By Dr. Rusty Lavender D.C.
Patulous Eustachian Tube Dysfunction Relief and Treatment in Sarasota: Most ear-pressure problems involve a tube that won’t open. This one is the opposite, and it can be just as distressing. You hear your own voice booming inside your head, as though you’re talking into a barrel. You hear yourself breathe, in and out, sometimes even your own heartbeat. Your ear feels full, but unlike a typical clogged ear, the fullness eases when you lie down and worsens when you stand, exercise, or talk for a long time. If that’s your experience, you may be dealing with patulous Eustachian tube dysfunction.
Patulous ETD is the third recognized type of Eustachian tube dysfunction, and it is fundamentally different from the other two. In the common obstructive type and in the baro-challenge type, the tube fails to open well enough. In patulous ETD, the tube stays open too much when it should be closed. That single difference changes everything: the symptoms, the causes, and importantly, the treatment. It also means we need to be especially careful and honest about where upper cervical care does and does not fit, and we will be.
At Lavender Family Chiropractic in Sarasota, Florida, our entire focus is the upper cervical spine, the atlas (C1) and axis (C2) at the very top of the neck, using 3D CBCT imaging and paraspinal infrared thermography and the gentle Knee Chest Upper Cervical technique. We want to be straight with you from the first paragraph: patulous ETD is a condition where many of the recognized causes lie outside what chiropractic addresses, and where medical evaluation is often essential. We’ll explain the condition thoroughly, tell you honestly where the upper neck may play a modest role, and tell you just as honestly when you need an ENT.
What Is Patulous Eustachian Tube Dysfunction?
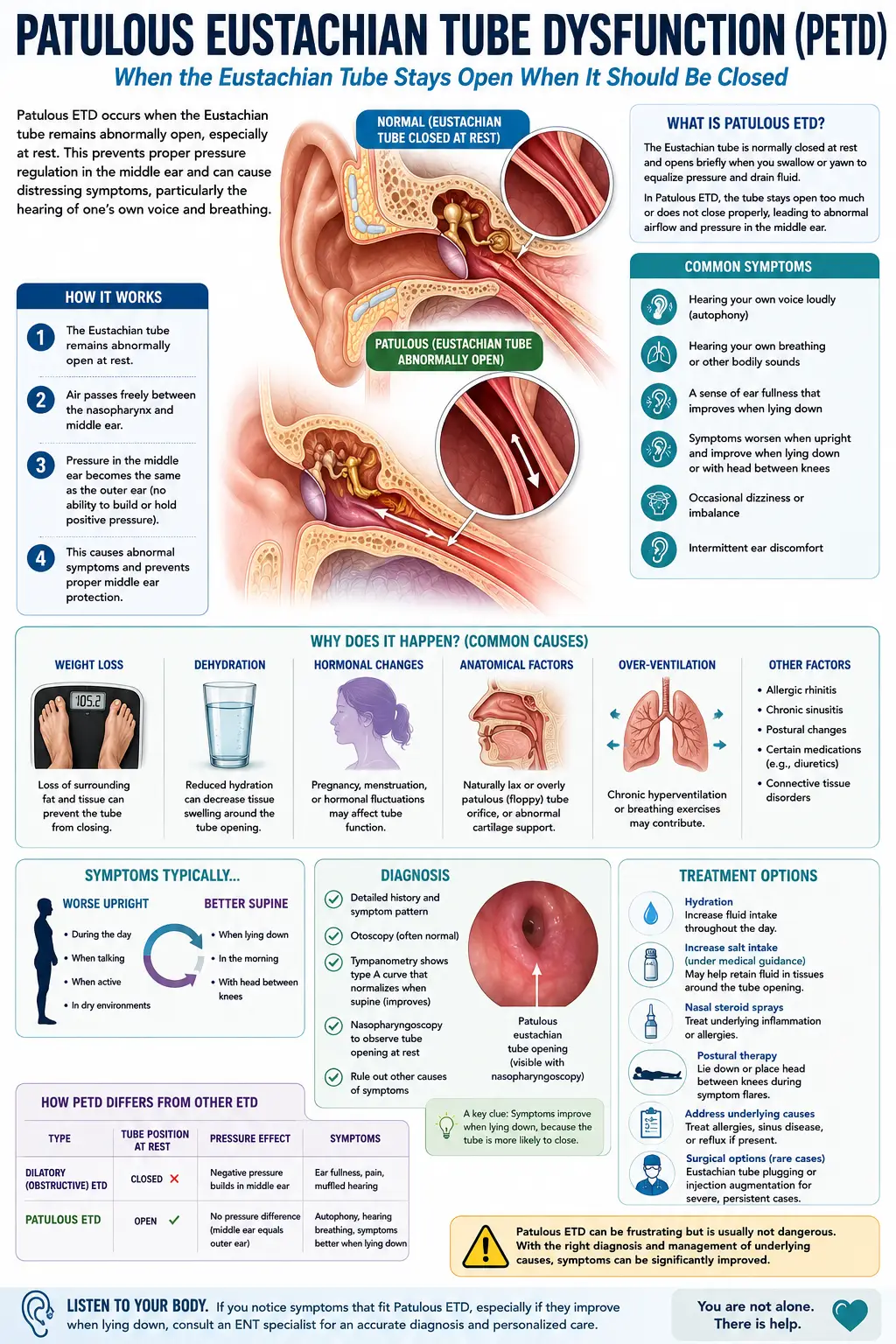
The Eustachian tube connects your middle ear to the back of your nose and throat. Normally it stays closed at rest and opens only briefly when you swallow, yawn, or chew, just long enough to equalize pressure and drain fluid, then closes again. That resting closure is important: it keeps the middle ear sealed off from the constant air movement and sound of your own breathing and voice traveling up from your throat.
In patulous ETD, the tube fails to stay closed. It remains abnormally open, or patent (the medical term “patulous” means open). With the tube held open, there is a continuous, open channel between your throat and your middle ear. As Brigham and Women’s Hospital describes it, the open Eustachian tube allows sounds to be transmitted directly to the middle ear, so patients experience autophony, the hearing of self-generated sounds including one’s own breathing, voice, or heartbeat.
Autophony is the hallmark. If your defining symptom is hearing yourself, your breath, your voice, sometimes your pulse, unusually and uncomfortably loudly, that points toward patulous ETD rather than the obstructive kind. Many people with patulous ETD also describe a sense of ear fullness or blockage, which is confusing because it can feel similar to a clogged, obstructed ear even though the underlying problem is the exact opposite. This is one reason the condition is frequently misdiagnosed.
The Telltale Pattern: Better Lying Down, Worse Standing
One of the most useful distinguishing features of patulous ETD is positional: symptoms typically improve when you lie down and worsen when you are upright, active, or talking a lot.
There is a clear mechanical reason for this. When you lie down, fluid (dependent edema) shifts into the tissues around the tube, and that mild swelling closes the abnormally open tube, relieving the autophony, at least temporarily. When you stand back up, the tissues drain, the tube falls back open, and the symptoms return. A 2025 case report on patulous ETD notes that patients typically report symptoms that worsen in upright positions but improve when lying down. Some people instinctively discover that lowering the head, or even putting the head between the knees, brings brief relief, the same mechanism at work.
This positional pattern is almost the reverse of what people expect from an “ear problem,” and recognizing it is often the key to getting the right diagnosis after months of being treated for the wrong thing.
What Causes the Tube to Stay Open
Here is where honesty about scope becomes essential, because the recognized causes of patulous ETD point largely toward factors that chiropractic care does not address. We think you deserve to understand the real drivers.
The most common and well-documented cause is significant weight loss. Surrounding the Eustachian tube is a small cushion of fatty tissue called Ostmann’s fat pad, which helps hold the tube closed at rest. When someone loses a substantial amount of weight, this fat pad shrinks, and the tube loses the tissue bulk that kept it closed. Brigham and Women’s notes plainly that when dramatic weight loss occurs, the fatty tissues surrounding the tube shrink, disrupting tube function. This is why patulous ETD sometimes appears after major weight loss, including after bariatric surgery.
Other recognized causes include dehydration, particularly from vigorous exercise, which reduces the water content of the tissues around the tube; pregnancy and hormonal changes, which can alter the tube’s opening pressures; scarring or traction in the nasopharynx, sometimes following procedures like adenoidectomy; and damage to or altered tone of the tensor veli palatini, the muscle that influences the tube. Caffeine and dehydration are also commonly cited as contributors that can be modified.
We highlight all of this for a reason. If your patulous ETD stems primarily from significant weight loss, scarring, or a hormonal change, those are not things an upper cervical adjustment fixes, and any provider implying otherwise would be misleading you. The honest, useful framing is narrower, and we’ll get to it.
Where Upper Cervical Care May, and May Not, Fit
We want to be more restrained here than we are with the other types of ETD, because the evidence and the mechanisms warrant restraint.
The one genuine connection point is muscle tone. The tensor veli palatini, the muscle whose tone helps regulate the tube, is innervated by the mandibular branch of the trigeminal nerve, the same nerve that serves the muscles of the jaw. Physiopedia’s review notes that because the trigeminal nerve supplies both the muscles of mastication and the tensor veli palatini, addressing the TMJ and associated structures can influence signaling to the muscles that control the Eustachian tube. Notably, clinical discussions of patulous ETD list temporomandibular disorders among the underlying factors worth addressing. Because the upper cervical spine influences the cranial-nerve pathways and muscle tone in this region, and because the jaw and the tube share trigeminal wiring, it is reasonable to consider whether upper neck and jaw mechanics are contributing in a given person.
But here is the honest boundary. For patulous ETD driven primarily by Ostmann’s fat pad loss from weight change, by hormonal shifts, or by scarring, upper cervical care is not a fix, and we will not present it as one. The most we would claim is that, in some patients, addressing upper cervical and jaw-related muscle tone may be one supportive piece, and that a careful evaluation can determine whether it is relevant to you at all. The trial evidence for chiropractic care in patulous ETD specifically is essentially absent, and we say that plainly. This is a condition where our most valuable role is often a thorough evaluation, honest counsel, and helping you get to the right provider.
A Critical Caution: Decongestants Can Make It Worse
This point is important enough to stand alone, because it is where patulous ETD trips up both patients and providers. With the common obstructive type of ETD, decongestants and drying agents are a standard first move, because the goal is to reduce swelling and open a congested tube. With patulous ETD, that same approach can backfire.
Because the problem is a tube that is already too open, drying it out further can worsen the symptoms. The 2025 case report lists the use of nasal or oral decongestants among the factors that can exacerbate patulous ETD. This is precisely why getting the right diagnosis matters so much: a treatment that helps one type of ETD can aggravate the other. If you have autophony that gets worse when you take decongestants, that is itself a meaningful clue pointing toward the patulous type, and a reason to seek proper evaluation rather than continuing to self-treat.
What Care Looks Like at Lavender Family Chiropractic
If you come into our Sarasota office with symptoms suggesting patulous ETD, here is what to expect, and where we’ll likely direct you.
Your first visit begins with a thorough consultation. Dr. Lavender or Dr. Temple will listen carefully to your history: whether your main symptom is autophony, whether it improves lying down and worsens upright, any recent significant weight loss, vigorous exercise and dehydration, pregnancy, prior ear or nasopharyngeal surgery, caffeine intake, and any jaw clenching or TMJ symptoms. This history usually makes the patulous pattern recognizable.
Because patulous ETD is frequently best managed medically, a large part of our value here is accurate recognition and appropriate referral. If your picture points clearly to weight-loss-related or structural patulous ETD, we will tell you directly and help you connect with an ENT, who can confirm the diagnosis with specialized testing (such as observing the eardrum move in time with your breathing) and discuss medical and, in some cases, procedural options. We are not here to keep you in our office for a condition we are not the right fit for. Patient honesty comes before everything.
Where upper cervical care may be considered is the subset of patients in whom jaw and upper-neck muscle tone appears to be a contributing factor, evaluated alongside the other causes, not instead of addressing them. For appropriate candidates, we use advanced 3D CBCT imaging and functional nervous system scans, and care is delivered through the gentle Knee Chest Upper Cervical technique, with no popping or twisting. We would frame any such care modestly and track whether it actually helps, rather than promising it will.
We will also reinforce the modifiable basics that genuinely help many people with patulous ETD: rehydration, moderating caffeine, and, where relevant, addressing jaw tension and TMJ dysfunction.
📞 Call (941) 243-3729 to schedule your consultation 📅 Book your consultation online 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
What the Research Says
The research on patulous ETD is well-developed on mechanism and diagnosis, and clear that treatment differs sharply from obstructive ETD, points we present honestly, including the limits of what we offer.
On the mechanism, the loss of tissue support around the tube is central. Brigham and Women’s describes how dramatic weight loss shrinks the fatty tissues that keep the tube closed, and dehydration from vigorous exercise reduces their water content, while hormonal changes in pregnancy can also contribute. The hallmark symptom of autophony arises directly from the open tube transmitting self-generated sound to the middle ear.
On the distinguishing features, the literature is consistent that symptoms worsen upright and improve lying down, and that decongestants are among the factors that can exacerbate the condition, the opposite of how obstructive ETD behaves. This is why the two types must be carefully distinguished, since treatment strategies diverge significantly: obstructive cases benefit from pressure-equalization and allergy control, whereas patulous cases sometimes require quite different, including procedural, management.
On the neuromuscular angle relevant to our scope, the tensor veli palatini’s tone influences the tube, and that muscle shares trigeminal innervation with the jaw, as Physiopedia documents. This provides a narrow, plausible rationale for considering jaw and upper-neck factors in selected patients, but it is not evidence that upper cervical care resolves patulous ETD. We have found no trial evidence to support such a claim, and we will not imply one. Our honest position: patulous ETD is well understood mechanically, its management is often medical, and upper cervical care has at most a modest, case-by-case supporting role tied to muscle tone, used alongside, and never as a replacement for, proper evaluation.
Lifestyle and Self-Care Factors
For patulous ETD specifically, several modifiable factors genuinely help, and they are worth knowing because some are simple.
Hydration is paramount. Because dehydration reduces the tissue volume that helps keep the tube closed, staying well hydrated is one of the most useful self-care steps, especially in the Florida heat and especially around vigorous exercise. Rehydrating sometimes relieves symptoms noticeably.
Be cautious with weight loss. If patulous symptoms began during or after significant weight loss, that connection is real. This is not a reason to avoid healthy weight management, but it is worth discussing with your provider, and worth knowing that the symptom often has this explanation.
Moderate caffeine. Caffeine is a recognized contributor for some people, partly through its drying, diuretic effect. Cutting back is a low-risk experiment.
Use position for relief. Lying down, or briefly lowering the head, can ease autophony in the moment by shifting fluid to close the tube. It’s a temporary measure, but a useful one to understand.
Be careful with decongestants. As above, drying agents can worsen patulous ETD. If decongestants make your autophony worse, take that as a diagnostic clue and raise it with a provider rather than continuing them.
Address jaw tension. Where TMJ dysfunction or clenching is part of your picture, addressing it may help, given the shared nerve supply between the jaw and the tube.
If you found this guide useful, you may also want to read our main guide on Eustachian tube dysfunction, which covers all three types and how they differ, and our guide on TMJ and TMD, since jaw factors are among the modifiable contributors to patulous ETD.
Serving Sarasota and the Surrounding Communities
Lavender Family Chiropractic is located in Sarasota, Florida, at 5899 Whitfield Avenue, Suite 107, at the corner of University and Whitfield. From this central location, we serve patients throughout the region, including Bradenton, Lakewood Ranch, Palmetto, Parrish, Venice, Osprey, Nokomis, Ellenton, and the surrounding Gulf Coast communities.
If you have been hearing your own voice and breathing too loudly and no one has been able to explain why, we would be glad to listen, help you understand whether this is patulous ETD, and point you toward the right care, including being honest about when that care is medical rather than chiropractic.
Top 15 FAQs About Patulous ETD and Upper Cervical Care
1. What is patulous ETD? It’s the type of Eustachian tube dysfunction where the tube stays open when it should be closed, the opposite of the common obstructive type. The hallmark symptom is autophony, hearing your own voice, breathing, or heartbeat unusually loudly.
2. What is autophony? It’s the experience of hearing self-generated sounds, your breathing, voice, or pulse, loudly inside your own head, because the open tube transmits those sounds directly to your middle ear. It’s the defining feature of patulous ETD.
3. Why does it feel better when I lie down? Lying down shifts fluid into the tissues around the tube, which closes the abnormally open tube and relieves symptoms temporarily. Symptoms typically return when you stand back up. This positional pattern is a key clue.
4. Why do I feel fullness if the tube is open? Confusingly, patulous ETD can feel like a blocked ear even though the tube is too open. This overlap with obstructive symptoms is exactly why the condition is so often misdiagnosed.
5. What causes patulous ETD? The most common cause is significant weight loss, which shrinks the fat pad that helps keep the tube closed. Other causes include dehydration, pregnancy and hormonal changes, scarring from prior surgery, and altered muscle tone around the tube.
6. Can chiropractic fix patulous ETD? We’re honest here: for cases driven by weight loss, hormonal change, or scarring, no, and we won’t claim otherwise. Upper cervical care may have a modest, case-by-case role only where jaw and neck muscle tone is a contributing factor, alongside proper evaluation.
7. So why see an upper cervical chiropractor at all? Mainly for accurate recognition and honest guidance, and, in selected patients, to address jaw and upper-neck muscle-tone factors. A big part of our value with this condition is identifying it correctly and directing you to the right care.
8. Should I see an ENT? Often, yes. Patulous ETD is frequently best managed medically, and an ENT can confirm it with specialized testing and discuss medical or procedural options. We’ll refer you when your picture calls for it.
9. Will decongestants help? Usually not, and they can make patulous ETD worse by drying out an already too-open tube. If decongestants worsen your autophony, that’s a clue you may have the patulous type. Raise it with a provider.
10. Does hydration really matter? Yes, more than for most ear conditions. Dehydration reduces the tissue volume that helps keep the tube closed, so staying well hydrated is one of the most useful self-care steps, especially around exercise and in the Florida heat.
11. Did my weight loss cause this? Quite possibly. Significant weight loss is the most common cause, through shrinkage of the fat pad around the tube. This isn’t a reason to avoid healthy weight management, but it explains the timing for many people.
12. Can pregnancy cause it? Yes. Hormonal changes in pregnancy can alter the tube’s opening pressures and produce patulous symptoms, which often improve after pregnancy. It’s worth knowing so you’re not alarmed.
13. Does jaw clenching play a role? It can. The muscle that influences the tube shares its nerve supply with the jaw, and TMJ disorders are listed among the modifiable contributors. Addressing jaw tension may help in some cases.
14. Is the adjustment safe? Yes, when appropriate. The Knee Chest Upper Cervical technique is gentle and precise, with no twisting or cracking. But for this condition specifically, we’re careful to use it only where it’s genuinely indicated, not as a blanket answer.
15. How do I get started? Call our Sarasota office at (941) 243-3729 or book online. We’ll listen to your history, help determine whether this is patulous ETD, and give you a straight answer, including pointing you to an ENT when that’s the right move.
Take the Next Step
Patulous Eustachian tube dysfunction is one of the most misunderstood ear conditions, partly because it can masquerade as a blocked ear while being the opposite, and partly because the usual ear treatments can make it worse. Getting it recognized correctly is often the hardest and most important step.
If you are in Sarasota, Bradenton, Lakewood Ranch, or anywhere along the Gulf Coast and you’ve been hearing yourself too loudly with no clear answers, Dr. Rusty Lavender and Dr. Jacob Temple at Lavender Family Chiropractic are here to listen, help you understand what’s happening, and guide you toward the right care, with honest counsel about when that care is medical and where, if anywhere, upper cervical care fits.
📞 Call (941) 243-3729 today to schedule your consultation 📅 Book online here 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield