By Dr. Rusty Lavender
Ear Tubes in Children: If you are a parent in Sarasota whose child keeps getting ear infections, or who has fluid behind the eardrum that won’t clear, or who has been recommended for ear tubes, you are facing one of the most common and most stressful decisions of early childhood. You want to do right by your child, you don’t want them in pain or missing out on hearing and speech, and you also don’t want to rush into surgery if it isn’t necessary. It is a genuinely hard decision, and it deserves clear, honest information.
We want to be direct with you from the very first paragraph, because when it comes to children’s health, honesty matters more than anything: this is fundamentally a medical decision, and the people best equipped to guide it are your pediatrician and a pediatric ENT. Upper cervical chiropractic care is not a treatment for ear infections, it is not a substitute for medical evaluation, and it is never a reason to delay care your child genuinely needs. We are writing this guide to help you understand what is actually going on, what the medical guidelines say, and where, if anywhere, our kind of care might fit as one supportive piece, always alongside proper medical care, never instead of it.
At Lavender Family Chiropractic in Sarasota, Florida, we focus on the upper cervical spine using gentle, child-appropriate methods. But our most important role with a child who has ear problems is often simply this: helping you understand the picture clearly and making sure your child gets the right care from the right providers.
Ear Tubes in Children and Why Children Get Eustachian Tube Dysfunction So Often
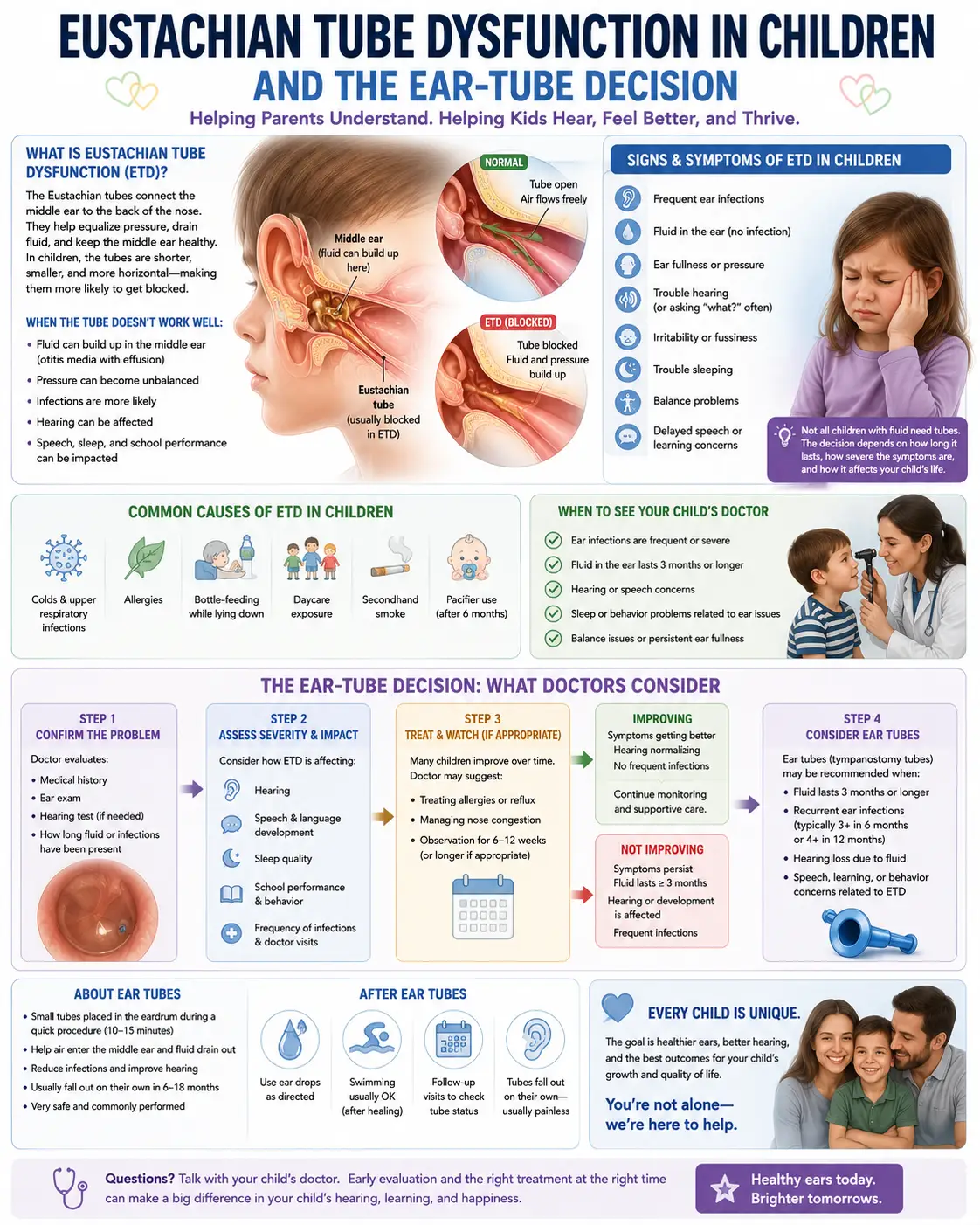
Ear problems are nearly a rite of passage in early childhood, and there is a real anatomical reason. The Eustachian tube connects the middle ear to the back of the nose and throat, ventilating the middle ear and equalizing pressure. In young children, this tube is shorter, narrower, and much more horizontal than in adults. That flatter angle makes it far less efficient at draining fluid and clearing infection, so fluid and germs get trapped behind the eardrum more easily.
This is why ear infections are so common in this age group. As the clinical guidelines note, children younger than seven are at increased risk of middle ear problems because of their immature immune systems and the poor function of the still-developing Eustachian tube. Otitis media, inflammation of the middle ear, is second only to the common cold as the most frequent illness diagnosed in children. The good news embedded in this: most children simply outgrow it as the tube lengthens, steepens, and matures with age.
A few terms help make sense of what a doctor may tell you. Acute otitis media (AOM) is an active middle ear infection with pain and often fever. Otitis media with effusion (OME) is fluid behind the eardrum without an active infection, the “glue ear” or lingering fluid that can muffle hearing. Both are tied to how well, or poorly, the Eustachian tube is doing its job.
What the Medical Guidelines Actually Say
Here is where parents most need clear information, because the medical guidelines are more measured, and more reassuring, than the anxiety around this decision often suggests. The American Academy of Otolaryngology–Head and Neck Surgery Foundation publishes the authoritative guidelines on ear tubes, and they emphasize watchful waiting and careful selection over rushing to surgery.
Watchful waiting comes first. For an otherwise healthy child with fluid behind the eardrum, the guideline summarized by the American Academy of Family Physicians is clear: tympanostomy tubes should not be used in children with a single episode of otitis media with effusion of less than three months’ duration, because OME is often self-limited following a cold or ear infection, and a three-month observation period helps distinguish fluid that will clear on its own from fluid that won’t. In other words, most fluid clears by itself, and the guidelines specifically advise against premature surgery.
When tubes are genuinely indicated. Tubes become appropriate when the problem persists and is affecting the child. The guidelines indicate that bilateral tubes should be offered when a child has fluid in both ears for three months or longer along with documented hearing difficulties, because the chance of spontaneous resolution is low once bilateral OME persists past three months. Tubes may also be considered for persistent fluid accompanied by symptoms like balance problems, poor school performance, behavioral issues, or ear discomfort.
The “at-risk child” is different. The guidelines carve out children who are at increased risk for speech, language, or learning problems, including those with existing developmental, hearing, or other conditions. These children warrant prompter evaluation and a lower threshold for intervention, because for them, even fluid that might be tolerated in another child can interfere with critical development.
It’s a shared decision. Crucially, the guidelines frame tube placement as a shared decision between the physician and the parents, weighing the natural history, the benefits and risks of the procedure, and the alternatives. You are meant to be an informed partner in this, not a bystander.
One more thing parents should know, because it surprises many: the guidelines actually recommend against using antihistamines, decongestants, oral steroids, or routine antibiotics to treat OME, because these have not been shown to help the fluid clear and carry their own downsides. If you’ve been giving these and they haven’t worked, that is consistent with what the evidence predicts.
Why Hearing Matters So Much in This Decision
The reason doctors take persistent fluid seriously, and the reason we will never tell you to ignore it, is hearing. Fluid behind the eardrum can cause a temporary, conductive hearing loss, muffling sound during exactly the years when a child is learning to talk and understand language. When this goes on long enough during a critical developmental window, it can contribute to delays in speech, language, and learning.
This is the heart of why the ear-tube decision exists, and why we hold the line on it so firmly. Tubes work by ventilating the middle ear directly, draining the fluid and restoring normal hearing, which removes that barrier to development. For a child with genuine, persistent fluid and hearing difficulty, that benefit is real and important. No alternative approach, including ours, should ever be used as a reason to leave a hearing-impairing effusion untreated. If your child has persistent fluid, getting their hearing tested, as the guidelines advise for OME lasting three months or more, is one of the most important steps you can take.
A Useful, Low-Risk Option During Watchful Waiting
If your child is in the watchful waiting window and you want to do something constructive while you wait to see whether the fluid clears, there is a simple, evidence-supported, low-risk option worth asking your doctor about: nasal balloon autoinflation.
This involves having the child gently inflate a small balloon through the nose, which helps open the Eustachian tube and encourage the middle ear to clear. It is low-cost, has essentially no adverse effects, and has shown benefit in helping clear middle ear fluid and improve symptoms in school-aged children during the watchful waiting period. It tends to work better in older children who can perform it reliably. We mention it not because it’s something we provide, but because it’s a genuinely useful, doctor-endorsed tool that many parents have never heard of, and it fits squarely within the watchful-waiting approach the guidelines recommend.
Where Upper Cervical Care May, and May Not, Fit
Now to the honest question many parents arrive with: does chiropractic help children’s ear problems? We’re going to answer this carefully, because your child’s wellbeing matters far more than promoting what we do.
The honest answer is that the evidence for chiropractic care affecting pediatric ear infections is limited and largely based on case reports and small studies, not the kind of large, high-quality trials that establish a treatment works. We will not tell you that adjustments cure or prevent ear infections, because the evidence does not support that claim, and your child deserves better than overstatement.
What can be said, modestly, is this. The muscles that open and coordinate the Eustachian tube are controlled by cranial nerves, and the tensor veli palatini, a key tube-opening muscle, shares its nerve supply with the muscles of the jaw, as documented in the clinical literature on tube function. The upper cervical spine sits adjacent to the brainstem where these nerve pathways travel. The theory behind upper cervical care for ear issues is that supporting healthy nerve function and muscle tone in this region, along with drainage, might help some children. That is a reasonable mechanistic idea, and some parents report improvement, but it remains a complementary consideration, not a proven treatment, and not a substitute for the medical pathway above.
So here is our genuine position. If you bring your child to us, our first job is to make sure they are on the right medical track: that fluid is being monitored, that hearing is being checked when it should be, and that you’re connected with your pediatrician and an ENT as needed. If, alongside that, you want a gentle upper cervical evaluation to see whether structural and neurological factors might be a supportive piece, we’re glad to provide it, framed honestly and tracked for whether it actually helps. What we will never do is position our care as a reason to skip or delay tubes or medical evaluation your child needs.
What Care Looks Like for a Child at Lavender Family Chiropractic
If you bring your child to our Sarasota office, here is what to expect.
We start with a thorough conversation about your child’s history: how many ear infections, how often, whether fluid lingers, any concerns about their hearing or speech, what your pediatrician has said, and whether tubes have been recommended. We ask about the red and yellow flags that mean a child needs prompt medical attention, and if your child’s picture calls for it, our recommendation will simply be to ensure they’re seen and managed by their pediatrician and a pediatric ENT. We see ourselves as part of a team that has your child’s doctors at its center.
For children for whom a gentle evaluation is appropriate, our methods are tailored to be safe and comfortable for a child, with no forceful twisting or cracking. We are transparent with you about what we’re assessing and what we realistically can and cannot contribute. And we keep the focus where it belongs: on your child’s hearing, comfort, and development, in coordination with their medical care.
We’re also here simply as a knowledgeable, honest sounding board. If you’re overwhelmed by the tube decision and want help understanding what the guidelines mean for your specific situation, that conversation alone is something we’re glad to offer, while always pointing you back to your child’s doctors for the medical decision itself.
📞 Call (941) 243-3729 to schedule a consultation 📅 Book online 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
When Your Child Needs Prompt Medical Attention
This deserves its own section, because nothing matters more. Please seek medical care, not chiropractic care, for these:
A child in significant ear pain, or with fever, especially a young infant, needs to be seen by a pediatrician. Any concern that your child isn’t hearing well, isn’t responding to sounds, or whose speech seems delayed needs prompt medical and hearing evaluation. Fluid or infections that persist or keep recurring need ongoing pediatric and ENT management. Drainage from the ear, severe pain, or a very sick-appearing child needs prompt medical attention. And children with existing developmental, hearing, or craniofacial conditions, including Down syndrome and cleft palate, need close, specialist-guided monitoring, because their ear and hearing risks are higher.
We say all of this plainly because a guide like this should make your child safer, never give anyone a reason to delay care they need.
Serving Sarasota Families and the Surrounding Communities
Lavender Family Chiropractic is located in Sarasota, Florida, at 5899 Whitfield Avenue, Suite 107, at the corner of University and Whitfield. We serve families throughout Sarasota, Bradenton, Lakewood Ranch, Palmetto, Parrish, Venice, Osprey, and the surrounding Gulf Coast communities.
If you’re navigating a child’s ear problems or the tube decision and want an honest conversation, including honesty about when the answer is squarely medical, we’re glad to help your family think it through.
Top 15 FAQs About Childhood ETD and the Ear-Tube Decision
1. Why does my child get so many ear infections? Young children’s Eustachian tubes are shorter, narrower, and more horizontal, so they drain poorly and trap fluid and germs more easily. Combined with developing immune systems, this makes ear infections very common, and most children outgrow them as the tube matures.
2. Will my child grow out of this? Usually, yes. Most ear infections and fluid resolve as children grow and the Eustachian tube lengthens and steepens. The tube-decision exists for the cases where problems persist long enough to affect hearing or development.
3. What’s the difference between an ear infection and fluid? An ear infection (acute otitis media) is active and painful, often with fever. Fluid (otitis media with effusion) is fluid behind the eardrum without active infection, sometimes called “glue ear,” which can linger and muffle hearing after an infection clears.
4. Should we wait or get tubes? For an otherwise healthy child, guidelines recommend watchful waiting for about three months, since most fluid clears on its own. Tubes become appropriate mainly when fluid persists in both ears for three months or more with hearing difficulty. It’s a shared decision with your child’s doctor.
5. When are tubes really necessary? Generally when fluid persists past three months in both ears with documented hearing loss, or when persistent fluid causes symptoms like balance, behavior, or school problems, or for children at higher developmental risk. Your ENT will assess this.
6. Are decongestants or antibiotics the answer instead? For lingering fluid (OME), guidelines actually recommend against antihistamines, decongestants, steroids, and routine antibiotics, because they haven’t been shown to clear the fluid. This surprises many parents who’ve been trying them.
7. Is there something low-risk we can do while we wait? Ask your doctor about nasal balloon autoinflation. It’s low-cost, essentially without side effects, and has evidence for helping clear middle ear fluid in school-aged children during watchful waiting. It works best in kids old enough to do it reliably.
8. Can chiropractic cure my child’s ear infections? No, and we won’t claim it can. The evidence is limited and mostly case-based. We don’t treat infections, and we’d never position our care as a substitute for the medical evaluation and treatment your child may need.
9. Then why would we see you at all? Mainly so we can help make sure your child is on the right medical track, and, if you wish, provide a gentle upper cervical evaluation as a complementary piece. A lot of our value is honest guidance and making sure nothing important gets missed.
10. Is chiropractic safe for a child? When appropriate and done with child-suitable, gentle methods, with no forceful twisting or cracking, it’s intended to be safe and comfortable. But for ear infections specifically, we always keep your child’s pediatrician and ENT at the center of care.
11. Why is everyone so concerned about hearing? Because fluid can cause temporary hearing loss during the years a child is learning language, which can contribute to speech and learning delays. That developmental window is exactly why persistent fluid is taken seriously and why hearing should be tested if it lasts three months or more.
12. My child has Down syndrome (or cleft palate). Is this different? Yes. These children have much higher rates of ear fluid and hearing issues and need close, specialist-guided monitoring and often earlier intervention. Please work with a pediatric ENT and your care team; this is firmly a medical pathway.
13. Are tubes a big deal? Tube placement is a common, generally safe procedure done under brief general anesthesia, and tubes usually fall out on their own within about a year. Like any procedure it has risks and considerations, which your ENT will review with you as part of a shared decision.
14. What if I’m just not sure what to do? That’s completely normal, it’s a hard decision. Get your child’s hearing tested if fluid has lasted three months or more, have a frank shared-decision conversation with your ENT about benefits and alternatives, and take the time the watchful-waiting window gives you.
15. How do we get started with you? Call our Sarasota office at (941) 243-3729 or book online. We’ll listen to your child’s history, help you understand the picture and the guidelines, make sure you’re connected with the right medical care, and discuss whether a gentle evaluation has anything to add.
Take the Next Step
The childhood ear-tube decision feels enormous because you’re trying to protect your child’s hearing and development while not over-treating. The reassuring truth is that most childhood ear problems resolve on their own, the medical guidelines are thoughtfully built around watchful waiting and careful selection, and when tubes are truly needed, they help. Your pediatrician and ENT are your essential guides, and a hearing test for persistent fluid is one of the most valuable steps you can take.
If you’d like an honest, informed conversation about your child’s situation, including straight talk about when the answer is purely medical and where, if at all, gentle upper cervical care might add support, Dr. Rusty Lavender and Dr. Jacob Temple at Lavender Family Chiropractic are here for Sarasota families.
📞 Call (941) 243-3729 today 📅 Book online here 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield