.
Sciatica is one of the most common reasons people seek out chiropractic care, and we want to be the practice that gives you a straight, honest assessment of where upper cervical care fits into your recovery and where it does not. If you are looking for that kind of transparency, we encourage you to reach out.
Top 15 FAQs About Sciatica and Upper Cervical Chiropractic Care
1. Can upper cervical chiropractic fix my sciatica? We want to be honest: upper cervical care does not directly repair a herniated lumbar disc. Sciatica is fundamentally a lower spine problem. What upper cervical care can do is address the whole-spine postural and dural-tension patterns that influence how your lumbar spine is loaded, as one part of a comprehensive strategy. For many patients, lumbar-focused care is also needed, and we will tell you that honestly.
2. Why would the top of my neck affect pain in my leg? Because the spine functions as one connected system. The dura — the membrane surrounding the spinal cord — is continuous from the skull to the sacrum, and tension is transmitted along its length. Upper cervical misalignment also drives postural compensations down the entire spine that affect how the lumbar discs are loaded. This is whole-spine influence, not a direct fix of the lumbar problem.
3. What actually causes sciatica? The most common cause is lumbar disc herniation, accounting for roughly 90% of cases, typically at the L4-L5 or L5-S1 levels. Other causes include lumbar spinal stenosis, spondylolisthesis, bone spurs, and piriformis syndrome. Rare serious causes include tumors, infections, and cauda equina syndrome.
4. Will my sciatica go away on its own? Most acute sciatica improves substantially within weeks to a few months with conservative care. The challenge is the subset that becomes chronic or recurrent. Even when sciatica resolves on its own, addressing the underlying biomechanical patterns can help reduce recurrence.
5. When is sciatica a medical emergency? Seek immediate medical care if you experience loss of bowel or bladder control, numbness in the saddle region (inner thighs, groin, buttocks), or rapidly progressing leg weakness. These can indicate cauda equina syndrome, a surgical emergency. We screen for these red flags carefully and will direct you to emergency care if needed.
6. Do I need surgery for sciatica? Most people do not. Surgery is generally reserved for cases with progressive neurological deficit, cauda equina syndrome, or intractable pain that has not responded to several months of conservative care. The 2010 McMorland study found that 60% of surgical candidates benefited from spinal manipulation as much as from surgery.
7. Is upper cervical care safe if I have a herniated disc? The Knee Chest Upper Cervical technique is exceptionally gentle and does not apply force to the lumbar spine at all. It is generally very safe. We perform a thorough examination, screen for red flags, and coordinate with other providers for the lumbar component of your care.
8. Should I see an upper cervical chiropractor or a regular chiropractor for sciatica? It depends on your situation. Many sciatica patients benefit from lumbar-focused chiropractic care, physical therapy, or both. Upper cervical care addresses the whole-spine and dural-tension component. We are honest about which approach, or combination, is likely to serve you best, and we coordinate with other providers.
9. How long does conservative care take to work for sciatica? Many patients see meaningful improvement within weeks. Chronic or recurrent cases may take longer. We provide honest timelines based on your specific examination findings.
10. Can stress make sciatica worse? Yes. Chronic stress increases muscle tension, lowers pain thresholds, and raises systemic inflammation — all of which can worsen nerve root irritation. Stress management is an underrated part of recovery.
11. Is sitting really that bad for sciatica? Sitting increases lumbar disc pressure more than standing or walking, and prolonged sitting is one of the most common aggravators of sciatica. Frequent movement breaks and alternating between sitting and standing help significantly.
12. Can a car accident cause sciatica? Yes. Trauma from motor vehicle accidents can cause lumbar disc herniation and other lumbar injuries that lead to sciatica. Our car accident chiropractic care addresses spinal injuries from collisions, including the whole-spine assessment that trauma patients need.
13. Will an MRI tell me what is causing my sciatica? MRI is valuable for identifying disc herniation, stenosis, and other structural causes, and for ruling out serious pathology. However, MRI findings do not always correlate perfectly with symptoms — many people have disc bulges on imaging without any pain. A complete evaluation combines imaging with clinical examination.
14. How will I know if upper cervical care is right for me? The only way to know is a thorough evaluation. We will assess your whole-spine picture, screen for red flags, and give you an honest assessment of whether upper cervical care is likely to help your specific situation — and whether you also need lumbar-focused or other care.
15. How do I get started? Call our Sarasota office at (941) 243-3729 or book your consultation online. We will review your history, perform a thorough examination, screen for any red flags, and give you a straight answer about how upper cervical care fits into your recovery.
Take the Next Step Toward Relief
Sciatica is one of the most common and most disruptive pain conditions there is — and the encouraging truth is that most of it improves with conservative care, and that surgery is necessary for only a minority of cases. The patients who recover best are the ones who address the condition comprehensively: the lumbar source of the problem, the whole-spine postural and neural-tension patterns that influence it, and the daily lifestyle factors that either support or sabotage healing.
If you are in Sarasota, Bradenton, Lakewood Ranch, or anywhere in the surrounding region and you are dealing with sciatica, Dr. Rusty Lavender and Dr. Jacob Temple at Lavender Family Chiropractic are here to give you an honest evaluation of where the upper cervical and whole-spine piece fits into your recovery. We will tell you straight what we can help with, what we cannot, and how to build the most complete path forward.
📞 Call (941) 243-3729 today to schedule your complimentary consultation 📅 Book online here 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield