Meniere’s Disease: If you’ve been diagnosed with Meniere’s disease, you already know how disabling it can be. The vertigo attacks that come without warning. The roaring tinnitus. The slow, fluctuating hearing loss in one ear. The crushing, deep pressure of aural fullness that feels like an invisible hand pushing against the inside of your skull. You’ve probably been told it’s a chronic condition with no cure, managed with low-sodium diets, diuretics, betahistine, intratympanic injections, and — if things get bad enough — surgical procedures.
What most Meniere’s patients are never told: a chiropractic researcher named Dr. Michael Burcon followed 300 Meniere’s patients for six years, found that every single one of them had a history of whiplash trauma — with an average 15-year delay between the injury and symptom onset — and documented a 97% improvement in vertigo intensity after upper cervical specific chiropractic care. His paper was published in the Journal of Upper Cervical Chiropractic Research in 2016 and presented at the Seventh International Symposium on Meniere’s Disease in Rome. He has presented his findings to more than 2,000 ENT surgeons across four continents, including Cleveland Clinic and the House Ear Institute.
That doesn’t mean upper cervical care is a guaranteed cure. It means there is a serious, peer-reviewed body of evidence connecting Meniere’s disease to upper cervical spine injury — and most patients have never been told that this connection even exists.
At Lavender Family Chiropractic in Sarasota, Florida, we routinely see Meniere’s patients who’ve been managing this condition for years without anyone ever evaluating the upper cervical spine. In this guide, we’ll walk through what Meniere’s actually is, the research connecting it to the upper neck, who tends to respond to upper cervical care, and how the gentle Knee Chest Upper Cervical technique addresses the structural and neurological factors that may be driving your symptoms.
What Is Meniere’s Disease?
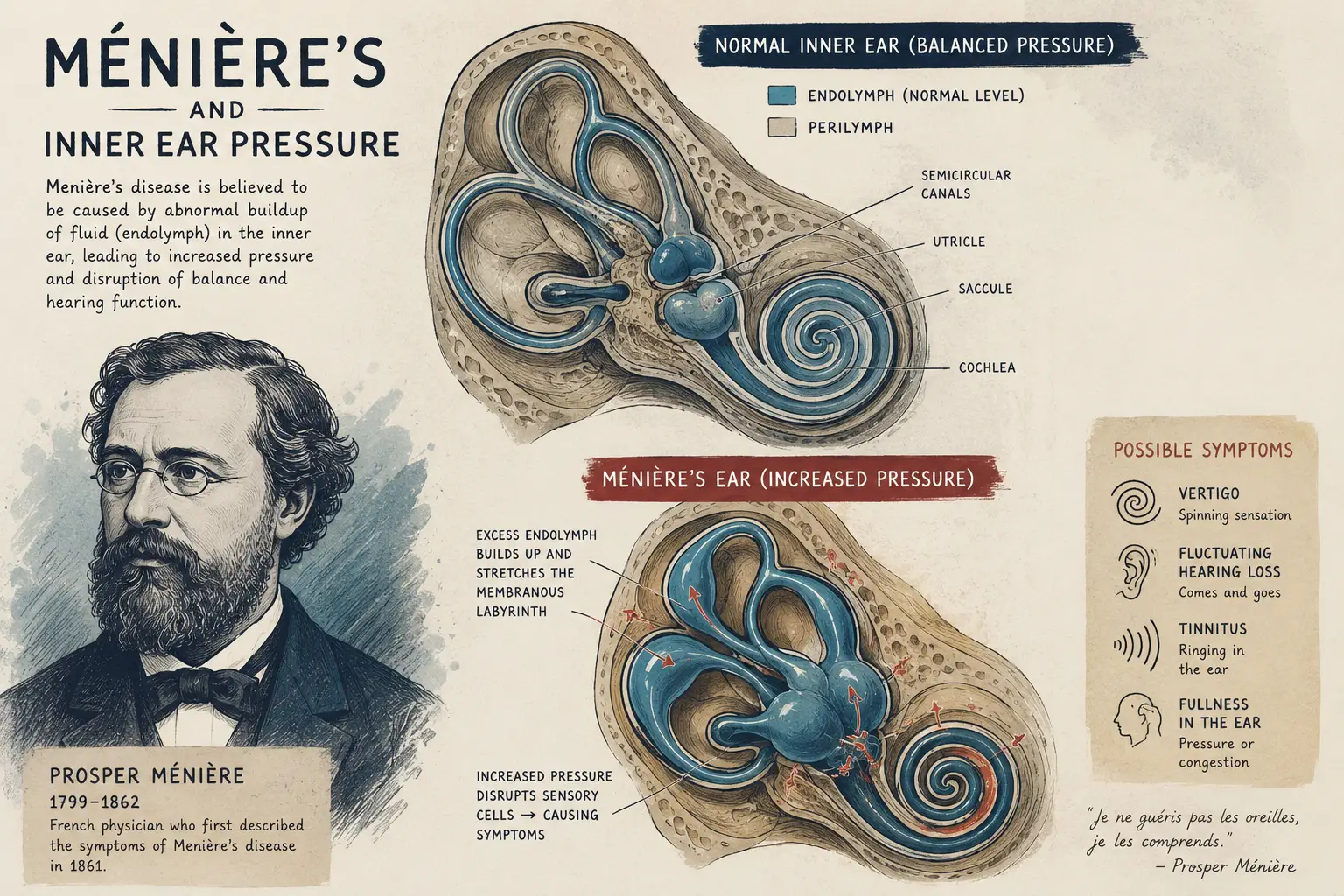
Meniere’s disease is a chronic inner ear disorder first described by French physician Prosper Ménière in 1861. According to the American Academy of Otolaryngology–Head and Neck Surgery diagnostic criteria, definite Meniere’s disease requires:
- Two or more spontaneous vertigo attacks lasting 20 minutes to 12 hours
- Documented sensorineural hearing loss at low to medium frequencies in the affected ear
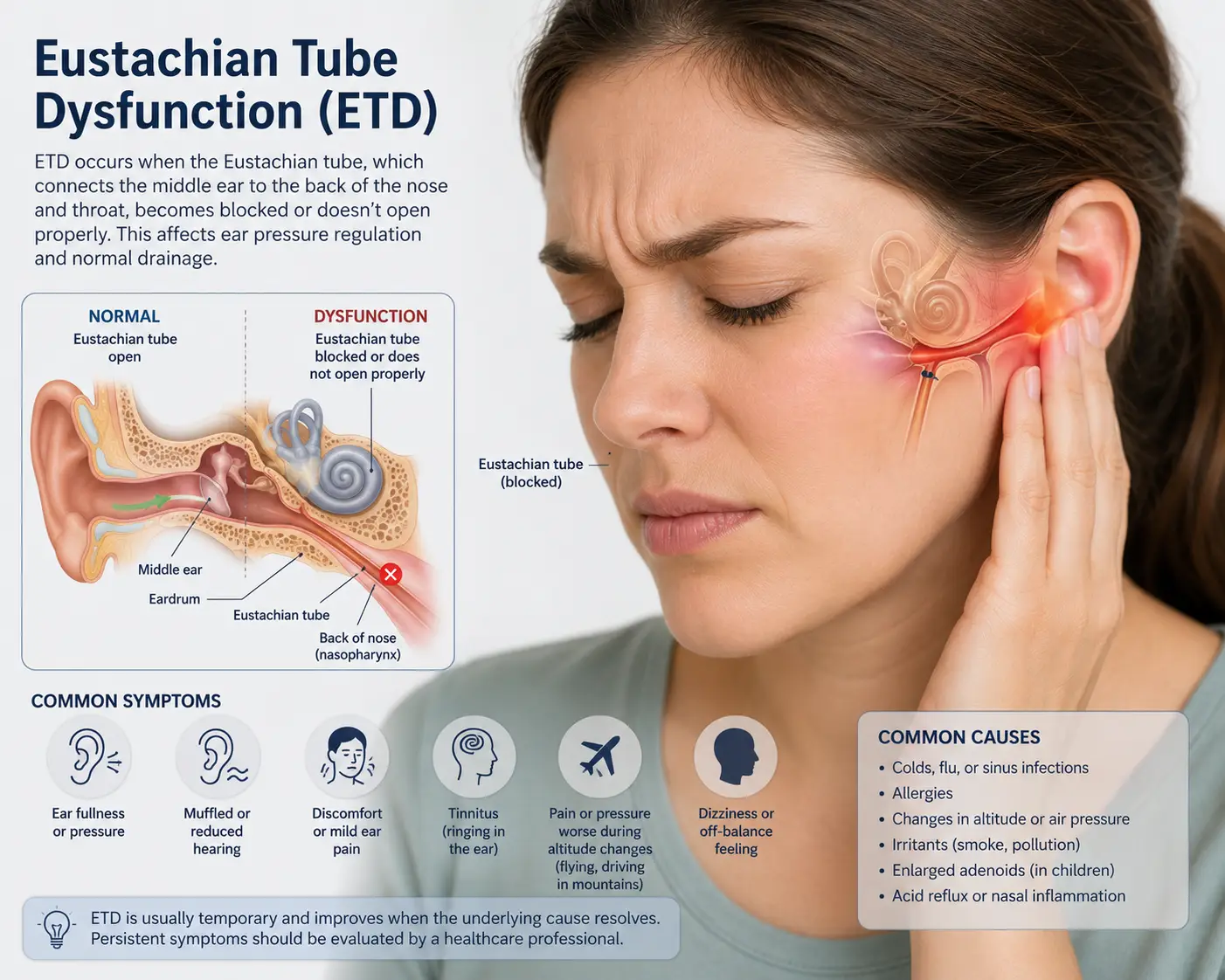
- Tinnitus or a feeling of fullness/pressure in the affected ear
- Other causes excluded
The four classic symptoms most patients describe as the “Meniere’s cluster”:
- Episodic vertigo — rotational dizziness that can last minutes to hours, often with nausea and vomiting
- Fluctuating hearing loss — typically low-frequency at first, progressing over years
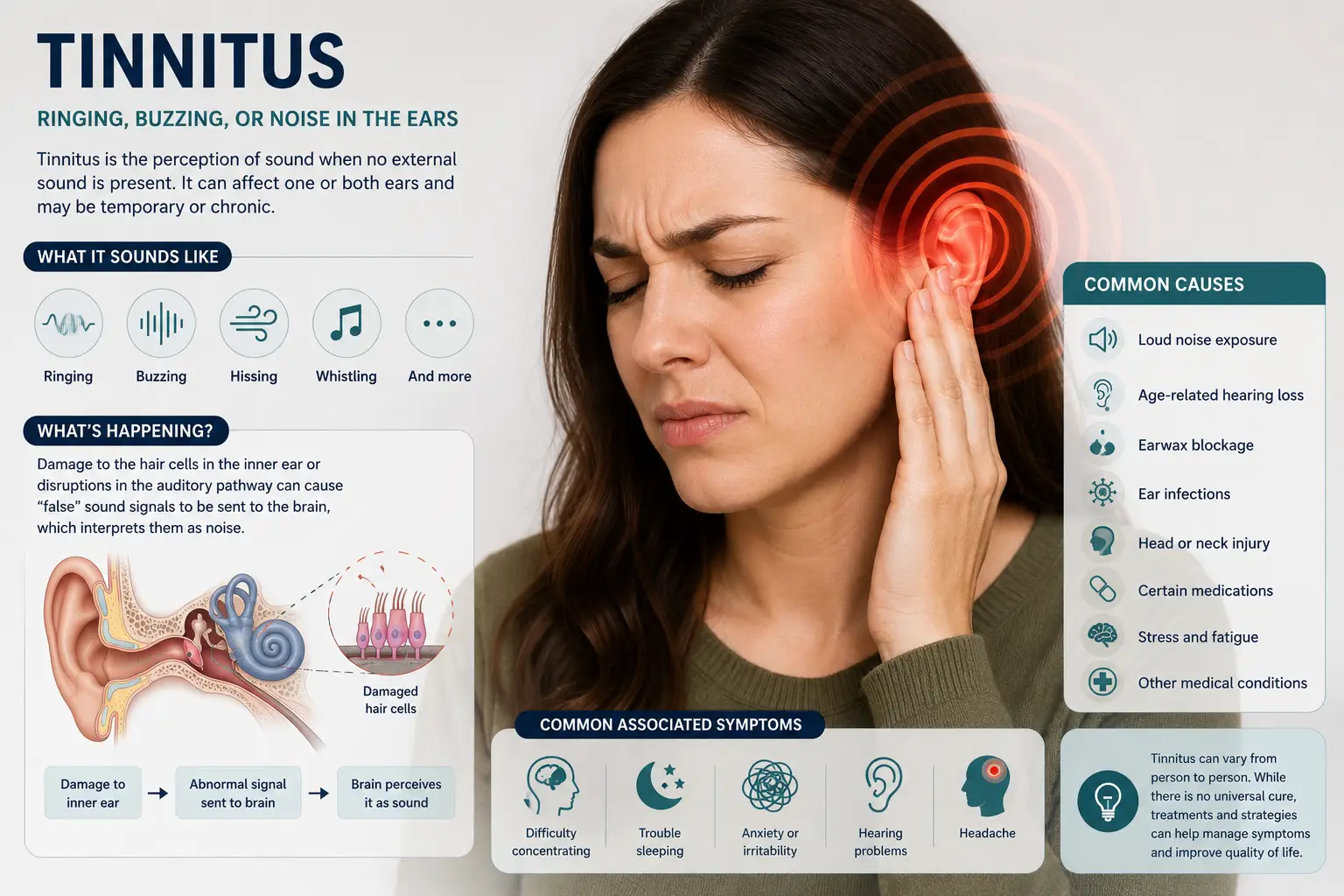
- Tinnitus — often a low-pitched roaring, buzzing, or seashell sound
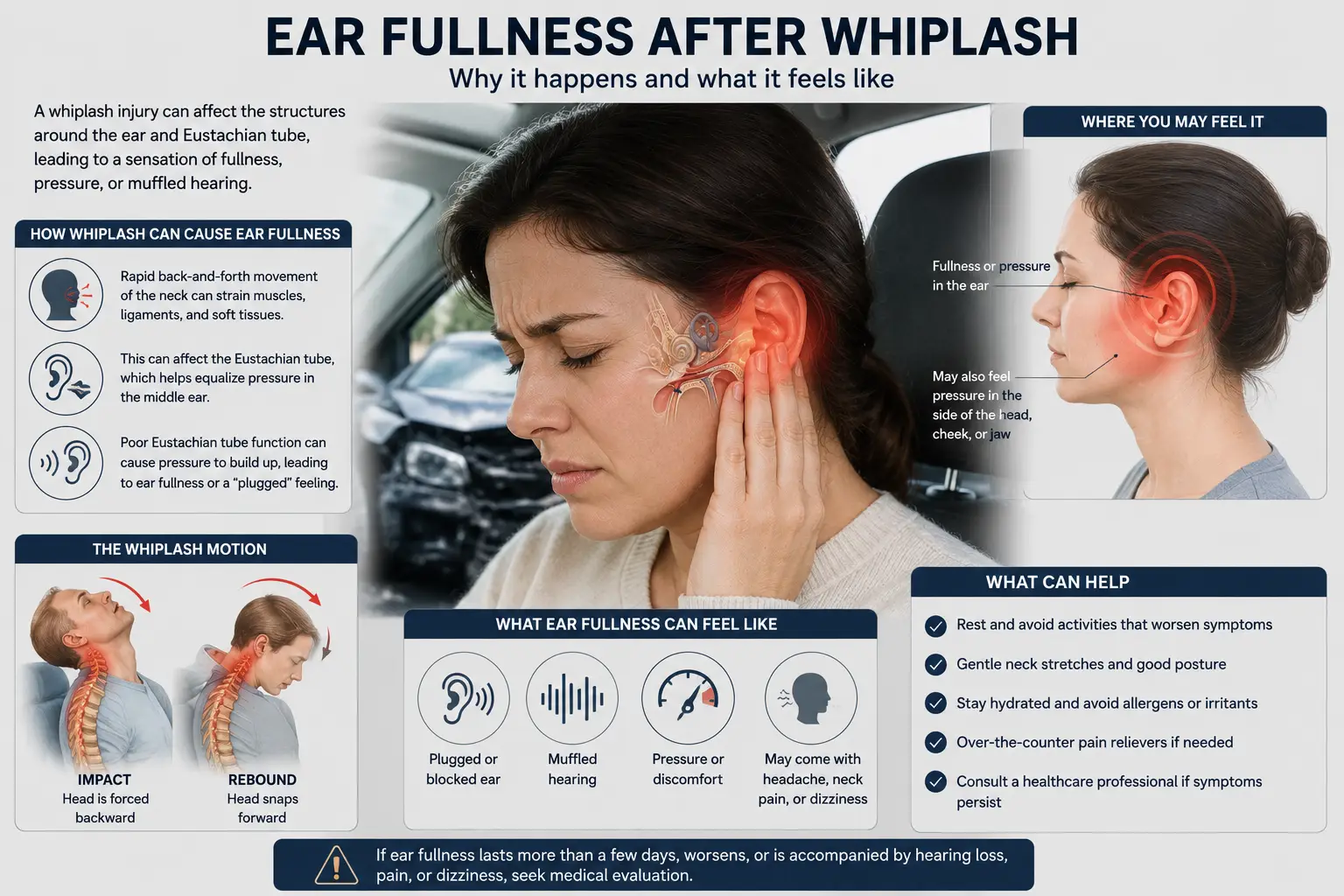
- Aural fullness — the deep, pressurized feeling that’s frequently the first warning sign of an impending attack
Prevalence and Burden
According to a large-scale prevalence study published in PubMed analyzing health claims data from over 60 million US patients, Meniere’s disease affects approximately 190 per 100,000 Americans — roughly 600,000 to 750,000 people nationwide — with prevalence climbing dramatically with age. The rate is just 9 per 100,000 in patients under 18 but rises to 440 per 100,000 in patients over 65. Meniere’s has a 1.89:1 female-to-male ratio and most commonly presents between ages 40 and 60.
That’s a lot of people living with a condition that conventional medicine acknowledges has no cure.
The Underlying Pathology: Endolymphatic Hydrops
The pathophysiological hallmark of Meniere’s disease is endolymphatic hydrops — an excessive buildup of fluid (endolymph) in the membranous labyrinth of the inner ear. A 2014 study in the American Journal of Neuroradiologyusing 3T MRI imaging detected endolymphatic hydrops in 95% of patients with definite Meniere’s disease, confirming the long-standing pathological understanding.
Here’s the critical question that gets ignored too often: what causes the endolymphatic hydrops in the first place?Conventional medicine still calls this “idiopathic” — meaning the cause is unknown. That’s where the upper cervical research becomes important.
The Anatomy: Why the Upper Neck Matters in Meniere’s
The atlas (C1) and axis (C2) sit at the base of the skull and surround the brainstem. This region is the structural and neurological gateway between the brain and the rest of the body — and it’s deeply interconnected with the inner ear, the vestibular system, blood flow to the brainstem, and the autonomic nervous system that regulates inner ear fluid balance.
When the atlas or axis is misaligned, several mechanisms can disrupt inner ear function:
1. Vertebral Artery Blood Flow
The vertebral arteries pass through the transverse foramina of the cervical vertebrae on their way to supply the brainstem and inner ear. Upper cervical misalignment can alter the geometry of these vessels and reduce blood flow to the labyrinth — affecting the endolymphatic balance that’s at the core of Meniere’s pathology.
2. The Eustachian Tube Connection
Dr. Michael Burcon’s research specifically describes how upper cervical misalignment can create irritation of the atlanto-occipital articulation, with swelling that puts pressure on adjacent middle ear structures including the Eustachian tube. Burcon’s hypothesis is that this contributes to the fluid pressure imbalance that drives endolymphatic hydrops.
3. The Autonomic Nervous System
Inner ear fluid regulation depends heavily on autonomic function — sympathetic and parasympathetic input that controls fluid production, secretion, and reabsorption. The atlanto-occipital region is densely involved with autonomic regulation. Upper cervical misalignment can compromise this regulation and contribute to inner ear fluid dysregulation over years and decades.
4. The Trigeminocervical Complex
The trigeminal nerve and upper cervical nerves converge in the brainstem at the trigeminocervical complex. Bartsch and Goadsby (2003) established this convergence in foundational research published in Current Pain and Headache Reports. Burcon specifically theorizes that this convergence creates a lesion affecting both the Eustachian tube and the trigeminal ganglion — establishing a neuroanatomical basis for the constellation of symptoms (vertigo, ear fullness, tinnitus, facial sensation changes) that defines Meniere’s.
5. Vagus Nerve Compromise
The vagus nerve exits the skull immediately adjacent to the atlas. Compromised vagal tone affects inflammation regulation throughout the head and neck — including the inner ear vasculature.
When these mechanisms work together, you have a plausible neurological explanation for what conventional medicine calls “idiopathic” endolymphatic hydrops.
The Whiplash–Meniere’s Connection
This is the most striking finding in the entire upper cervical chiropractic literature, and it deserves its own section.
In Burcon’s 2016 paper, every one of his 300 medically-diagnosed Meniere’s patients had a prior history of whiplash trauma. The average delay between the original whiplash injury and the onset of Meniere’s symptoms was approximately 15 years.
Read that again. Fifteen years on average between the car accident and the first vertigo attack.
This is precisely why the connection has been missed by conventional medicine for over a century. By the time symptoms appear, the patient has long forgotten the accident — or considers it irrelevant because they “recovered.” The upper cervical misalignment from that whiplash can sit silent for years, slowly disrupting autonomic regulation, blood flow, and trigeminocervical signaling until inner ear fluid balance finally fails and the diagnosis is made.
Burcon further notes that approximately half of these traumas were caused by motor vehicle accidents and approximately half from injuries involving head trauma — sports concussions, falls, blows to the head. In his clinical observation, 90% of patients showed an atlas listing of “posterior and inferior on the side opposite to the affected ear” — a striking pattern of structural specificity that suggests a real underlying mechanism, not coincidence.
For more on the post-trauma connection, see our car accident chiropractic care page.
How Lavender Family Chiropractic Approaches Meniere’s
At Lavender Family Chiropractic, we don’t treat Meniere’s directly — and we don’t claim to cure it. What we do is investigate whether upper cervical misalignment is a contributing factor in your specific case, and if it is, deliver a precise correction so your nervous system can function the way it’s designed to.
1. We Use 3D CBCT Imaging, Not Flat X-rays
Our office is equipped with a 3D Cone Beam Computed Tomography (CBCT) scanner. This gives us a true three-dimensional view of your upper cervical spine — something flat X-rays simply can’t provide. For Meniere’s patients, this matters because the misalignments we’re looking for are often subtle rotations of the atlas relative to the skull and axis — easily missed on standard imaging but clearly visible in 3D.
2. We Use the Knee Chest Upper Cervical Technique
Our doctors — Dr. Rusty Lavender and Dr. Jacob Temple — are trained in the Knee Chest Upper Cervical technique. You rest comfortably in a knee-chest position while we deliver a precise, low-force adjustment to the atlas or axis based on your individual imaging.
There’s no twisting, popping, or cracking. This matters enormously for Meniere’s patients, who often arrive with intense sensitivity to head and neck movement — even minor positional changes can trigger vertigo attacks. The Knee Chest technique is gentle enough for patients with active vertigo, post-concussion symptoms, or significant trauma history.
3. We Build Personalized Care Plans
Meniere’s disease that has been brewing for years — sometimes decades — doesn’t resolve in a single visit. We design personalized care plans based on your imaging, exam findings, attack frequency, and symptom history. Your plan is built to:
- Correct the upper cervical misalignment
- Stabilize the correction over weeks and months
- Allow the autonomic and vascular systems to recalibrate
- Transition you into long-term wellness care
Burcon’s research showed that meaningful improvement typically occurred within the first 4–6 weeks of consistent care, with sustained results over six years of follow-up. Your specific timeline depends on your imaging, history, and how your body responds.
Tired of Living in Fear of the Next Vertigo Attack?
You don’t have to keep wondering when the room will start spinning. Call Lavender Family Chiropractic at (941) 243-3729 to schedule your complimentary consultation. Dr. Rusty Lavender or Dr. Jacob Temple will sit down with you, look at your upper cervical spine, and tell you honestly whether the root cause of your Meniere’s symptoms might be in your neck.
What the Research Says About Meniere’s and Upper Cervical Care
This is where the research is strongest of any condition in our entire patient population.
The Burcon Studies
Dr. Michael Burcon has published the largest body of upper cervical chiropractic research on Meniere’s disease in existence. His landmark 2016 study in the Journal of Upper Cervical Chiropractic Research — “Health Outcomes Following Cervical Specific Protocol in 300 Patients with Meniere’s Followed Over Six Years” — produced these findings:
- 97% improvement in vertigo intensity, with mean self-reported vertigo scores dropping from 8.5 to below 1 on a 10-point scale
- All 300 patients had a prior history of whiplash trauma, with an average 15-year delay between injury and symptom onset
- 90% of patients showed an atlas listing of posterior and inferior on the side opposite the affected ear — suggesting a consistent structural pattern
- 97% of patients achieved control over vertigo within six weeks
Burcon has presented these findings to more than 2,000 ENT surgeons at venues including Cleveland Clinic, the House Ear Institute, the Prosper Meniere Society in Austria, and the Kyoto International Convention Center in Japan.
Additional Case-Level Evidence
A 2004 case report in the Journal of Manipulative and Physiological Therapeutics documented clinical improvement in a 75-year-old patient with longstanding vertigo, tinnitus, and hearing loss following upper cervical specific care — supporting the broader pattern of cervical-driven symptom improvement seen in Burcon’s larger cohort.
The Honest Limitations
We want to be transparent. Burcon’s research, while extensive, consists of case series rather than randomized controlled trials. The findings haven’t been replicated in large RCTs by independent research groups. Conventional medicine still considers Meniere’s “idiopathic” and treats it with sodium restriction, diuretics, betahistine, and procedural interventions.
What the evidence supports is this: for Meniere’s patients with a history of head or neck trauma — which Burcon’s data suggests may be the majority — gentle upper cervical correction can produce significant, lasting improvement in vertigo intensity, frequency, and quality of life. Not every patient will respond. That’s why we use 3D CBCT imaging and a thorough exam to determine whether your specific case fits the profile.
Upper cervical care doesn’t replace medical management — it complements it. Many of our Meniere’s patients continue working with their ENT and primary care provider while pursuing upper cervical care for the structural contribution that conventional medicine doesn’t address.
Lifestyle Habits That Support Meniere’s Management
While correcting upper cervical misalignment addresses a major structural contributor, these habits help reduce attack frequency and severity:
- Reduce sodium intake. The American Academy of Otolaryngology recommends keeping daily sodium under 1,500 mg. High sodium increases endolymph volume and pressure.
- Limit caffeine and alcohol. Both can trigger vertigo attacks in Meniere’s patients.
- Stay hydrated with plain water throughout the day. Counterintuitive but important — chronic dehydration can worsen Meniere’s symptoms.
- Manage stress aggressively. Stress is one of the most reliable triggers for vertigo attacks. Daily yoga, meditation, breathwork, or walking — pick one and commit.
- Get adequate sleep. Sleep deprivation lowers the threshold for vertigo attacks. Aim for 7–9 hours nightly.
- Avoid known triggers. Common triggers include MSG, aged cheeses, processed meats, and changes in barometric pressure. Keep an attack log to identify your patterns.
- Don’t smoke. Nicotine constricts inner ear blood flow.
- Track barometric pressure changes. Sarasota’s coastal climate brings frequent pressure changes that can trigger attacks. Some patients find pre-storm symptoms predictable enough to take precautions.
- Avoid stomach sleeping. Keeps your neck rotated for hours and aggravates upper cervical misalignment.
For Meniere’s patients whose symptoms include significant ear fullness and pressure, see our companion guide on ear pressure and upper cervical chiropractic for additional context.
Serving Sarasota and the Surrounding Communities
Lavender Family Chiropractic is located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — right at the corner of University and Whitfield. We’re easy to reach from anywhere on the Suncoast and proud to serve patients from across the region, including Bradenton, Lakewood Ranch, Parrish, Ellenton, Palmetto, University Park, Longboat Key, Siesta Key, Osprey, Venice, Myakka City, Ruskin, Tampa, and St. Petersburg.
If you’ve been managing Meniere’s disease for years without anyone evaluating your upper cervical spine, we’d love to help you investigate this missing piece.
Top 15 FAQs About Meniere’s Disease and Upper Cervical Care
1. Can chiropractic care really help Meniere’s disease?
For the right patient, yes — and the research base is more substantial here than for most conditions. Dr. Michael Burcon’s six-year follow-up of 300 Meniere’s patients showed 97% improvement in vertigo intensity after upper cervical specific care. The strongest candidates are patients with a history of head or neck trauma, which Burcon’s data suggests applies to a very high percentage of Meniere’s sufferers.
2. My ENT said Meniere’s has no cure. Is upper cervical care a cure?
We don’t make cure claims, and we’d be skeptical of anyone who does. What upper cervical care does, for the right patient, is address a structural and neurological contributor that conventional Meniere’s management doesn’t touch. Many patients experience dramatic reduction in attack frequency and intensity. Whether the underlying disease is “cured” or simply well-managed is a semantic question — what matters is quality of life.
3. Does the adjustment hurt?
No. The Knee Chest Upper Cervical technique uses light, specific pressure while you rest comfortably in a knee-chest position. There’s no twisting, popping, or cracking — which is especially important for Meniere’s patients who often can’t tolerate aggressive head and neck movement.
4. Will the adjustment trigger a vertigo attack?
We take this very seriously. Our gentle Knee Chest technique is specifically designed to avoid the abrupt head and neck movements that can trigger Meniere’s vertigo. Most patients tolerate the adjustment without any vertigo response. We adapt our approach based on your specific sensitivity.
5. I can’t remember being in a car accident. Could I still have an upper cervical misalignment?
Yes. Many patients have had trauma they don’t remember or didn’t consider significant — childhood falls, sports collisions, low-speed fender benders. Burcon’s data also showed that approximately half of his patients’ relevant traumas were from head impacts rather than classic motor vehicle whiplash. Our 3D CBCT imaging can identify misalignment regardless of whether you remember the original event.
6. How long until I notice improvement?
It varies. Burcon’s data showed 97% of patients gained control over vertigo within six weeks of consistent care. Some patients notice changes within the first few visits — others need several weeks. We’ll give you a realistic timeline based on your imaging and exam findings.
7. Do I have to stop my current Meniere’s treatment to try upper cervical care?
No. Upper cervical care complements medical management — it doesn’t replace it. We encourage you to continue working with your ENT and primary care provider. Many of our Meniere’s patients continue medications, dietary restrictions, and other treatments while pursuing upper cervical care.
8. Will my hearing come back?
The honest answer is: it depends. Hearing loss in Meniere’s is variable. Some patients experience improvement in hearing as the underlying fluid pressure normalizes. Others — particularly those with long-standing disease and significant damage to the cochlear hair cells — may see less change in hearing even with significant vertigo improvement. We can’t predict your specific response without seeing your imaging and history.
9. What about the ear fullness? Will that improve?
Aural fullness is often one of the first symptoms to respond to upper cervical care in Meniere’s patients. Many patients report dramatic reduction in the deep, pressurized feeling within weeks of starting care.
10. Do you accept insurance?
We’ll walk you through your options during your consultation. Our care plans are designed to make consistent, long-term care affordable regardless of insurance coverage.
11. What is 3D CBCT and why do you use it for Meniere’s?
3D Cone Beam Computed Tomography gives us a true three-dimensional view of your upper cervical spine. For Meniere’s patients this matters because the misalignments Burcon documented are subtle rotational shifts — clearly visible in 3D but often missed on standard X-rays.
12. Is upper cervical care safe if I’ve had ear surgery?
Generally yes. Burcon’s research included patients who had undergone various Meniere’s-related procedures, including vestibular nerve section. The Knee Chest technique doesn’t involve any direct contact with the ear itself — it adjusts the upper cervical spine.
13. What if my Meniere’s is bilateral?
Bilateral Meniere’s is more challenging than unilateral, but the upper cervical contribution still applies. Burcon’s data primarily focused on unilateral cases, but bilateral patients are still candidates for evaluation. Your specific situation would be discussed during your consultation.
14. Can children develop Meniere’s? Can they receive upper cervical care?
Meniere’s is rare in children (less than 3% of cases). However, children with chronic vertigo, tinnitus, ear fullness, or hearing concerns can still benefit from upper cervical evaluation. The Knee Chest technique is gentle enough for pediatric patients.
15. How do I get started?
Call (941) 243-3729 or book your complimentary consultation online. You’ll sit down with Dr. Rusty Lavender or Dr. Jacob Temple, talk through your Meniere’s history, attack patterns, prior trauma history, and current management, and find out whether upper cervical chiropractic is the right fit for you.
Ready to Investigate the Missing Piece? Call Lavender Family Chiropractic
You’ve been told Meniere’s disease is chronic, idiopathic, and incurable. The research from Dr. Michael Burcon and the upper cervical chiropractic community suggests that — for the majority of Meniere’s patients — there is a structural and neurological contribution from old head or neck trauma that conventional medicine has never investigated.
At Lavender Family Chiropractic, Dr. Rusty Lavender and Dr. Jacob Temple use precise 3D CBCT imaging and the gentle Knee Chest Upper Cervical technique to identify whether the upper cervical spine is contributing to your Meniere’s symptoms — and if it is, to correct it with the precision the condition demands.
You’re not stuck. The next attack doesn’t have to feel inevitable.
📞 Call (941) 243-3729 today 📅 Book your complimentary consultation online 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
Related Articles
- Ear Pressure and Upper Cervical Chiropractic: Relief Through Precision Care
- Ear Fullness After a Car Accident or Whiplash in Sarasota
- Clicking in My Ear and Pulsatile Tinnitus: The Upper Cervical Connection
By Dr. Rusty Lavender, DC | Lavender Family Chiropractic, Sarasota, FL