By Dr. Rusty Lavender
Dilatory (Obstructive) Eustachian Tube Dysfunction Relief and Treatment in Sarasota: Some people only feel their ears during a flight or a storm. This guide is about the other pattern, the one where your ears feel clogged, full, or muffled much of the time, and the relief you keep waiting for never quite comes. You yawn, you swallow, you try to make them “pop,” and maybe they clear for a moment before the heaviness settles back in. Sounds feel distant, like you are hearing through cotton or from underwater. This persistent, day-to-day version of ear fullness has a specific name: dilatory Eustachian tube dysfunction, also called obstructive ETD.
Dilatory ETD is the most common form of Eustachian tube dysfunction, and it is fundamentally a problem of a tube that will not open well enough, often enough, to keep your middle ear properly ventilated. It is different from the baro-challenge type, where the ears only act up during pressure changes; with dilatory ETD, the difficulty is present under ordinary, everyday conditions. If you have spent months cycling through decongestants, antihistamines, and nasal sprays without lasting relief, the obstructive nature of this type is part of why.
At Lavender Family Chiropractic in Sarasota, Florida, our entire focus is the upper cervical spine, the atlas (C1) and axis (C2) at the very top of the neck. We use 3D CBCT imaging and paraspinal infrared thermography to understand how your upper neck is influencing the nerves and muscles that control your ears, and we correct upper cervical misalignment with the gentle, precise Knee Chest Upper Cervical technique, with no twisting, popping, or forceful manipulation. We want to be honest from the start: we do not treat infections, and we are not a substitute for medical evaluation of the inflammation and congestion that frequently drive this condition. What we can do is help address one specific and often-overlooked piece, the neuromuscular coordination that opens the tube, which is influenced by the upper neck.
What Is Dilatory (Obstructive) Eustachian Tube Dysfunction?
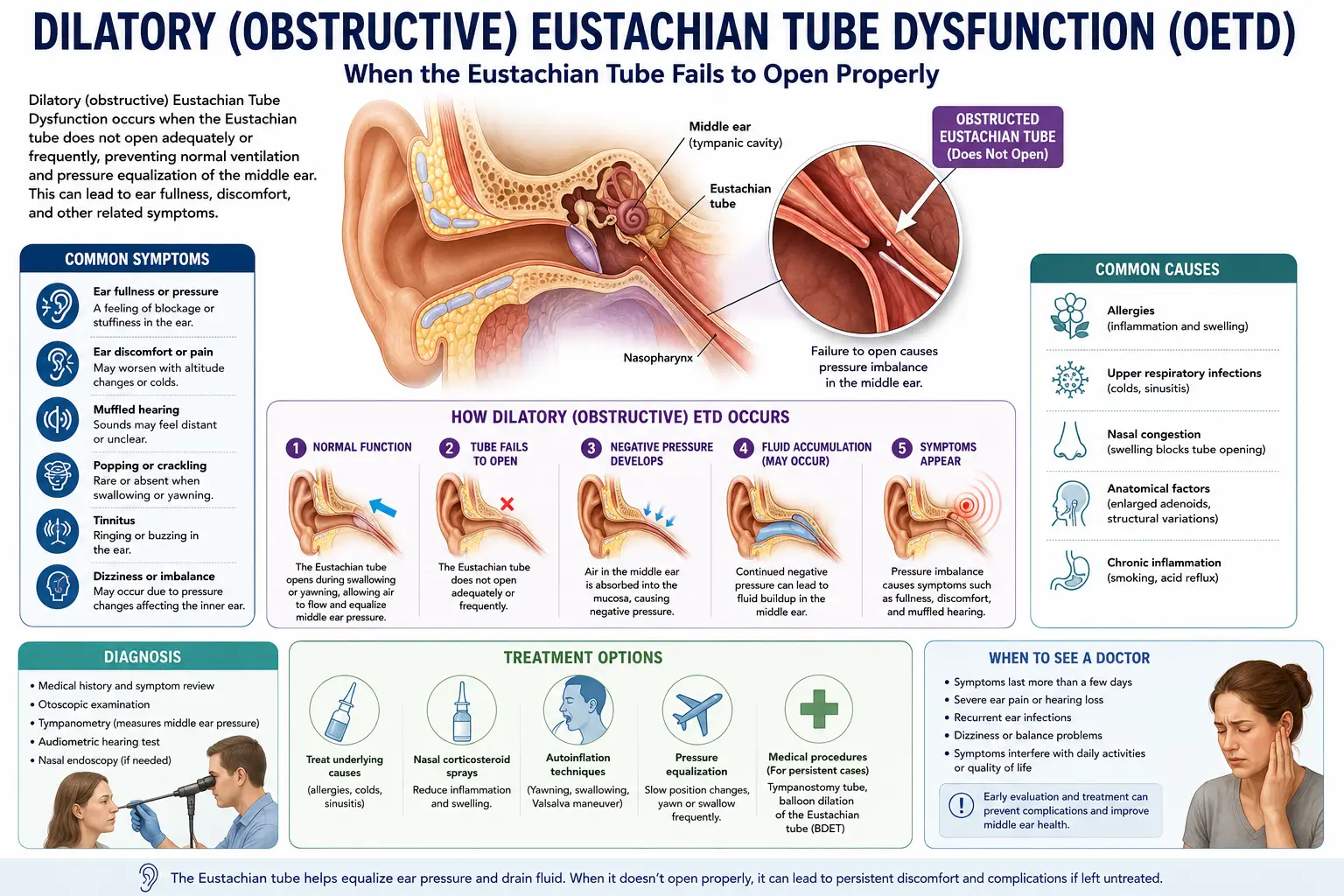
The Eustachian tube is a narrow canal connecting your middle ear to the back of your nose and throat. Its job is to equalize air pressure on both sides of the eardrum, ventilate the middle ear, and let fluid drain. It is normally closed, and it opens briefly, an active event driven by small muscles, each time you swallow, yawn, or chew.
Dilatory ETD is the failure of that opening. The word “dilatory” refers to dilation, the opening of the tube. In dilatory dysfunction, the tube’s dilatory effort is consistently insufficient to adequately aerate the middle ear. The tube does not open well enough or often enough, so the middle ear cannot stay properly ventilated. The result is negative pressure building behind the eardrum, fluid that does not drain, and the familiar symptoms: persistent ear fullness or pressure, muffled or “underwater” hearing, popping and crackling that does not fully clear, and sometimes a sense of imbalance or mild tinnitus.
This is the most common type of Eustachian tube dysfunction in clinical practice. It is also the type most associated with downstream middle ear problems when it becomes chronic, because a middle ear that stays poorly ventilated and full of fluid is set up for issues like fluid behind the eardrum and recurrent ear problems. As the Cleveland Clinic notes, Eustachian tube dysfunction is most common in young children, in large part because their tubes are smaller, flatter, and more prone to this obstructive pattern, though it affects adults too.
The crucial contrast with baro-challenge-induced ETD, which we cover in a separate guide, is timing. In baro-challenge ETD, the tube works acceptably at rest and only fails during rapid pressure changes like flying or diving, with a normal exam in between. In dilatory ETD, the difficulty is present under ordinary conditions, so the symptoms are more constant and the exam is more likely to show signs like negative middle ear pressure or eardrum retraction.
The Three Subtypes: Functional, Dynamic, and Anatomical
Not all dilatory ETD is the same, and the distinction matters because it shapes what is actually wrong and what is likely to help. Clinicians divide dilatory dysfunction into three subtypes.
Functional obstruction is the most common and, for our discussion, the most important. Here the tube is structurally normal and open-able, there is no physical blockage, but it fails to open effectively when you swallow or yawn. A 2025 review on the mechanisms of ETD describes functional obstruction precisely: it occurs when the Eustachian tube is structurally patent but fails to open effectively during physiologic maneuvers such as swallowing or yawning, with neuromuscular dysfunction of the tensor veli palatini and levator veli palatini muscles, or inhibitory influences from inflammatory conditions like allergic rhinitis and reflux, as common contributors. Read that carefully, because it is the heart of the matter: functional obstruction is, in significant part, a neuromuscular problem, the muscles that should open the tube are not doing their job effectively. That is precisely the kind of dysfunction that has a plausible connection to the nervous system and the upper neck.
Dynamic dysfunction, sometimes called muscular failure, overlaps with functional obstruction and refers to the active opening mechanism itself underperforming, the muscular effort to dilate the tube being inadequate or poorly coordinated.
Anatomical obstruction is a physical blockage somewhere in the system, a genuine structural cause. This can include a mass or enlarged tissue, such as enlarged adenoids in children, scarring, or, rarely, a tumor in the nasopharynx. This subtype is important to recognize because it is the one most likely to require medical or surgical attention, and because a persistent, one-sided obstruction in an adult always warrants a proper ENT evaluation to rule out serious causes. We take this seriously and will direct you to the right specialist when the picture calls for it.
Understanding which subtype is in play is part of why a careful evaluation matters, and why no one should assume all chronic ear fullness has the same cause.
What Drives the Obstruction: Inflammation and Congestion
For most people with dilatory ETD, especially the functional and dynamic kinds, the engine of the problem is inflammation and congestion in the lining of the tube and the nasopharynx around it. The mucosa, the moist lining, of the Eustachian tube is continuous with the lining of the nose and sinuses, so whatever inflames the nose tends to inflame the tube.
The usual drivers are familiar to anyone who has lived through a Florida allergy season. According to clinical references, the physiological causes of dilatory ETD involve inflammation and mucosal swelling from rhinitis, upper respiratory infections (colds), and reflux, which lead to blockage of the tube and dysfunction. Allergic rhinitis, chronic rhinosinusitis, laryngopharyngeal reflux, and exposure to tobacco smoke are repeatedly identified as the most common contributors. When the lining swells, the tube cannot open and clear the way it should, and the obstructive cycle sets in.
This is also why the standard first-line treatments, decongestants, antihistamines, nasal steroids, target inflammation, and why they often help, at least partially. But it is also why relief can be incomplete or short-lived: if part of the problem is the neuromuscular coordination of tube opening rather than inflammation alone, addressing only the inflammation leaves a piece unaddressed. That gap is exactly where we believe the upper neck deserves consideration.
The Upper Cervical Connection: The Muscles That Open the Tube
Here is where the obstructive story connects to what we do. The tube does not open passively; it is actively opened by two small muscles, the tensor veli palatini, the primary opener, and the levator veli palatini. When functional obstruction is the problem, it is precisely these muscles failing to open the tube effectively, the neuromuscular dysfunction the research describes.
These muscles are controlled by cranial nerves. The tensor veli palatini shares its nerve supply, the mandibular branch of the trigeminal nerve, with the muscles of the jaw. Physiopedia’s review notes that because the trigeminal nerve supplies both the muscles of mastication and the tensor veli palatini, addressing the TMJ and associated structures can simultaneously influence signaling to the muscles that control the Eustachian tube. The coordination and tone of the muscles that open the tube is a nervous-system function, and that is the bridge to the upper cervical spine.
The atlas and axis sit immediately beneath the skull, adjacent to the brainstem, where many of the cranial-nerve pathways governing these muscles travel and relay. The region is also one of the most proprioceptively dense in the body, heavily influencing the tone and coordination of nearby muscles. The reasoning, and our clinical experience, is that when the atlas or axis is misaligned, it may alter the neural input and muscle tone serving the tube-opening muscles, contributing to the ineffective, poorly-timed opening that defines functional dilatory ETD.
There is also an autonomic and congestion dimension that ties the two halves of the problem together. The upper cervical region influences autonomic balance, which affects blood vessel tone and mucosal congestion in the nasopharynx, the very inflammation-and-swelling that drives obstruction. And because the jaw and the tube share trigeminal wiring, people who clench, grind, or have TMJ dysfunction may have further-compromised tube coordination.
We want to be careful and honest, because this is an area ripe for overpromising. The anatomy, that the tube is opened by specific muscles, that those muscles are controlled by cranial nerves traveling near the upper cervical spine, that functional obstruction is substantially a neuromuscular failure, is well-documented. What is not established by large clinical trials is the degree to which correcting upper cervical alignment improves dilatory ETD. Our honest position is that there is a sound, mechanism-based rationale for addressing the upper neck as one part of the picture, alongside appropriate management of the inflammation and congestion, and many patients report meaningful improvement, while high-quality outcome evidence is still developing.
Why Upper Cervical Care Matters for Dilatory ETD
At Lavender Family Chiropractic in Sarasota, our approach to dilatory ETD is built around the part of the problem that the standard inflammation-focused treatments do not address: the neuromuscular coordination of tube opening. Through the Knee Chest Upper Cervical technique, we correct atlas and axis misalignment with a precise, gentle, sub-millimeter adjustment, with no twisting, cracking, or forceful manipulation.
For someone with chronic, obstructive ear fullness, restoring proper upper cervical alignment aims to support healthier neural input to the tensor veli palatini and levator veli palatini, so they can open the tube more effectively and consistently. It aims to support better autonomic balance and reduced congestion in the nasopharynx, addressing the inflammatory side of the obstruction. And by easing skull-base tension and improving jaw mechanics, it addresses the shared trigeminal pathways linking the jaw to the tube.
The goal is not to claim we cure ETD or replace medical care for the inflammation that often drives it. The goal is to address an overlooked, neuromuscular contributor, in coordination with whatever allergy, reflux, or sinus management your situation calls for. We see ourselves as one part of a complete approach. What separates upper cervical care from a generic adjustment is the precision of the diagnosis and the specificity and gentleness of the correction, which matters especially when the tube and surrounding tissues are already irritated.
What Care Looks Like at Lavender Family Chiropractic
If you come into our Sarasota office for chronic, obstructive ear fullness, here is what to expect.
Your first visit begins with a thorough consultation. Dr. Lavender or Dr. Temple will review your full history: how long your ears have been clogged, whether it is constant or fluctuating, your history of allergies, sinus issues, colds, and reflux, any jaw clenching or grinding, and what treatments you have already tried. We pay close attention to red flags. A persistent, one-sided blockage, especially in an adult, or any sign pointing to an anatomical cause, prompts us to refer you for ENT evaluation, because the anatomical subtype of dilatory ETD can occasionally signal something that needs medical attention. Patient safety comes first, always.
For appropriate patients, the examination includes advanced 3D CBCT imaging of your upper cervical spine, postural and range-of-motion assessment, and functional nervous system scans using paraspinal infrared thermography. This lets us see how the atlas and axis are influencing the nerves and muscle tone serving your ears, jaw, and sinuses, and base recommendations on your specific anatomy rather than guesswork.
For patients who are appropriate candidates, care is delivered through the gentle Knee Chest Upper Cervical technique, with no popping or twisting. We offer customized treatment plans tailored to your situation, and we pair corrections with simple home strategies for swallowing mechanics, posture, hydration, and managing congestion. We monitor objective scans and clinical changes over time rather than adjusting and hoping, and we are honest about realistic timelines, some people notice changes in ear fullness within a few weeks, while for others gains build more gradually as alignment stabilizes. We also coordinate openly with your other providers, because dilatory ETD is often best addressed from more than one angle at once.
📞 Call (941) 243-3729 to schedule your consultation 📅 Book your consultation online 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
What the Research Says
The research on dilatory ETD is clear on what it is and what drives it, and appropriately reserved on chiropractic-specific outcomes, which we present honestly.
On classification, dilatory ETD is one of three recognized types of Eustachian tube dysfunction from the 2015 expert consensus statement, and it is consistently described as the most common type, subdivided into functional, dynamic (muscular), and anatomical obstruction. The Cleveland Clinic frames the obstructive type as the tube failing to open properly with fluid building up and causing pressure, and notes ETD is most common in young children.
On the mechanism that matters most for our approach, the 2025 review is explicit that functional obstruction occurs when the tube is structurally open-able but fails to open effectively during swallowing or yawning, driven by neuromuscular dysfunction of the tensor veli palatini and levator veli palatini muscles or by inflammatory inhibition. The neuromuscular framing is what links this condition to the cranial nerves and, by extension, the upper cervical spine. Physiopedia documents the shared trigeminal innervation between the jaw muscles and the tensor veli palatini, providing the anatomical rationale.
On the inflammatory drivers, clinical references consistently identify mucosal inflammation from allergic rhinitis, chronic rhinosinusitis, reflux, upper respiratory infections, and smoke exposure as the most common causes of dilatory dysfunction, which is why medical management targets these.
Where the evidence is genuinely limited is in trials of upper cervical chiropractic for dilatory ETD specifically. We have not found large randomized trials establishing that upper cervical care resolves this condition, and we will not pretend otherwise. The honest summary: the condition, its subtypes, and its neuromuscular and inflammatory mechanisms are well understood, and addressing the neuromuscular coordination of the tube is a reasonable, rationale-based strategy, used alongside appropriate medical care and evaluated case by case.
Lifestyle Factors That Help
Whether or not upper cervical care is part of your plan, several daily factors influence dilatory ETD, largely because they affect the inflammation and congestion that drive the obstruction.
Manage allergies and congestion proactively. Because allergic rhinitis and sinus inflammation are leading drivers, staying ahead of allergies, especially in Florida’s long allergy seasons, directly supports tube function. Work with your provider on an allergy plan if this is your pattern.
Address reflux. Laryngopharyngeal reflux is a well-documented contributor, and its irritation reaches the tissues around the tube. If you have reflux symptoms, managing them, through diet, timing of meals, and medical care when needed, can help your ears.
Avoid tobacco smoke. Smoke exposure is repeatedly identified as a contributor to dilatory dysfunction. Avoiding it, including secondhand smoke, supports the health of the tube lining.
Stay hydrated. Well-hydrated mucosa functions and clears better, which matters especially in the Florida heat. Aim for at least half your body weight in ounces of water daily.
Practice gentle equalization, not forceful straining. Swallowing, yawning, and chewing gum encourage the tube to open. Aggressive, forceful attempts to “pop” the ears are not helpful and can irritate things further.
Manage jaw tension. Because the jaw and the tube share trigeminal wiring, clenching and nighttime grinding can worsen tube coordination. Addressing jaw tension supports better tube function.
Don’t ignore a persistent one-sided blockage. If only one ear stays blocked for weeks, get it evaluated. This is the pattern most worth ruling out an anatomical cause for, and it is a matter of safety, not just comfort.
If you found this guide useful, you may also want to read our main guide on Eustachian tube dysfunction, which covers all three types and the upper cervical approach, and our guide on TMJ and TMD, since jaw dysfunction and tube dysfunction share the same nerve supply and often travel together.
Serving Sarasota and the Surrounding Communities
Lavender Family Chiropractic is located in Sarasota, Florida, at 5899 Whitfield Avenue, Suite 107, at the corner of University and Whitfield. From this central location, we serve patients throughout the region, including Bradenton, Lakewood Ranch, Palmetto, Parrish, Venice, Osprey, Nokomis, Ellenton, and the surrounding Gulf Coast communities. Patients also travel from St. Pete, Riverview, and Manatee County to receive specialized upper cervical care here.
If your ears have been clogged, full, or muffled for weeks or months and partial fixes keep wearing off, we would be glad to take an honest look at whether the neuromuscular side of the problem, and the top of your neck, is part of the picture.
Top 15 FAQs About Dilatory (Obstructive) ETD and Upper Cervical Care
1. What is dilatory or obstructive ETD? It’s the most common type of Eustachian tube dysfunction, where the tube doesn’t open well enough or often enough to keep your middle ear ventilated. The result is persistent ear fullness, muffled hearing, and popping that won’t fully clear, present under everyday conditions rather than just during pressure changes.
2. How is it different from the flying/storm type? With baro-challenge ETD, the tube works fine at rest and only struggles during pressure changes like flights or weather. With dilatory ETD, the difficulty is constant or near-constant, because the tube’s basic opening function is impaired.
3. What are the three subtypes? Functional (the tube is structurally fine but the muscles don’t open it effectively), dynamic or muscular (the active opening underperforms), and anatomical (a physical blockage like enlarged adenoids or, rarely, a mass). The first two are neuromuscular; the third is structural.
4. What causes it? Most often, inflammation and congestion of the tube’s lining from allergies, sinus issues, colds, or reflux, and, in the functional subtype, ineffective opening by the tube’s muscles. Smoke exposure is also a contributor.
5. Why don’t decongestants fully fix it? They target the inflammation, which is part of the problem, so they often help partially. But if the neuromuscular coordination of tube opening is also involved, treating inflammation alone leaves that piece unaddressed, which is why relief can be incomplete.
6. How does my neck connect to this? The muscles that open the tube are controlled by cranial nerves that travel near the brainstem, beside the atlas and axis. Functional obstruction is largely a failure of those muscles to open the tube, so the nervous-system input from the upper neck is plausibly relevant.
7. Can upper cervical care cure this? We won’t claim a cure. The anatomy and the neuromuscular mechanism are well established, but trial evidence for chiropractic specifically resolving dilatory ETD is limited. The goal is to address the neuromuscular contributor alongside appropriate medical care, evaluated case by case.
8. Is the adjustment safe with irritated ears? Yes. The Knee Chest Upper Cervical technique is gentle and precise, with no twisting, cracking, or forceful manipulation, which is appropriate when tissues are already irritated. We examine thoroughly first.
9. When should I see an ENT instead? Any persistent one-sided blockage, especially in an adult, or signs pointing to an anatomical cause, should be evaluated by an ENT to rule out a structural problem. We’ll refer you when the picture calls for it. This is about safety.
10. Can this affect my hearing? Yes, temporarily. Poor ventilation and fluid behind the eardrum can muffle hearing. When chronic, dilatory ETD is associated with middle ear problems, which is another reason not to leave a persistent case unaddressed.
11. Does allergy season make it worse? Very often, yes. Because allergic inflammation is a leading driver, Florida’s long allergy seasons can aggravate dilatory ETD. Managing allergies proactively is one of the most useful things you can do.
12. Does reflux really affect my ears? It can. Laryngopharyngeal reflux irritates the tissues around the tube and is a recognized contributor. If you have reflux symptoms, managing them may help your ears.
13. Does jaw clenching matter? It can. The jaw muscles and the main tube-opening muscle share the same nerve supply, so clenching and grinding can worsen tube coordination. Addressing jaw tension may help.
14. How will I know if upper cervical care is right for me? Only a thorough evaluation can tell. Our exam, including 3D imaging and nervous-system scans, shows whether an upper cervical misalignment is contributing, and we’ll give you an honest assessment, including whether you also need medical management of inflammation.
15. How do I get started? Call our Sarasota office at (941) 243-3729 or book your consultation online. We’ll review your history, perform a thorough exam, screen for red flags, and give you a straight answer about how upper cervical care fits into your situation.
Take the Next Step
Chronic, obstructive ear fullness is wearing precisely because it does not let up, and because the usual fixes so often leave a piece of the problem behind. That remaining piece is frequently the neuromuscular coordination that opens your Eustachian tube, which the standard inflammation-focused approach does not address, and which is influenced by the top of your neck.
If you are in Sarasota, Bradenton, Lakewood Ranch, or anywhere along the Gulf Coast and you have been living with clogged, muffled ears, Dr. Rusty Lavender and Dr. Jacob Temple at Lavender Family Chiropractic are here to give you an honest evaluation of whether upper cervical care, alongside appropriate medical management, fits into your situation.
📞 Call (941) 243-3729 today to schedule your consultation 📅 Book online here 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield