Mal De Débarquement Syndrome: You went on a cruise out of Port Tampa Bay. You took a long flight to see family. You drove down I-75 from Atlanta in one stretch. You spent a weekend on a friend’s boat off Anna Maria Island. The trip ended days, weeks, even months ago — but your body never got the memo. The floor still tilts. The kitchen counter feels like a deck beneath your feet.
You sway in line at Publix, rock subtly while standing in your own shower, and feel a strange pulling sensation when you try to walk in a straight line down the hallway. The only time it stops is when you get back in a car or on a boat — which feels like a cruel joke, because the very motion that started this is the only thing that quiets it.
If that description made the back of your neck tighten with recognition, you may be living with Mal de Débarquement Syndrome — MdDS for short. And if you have been told it is rare, untreatable, “all in your head,” or that you simply have to wait it out for a year and hope it goes away, please keep reading. There is a piece of this puzzle that almost no one in conventional medicine examines, and it sits at the very top of your spine.
We see patients with MdDS at our office every month. They come from Sarasota, Bradenton, Lakewood Ranch, Venice, and well beyond — often after years of cycling through ENTs, neurologists, vestibular therapists, and primary care doctors who all return the same verdict: every test looks normal, so there is nothing more to do. They arrive exhausted, frightened, and quietly convinced that their body is broken in some unfixable way.
Almost always, there is a pattern hiding in plain sight. And the pattern is not in the inner ear, not in the brain on MRI, and not in any blood panel. It is in the relationship between the top two bones of your neck, the brainstem they protect, and the balance system that depends on both for accurate information.
This is the article we wish every MdDS patient on the Suncoast could read.
What Is Mal de Débarquement Syndrome?
Mal de Débarquement is French for “sickness of disembarkment.” The original meaning is exactly what it sounds like — that lingering feeling many travelers get for an hour or two after stepping off a long boat ride or flight, where the ground seems to keep gently rocking. For most people, that sensation fades within a day. The brain quickly recalibrates, recognizes that the body is now on stable ground, and the perception of motion stops.
But for a smaller group of people, it does not stop. The rocking, swaying, or bobbing sensation persists for more than a month. It can stretch into years. This is the clinical condition known as Mal de Débarquement Syndrome, or MdDS, and it is recognized as a central vestibular disorder by the Bárány Society’s International Classification of Vestibular Disorders.
The hallmark symptoms include:
- A constant or near-constant sense of rocking, swaying, or bobbing — as if you are still on a boat, train, or plane
- A feeling of being pulled to one side, or of the floor tilting underneath you
- Symptoms that paradoxically improve when you re-expose yourself to passive motion (driving, riding in a car, getting back on a boat)
- Symptoms that worsen with stillness, when standing on stable ground, or in visually busy environments like grocery stores
- Heightened sensitivity to visual motion — scrolling phones, ceiling fans, busy patterns, traffic
- Cognitive fog, fatigue, anxiety, and difficulty concentrating
- A sense that something is fundamentally “off” with how your body relates to space
There are two recognized forms. Motion-triggered MdDS (MT-MdDS) develops within 48 hours of disembarking from extended passive motion — typically a cruise, a long flight, or a multi-hour drive. Non-motion-triggered MdDS (non-MT-MdDS) develops without any clear travel trigger and may follow stress, illness, hormonal shifts, or a minor head or neck injury.
MdDS is not lightheadedness. It is not panic. It is not BPPV, where crystals dislodge in the inner ear and cause sharp positional spinning. MdDS is a persistent oscillatory perception of self-motion that the conventional inner-ear tests — VNG, ENG, VEMP, audiograms, MRI — almost universally read as completely normal. That is why so many patients are dismissed. The standard tools cannot see the problem because the problem is not where the standard tools are looking.
MdDS Is a Brain, Nervous System, and Sensory Integration Condition
To understand why upper cervical chiropractic care can help with a condition that lives, by definition, in the central nervous system, you need a brief look at how your balance system actually works.
Your brain decides where your body is in space by combining three streams of sensory input in real time:
The Vestibular System
Your inner ears contain tiny fluid-filled canals and crystals that detect motion, acceleration, and head position. They send constant signals to the brainstem about whether you are moving, in what direction, and how fast.
The Visual System
Your eyes confirm or contradict what the inner ear is reporting. When you look at the horizon and it stays still, your brain confirms you are not moving. When the visual field shifts, your brain processes that as motion.
The Proprioceptive System
This is the one almost no one talks about, and it is the most important part of the MdDS conversation. Your muscles, joints, tendons, and especially the deep stabilizing muscles of your upper neck contain enormous numbers of mechanoreceptors and proprioceptors — sensors that tell the brain where your head is positioned relative to your body and the ground.
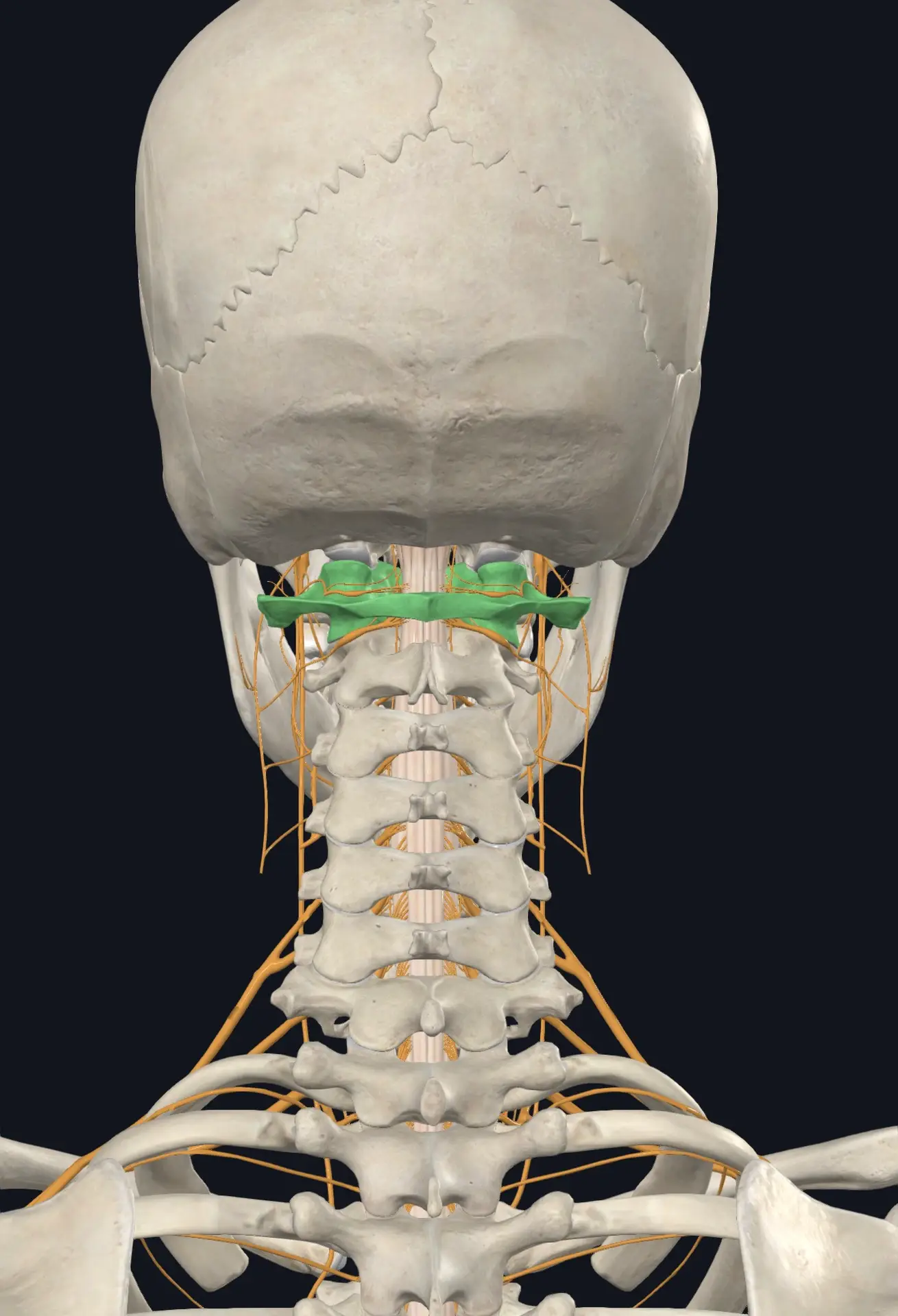
The upper cervical spine — specifically the joints between your skull, atlas (C1), and axis (C2) — has the highest density of these proprioceptive receptors anywhere in the body. By some estimates, the suboccipital region contains more proprioceptive nerve endings per square inch than any other part of the human spine.
Your brain integrates all three streams in the brainstem and cerebellum. When all three agree, you feel grounded and steady. When even one stream sends distorted, delayed, or contradictory information, your brain enters what researchers call “sensory mismatch.” It tries to compensate. It increases the gain on certain pathways. It builds a new internal model of what “normal” feels like.
In MdDS, the leading scientific theory is that the brain has maladapted — that it built an internal model of motion during your trip and got “stuck” in that model after the motion stopped. Recent research from neurotology labs has pointed specifically to the velocity storage mechanism and the vestibulo-ocular reflex as the central neurological systems that fail to recalibrate.
Here is the part that is almost never discussed in conventional MdDS care: if the proprioceptive input from your upper neck is distorted — if your atlas is even slightly misaligned, if the deep cervical muscles are sending faulty information about where your head is in space — your brain has a much harder time recalibrating. It cannot reset to “stable ground” if the messages it is receiving from your neck are still telling it the head is unstable, tilted, or moving.
This is why a growing body of clinical evidence suggests that addressing upper cervical dysfunction may be one of the missing pieces in non-resolving MdDS.
The Upper Neck: Your Body’s Most Critical Junction
The atlas (C1) and axis (C2) are unlike any other vertebrae in the spine. They are the only vertebrae that directly cradle the brainstem. They allow more than half of all head rotation to occur. They surround the vertebral arteries that carry blood to the back half of your brain — including the very brainstem regions responsible for vestibular processing. And they sit at the convergence point of the vagus nerve, the upper cervical nerve roots, and the spinal accessory nerve, all of which feed into central balance, autonomic, and postural control systems.
When the atlas or axis is misaligned — whether from a fall years ago, a whiplash injury, a sports concussion, a difficult birth, repetitive postural strain, or simply sleeping wrong on a long flight — the consequences can ripple through the entire nervous system:
- Distorted proprioceptive signaling. The brain receives faulty information about head and neck position, contributing directly to sensory mismatch.
- Mechanical brainstem irritation. The brainstem tracts that process vestibular and balance information run directly through this region. Any chronic mechanical stress here can alter how those signals are processed.
- Compromised vertebral artery flow. The vertebral arteries thread through the transverse foramina of C1 and C2. Misalignment can subtly alter blood flow to the very brainstem regions involved in MdDS.
- Cerebrospinal fluid flow disruption. The atlanto-occipital junction is one of the most important sites for CSF drainage from the cranium. Restriction here has been linked to a wide range of neurological and vestibular symptoms.
- Vagal nerve interference. The vagus nerve passes directly through this region and influences autonomic balance, which is frequently disrupted in MdDS patients.
You can learn more about how this region affects nervous system function on our page about upper cervical chiropractic care.
Why Traditional Care Often Misses This
Most MdDS patients describe the same frustrating journey. They see their primary care doctor, who refers them to ENT. ENT does a hearing test, a VNG, sometimes an MRI of the brain. Everything reads normal. They are referred to neurology. Neurology rules out stroke, multiple sclerosis, and tumors. Everything reads normal. They are sent to vestibular rehabilitation, which can help some patients but often makes MdDS worse because traditional VRT is designed for inner-ear-based vestibular disorders, not central recalibration disorders. They may be prescribed clonazepam, an SSRI, or sent home with a diagnosis of “anxiety.”
What is rarely — almost never — examined is the structural and functional state of the upper cervical spine and the proprioceptive feedback it generates. Standard X-rays do not assess it functionally. Standard MRI does not capture the dynamic, postural relationship between the skull and atlas. Most physical exams do not test the deep cervical proprioceptors at all. So the patient is told everything is normal, when in reality, the one system that has not been properly evaluated is the one most likely contributing to the persistence of their symptoms.
This is the gap our office was built to address.
Upper Cervical Chiropractic Care: What Makes It Different
Upper cervical chiropractic is not the popping, twisting, or general neck cracking many people picture when they think of a chiropractor. It is a precise, gentle, imaging-driven approach focused exclusively on the relationship between the skull, atlas, and axis. There is no twisting of the head, no forceful manipulation, no audible “crack.” For patients with MdDS — many of whom are already overwhelmed by motion sensitivity — this gentleness is not just a preference, it is a clinical necessity.
The work is built on three principles:
- Precision. No two upper necks are misaligned in exactly the same way. Every correction is calculated for that specific person, that specific spine, that specific day.
- Specificity. Adjustments target only the segments that need correction. Healthy joints are left alone.
- Sustainability. The goal is to hold the correction over time so the nervous system can fully recalibrate, not to deliver repeated forceful adjustments that destabilize the area.
When the atlas and axis are restored to a more neutral, balanced position, several things begin to happen — often gradually, sometimes in waves. Proprioceptive input from the upper neck begins to normalize. The brainstem receives cleaner signals. Vertebral artery and CSF flow improve. Vagal tone shifts toward parasympathetic dominance. And the brain, finally given accurate information from the very joints that tell it where the head is in space, begins to do what it has been trying to do all along — recalibrate, and let go of the maladaptive motion model that has been running on a loop.
This is not a cure-all. It is not magic. It is not appropriate for every patient. But for the right patient, it can be the missing piece that the previous five providers never examined.
What to Expect at Lavender Family Chiropractic
Our team — Dr. Rusty Lavender and Dr. Jacob Temple — has built our practice around this work. Every new patient at our Sarasota office goes through the same thorough, unhurried evaluation process:
- A detailed history that walks through your trip, your symptom timeline, prior trauma, surgeries, and every provider you have already seen
- A neurological and postural exam designed to identify where your nervous system is currently struggling
- 3D CBCT (cone beam computed tomography) imaging that shows the exact three-dimensional relationship between your skull, atlas, and axis — something traditional X-rays cannot do
- Tytron paraspinal thermography scans that measure autonomic nervous system function along your spine, giving us an objective view of where your nervous system is under stress
- A clear, honest report of findings — including whether we believe we can help, and just as importantly, whether we believe you would be better served somewhere else
You can read more about how the first visit works on our What to Expect page.
We never rush a patient into care, and we never accept a patient we do not believe we can help.
If you have been searching for answers to your MdDS for months or years and you live anywhere on the Suncoast — from downtown Sarasota to Lakewood Ranch, Bradenton, Venice, Osprey, Parrish, or Palmetto — we would like to evaluate your case. You can schedule your new patient visit here or call us directly at (941) 243-3729.
Evidence and Emerging Research
We are careful with claims at our office. MdDS is a relatively under-researched condition compared to migraine or Parkinson’s, and the body of literature specific to chiropractic and MdDS is still small. That said, the clinical and scientific signal is meaningful and worth understanding.
A widely cited 2012 case report published in the Journal of Chiropractic Medicine by Gleberzon and Arts documented a patient with recurrent episodes of Mal de Débarquement Syndrome who experienced clinical improvement under upper cervical chiropractic management. While a single case report is not high-level evidence, it does establish biological plausibility and provides a documented framework for further inquiry.
The broader scientific literature on cervical proprioception and central vestibular processing is far more developed and consistently supports the underlying mechanism:
- Decades of research from the cervicogenic dizziness literature have established that distorted proprioceptive input from the upper cervical spine can produce balance disturbances, motion sensitivity, and disequilibrium even when the inner ear tests normal.
- Imaging and physiological studies have documented changes in cerebrospinal fluid dynamics, vertebral artery flow, and brainstem function in association with upper cervical dysfunction.
- Recent neurotology research has pointed clearly to maladaptation of the vestibulo-ocular reflex and velocity storage mechanism as central drivers of MdDS — both of which depend heavily on accurate proprioceptive input from the upper neck for proper recalibration.
- A growing body of work on craniocervical instability has shown overlap between cervical ligament laxity, distorted proprioception, and persistent vestibular symptoms in patients who do not respond to conventional vestibular care.
We do not promise a specific outcome for any individual patient. What we can say honestly is that for the right candidate, the mechanism is plausible, the clinical pattern is consistent, and the option is non-invasive, drug-free, and worth careful evaluation before more invasive interventions are considered.
You can learn more about how this work fits into the broader picture of nervous system health on our Why Upper Cervicalpage.
Lifestyle Factors That Complement Upper Cervical Care
Recovery from MdDS is rarely about a single intervention. The patients who do best almost always combine precise upper cervical care with consistent daily habits that support nervous system regulation. The following are the strategies we most commonly recommend:
Prioritize parasympathetic rest. MdDS patients are almost always running in a sympathetic-dominant state — wired, tired, and over-activated. Slow nasal breathing, vagal tone exercises, gentle walks, and sufficient sleep are not optional. They are part of the treatment.
Limit visual triggers strategically. Endless phone scrolling, fast-paced video, busy fluorescent environments, and visually complex screens can keep the brain stuck in over-processing mode. Short, intentional breaks — looking at the horizon, walking outside, blinking softly while focusing on a fixed point — give the visual-vestibular system room to settle.
Hydrate and stabilize blood sugar. The vestibular system is metabolically expensive. Dehydration, skipped meals, and blood sugar swings reliably worsen MdDS symptoms.
Move gently and consistently. Gentle, predictable movement — walking, easy yoga, low-impact strength work — helps the brain receive consistent, accurate proprioceptive input. Aggressive, high-intensity workouts can sometimes flare symptoms in the early stages of recovery.
Address underlying migraine physiology. MdDS overlaps significantly with migraine biology. Many of the dietary, sleep, and trigger-management strategies that help migraine sufferers also help MdDS patients. We discuss this in detail in our guide to natural migraine relief in Sarasota, which is worth reading if you have any history of migraines, vestibular migraines, or motion-triggered headaches.
Be patient with the timeline. Nervous system recalibration is not a one-week process. Most patients begin to notice meaningful shifts within the first month of upper cervical care, but true stabilization often takes three to six months of consistent care, consistent lifestyle support, and consistent rest.
Serving Sarasota and the Surrounding Gulf Coast
Our office is located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield, easy to reach from anywhere in Sarasota or Manatee County. Patients travel to us from across the Suncoast and beyond, including:
- Sarasota — downtown, Southside Village, Arlington Park, Gulf Gate, Palmer Ranch, University Park, Lakewood Ranch, Bee Ridge, Fruitville, Desoto Lakes, and the surrounding neighborhoods
- Bradenton — West Bradenton, East Bradenton, Cortez, Palma Sola, and surrounding areas
- Lakewood Ranch — Country Club East, Greenbrook, Heritage Harbour, Lakewood National
- Venice — Venice Island, South Venice, Nokomis, Laurel
- Osprey, Siesta Key, Longboat Key, and Lido Key
- Parrish, Palmetto, Ellenton, and Myakka City
- Port Charlotte, Punta Gorda, and North Port
- St. Petersburg and the broader Tampa Bay region
You can see the full list on our Areas We Service page. We routinely care for cruise passengers who developed MdDS after departing from Port Tampa Bay or Port Canaveral, snowbirds who developed it after long flights from the Northeast and Midwest, and lifelong Floridians who developed it after extended boating, fishing trips, or long road trips.
If you are willing to make the drive, we are willing to do the work.
Is Upper Cervical Care Right for You?
The honest answer is — sometimes yes, sometimes no, and that is exactly why the new patient evaluation matters. Upper cervical chiropractic is most likely to help an MdDS patient when:
- Symptoms began after a clear motion trigger or after a head, neck, or whiplash event
- Inner ear and brain imaging have ruled out other vestibular and neurological causes
- There is a history of trauma, falls, sports injuries, or whiplash earlier in life
- Conventional treatments — VRT, medications, dietary changes — have brought partial or no relief
- There are coexisting symptoms suggestive of upper cervical dysfunction: chronic neck tension, migraines, brain fog, autonomic dysregulation, jaw tension, ear fullness, or visual disturbances
Upper cervical care is less likely to be the right fit when MdDS is part of a broader, actively managed condition that requires a different first-line approach — which is exactly the kind of clarity our evaluation is designed to deliver. If we do not believe we can help, we will tell you, and we will help you find someone who can.
You Are Not Imagining This
If there is one message we want every MdDS patient on the Suncoast to hear, it is this: the rocking is real. The swaying is real. The exhaustion of fighting your own balance system every minute of every day is real. You are not anxious, you are not weak, and you are not making it up.
You are dealing with a genuine neurological condition that conventional care has not fully figured out yet — and the part of your body most likely to be contributing has almost certainly never been properly evaluated. That is the gap we exist to close.
We would be honored to meet you, hear your story, and tell you honestly whether we believe we can help. Whether you are five weeks into this or five years into it, the door is open.
Lavender Family Chiropractic 5899 Whitfield Avenue, Suite 107 Sarasota, FL 34243 (941) 243-3729 Schedule your new patient visit
Related Articles
- Vertigo Treatment Sarasota & Lakewood Ranch: How the Upper Cervical Spine Holds the Key to Lasting Relief
- Vestibular Migraines and Upper Cervical Care: A Comprehensive Guide to Relief
- When Your Head Feels Too Heavy: Craniocervical Instability, Vertigo, and Migraines
This blog is for informational purposes only and does not constitute medical advice. Please consult a qualified healthcare provider for diagnosis and treatment of any health condition. Lavender Family Chiropractic | 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 | (941) 243-3729
Related Posts
Popular Posts