Tinnitus: If you’ve been told your tinnitus is “just something you have to live with,” there’s something your ENT may not have explained: a significant subset of tinnitus has nothing to do with damage inside your ear. It comes from your neck. Specifically, from how your upper cervical spine sends signals to a region of your brainstem called the dorsal cochlear nucleus — the same region that processes the sound you actually hear from the outside world.
This isn’t fringe theory. It’s been called somatic (or somatosensory) tinnitus in the peer-reviewed literature since Dr. Robert Levine’s foundational 1999 paper in the American Journal of Otolaryngology. And for the patients we see at Lavender Family Chiropractic in Sarasota, Florida, understanding this distinction is often the difference between years of frustration and finally getting somewhere.
In this guide, we’ll walk through what this condition actually is, why the upper cervical spine is so often a hidden driver, what the published research really shows, and how the gentle Knee Chest Upper Cervical technique used at Lavender Family Chiropractic addresses the root cause for the right patient.
What Is Tinnitus?
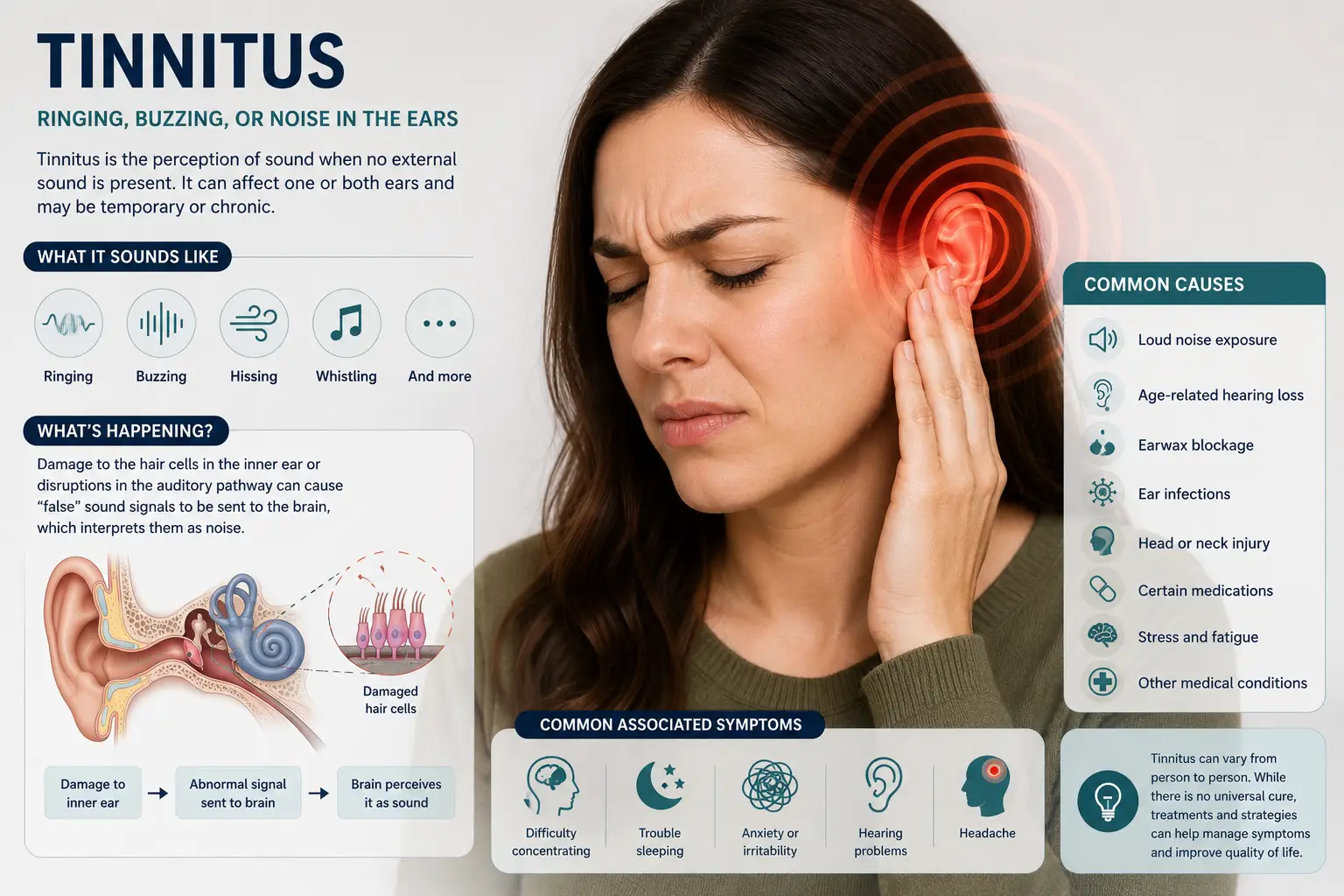
Tinnitus is the perception of sound when no external sound is present. People describe it dozens of ways:
- Ringing
- Buzzing
- Hissing
- Whooshing
- Clicking
- Pulsing
- Roaring
- Humming
- A high-frequency tone like a TV left on
It can be in one ear, both ears, or seem to come from inside your head. It can be constant or intermittent, mild or maddening. According to a 2024 study published in The Lancet Regional Health – Americas, the prevalence of tinnitus in the United States is approximately 11.2% — roughly 27 million adults. More recent NHANES data from a 2025 cross-sectional analysis put the figure at 17.2% of US adults, with prevalence rising sharply with age (10.5% in adults 20–39 vs. 24.7% in those over 60).
That’s millions of people walking around with sound they can’t escape. And for many of them, the cause isn’t where they’ve been told to look.
The Two Categories
Ringing generally falls into two categories:
- Subjective tinnitus — only the patient hears it. This is by far the most common type and includes most ringing, buzzing, and hissing.
- Objective tinnitus — rare, and sometimes audible to a clinician with a stethoscope. Usually caused by vascular or muscular issues (turbulent blood flow, muscle spasms in the middle ear).
Within subjective tinnitus, there’s an important subtype that often gets overlooked: somatic (somatosensory) tinnitus.
Somatic Tinnitus: The Neck-Driven Subtype Most Patients Have Never Heard Of
In 1999, Dr. Robert Levine published a landmark paper in the American Journal of Otolaryngology describing a specific population of patients with a unique set of features:
- An associated somatic (musculoskeletal) disorder of the head or upper neck
- Symptoms localized to the ear on the same side as the somatic problem
- No vestibular complaints
- Normal neurological exam findings
- Symmetric, normal-range hearing on audiometry
These patients didn’t fit the classic noise-induced or age-related profile. Their symptoms changed with neck movement, jaw clenching, or pressure on certain muscles — meaning the auditory perception was being modulated by somatosensory input from the cervical spine and craniofacial region.
Levine called this somatic (craniocervical) tinnitus and proposed that it was caused by disinhibition of the dorsal cochlear nucleus (DCN) — a brainstem region that integrates somatosensory (touch, position, and movement) input with auditory input.
In other words: when the upper neck sends abnormal signals to the brainstem, the brainstem region that processes hearing can start generating phantom sound.
How Cervical Input Reaches the Auditory Brainstem
Multiple peer-reviewed studies have confirmed this neuroanatomical connection:
- Zhan, Pongstaporn, and Ryugo (2006) traced anatomical projections from the second cervical (C2) dorsal root ganglion directly to the cochlear nucleus in rats — establishing a hard-wired anatomical pathway from the upper neck to the auditory brainstem.
- Shore and colleagues (2008) demonstrated that dorsal cochlear nucleus responses to somatosensory stimulation become enhanced after noise-induced hearing loss — meaning the brainstem becomes more sensitive to neck input precisely when peripheral hearing is compromised.
- Bressi and colleagues (2017) proposed the “triple hypothesis” in Medical Hypotheses: cervical spine disorders can generate tinnitus through (1) stimulation of dorsal spinal cord roots feeding the dorsal cochlear nucleus, (2) inner ear blood flow impairment via vertebral artery alterations, and (3) trigeminal nerve irritation.
The takeaway is that the neuroscience supports what chiropractors and physiotherapists have observed clinically for decades: in a meaningful subset of patients, the noise originates in the neck, not the ear.
The Anatomy of the Upper Neck and Why It Matters for Tinnitus
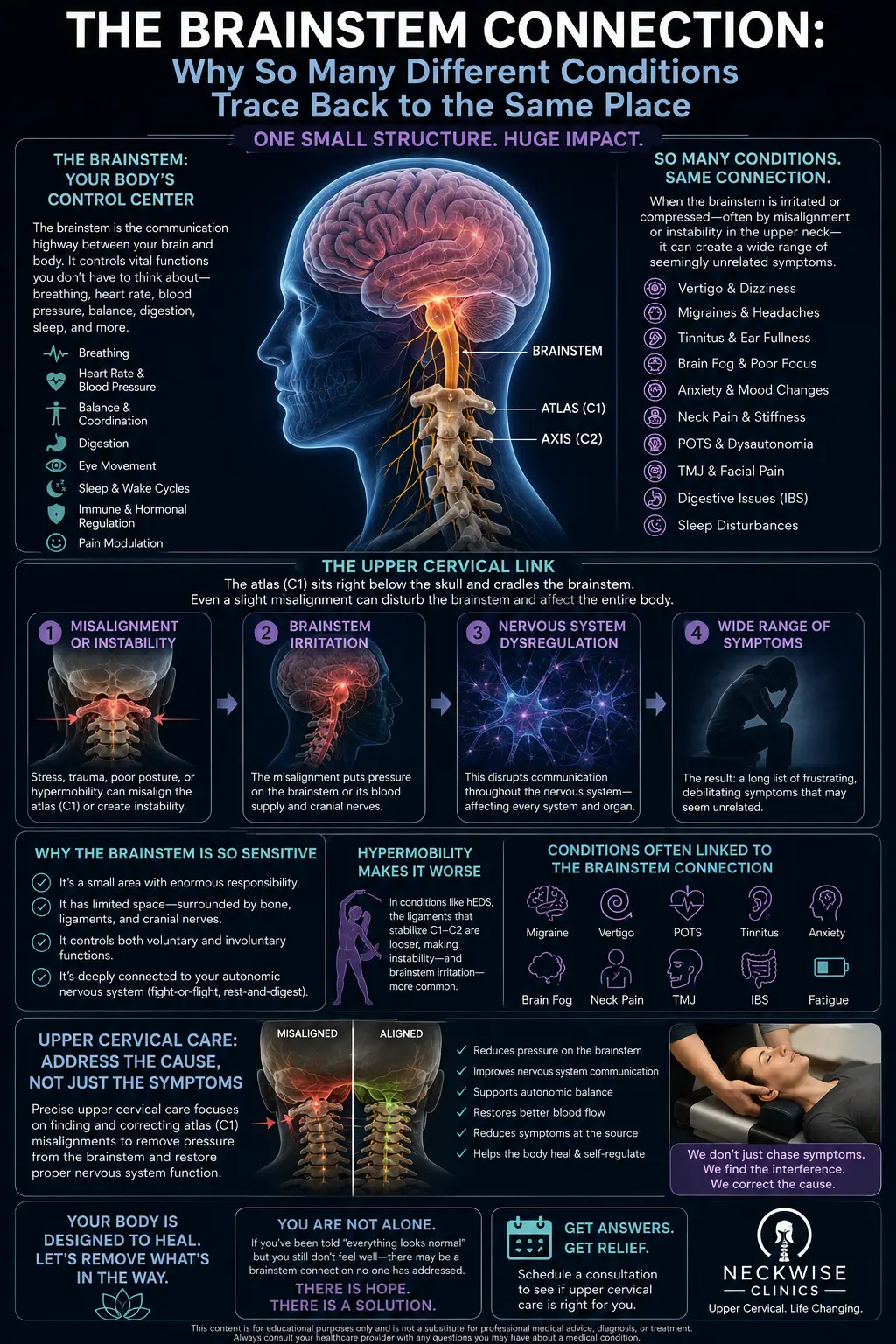
The atlas (C1) and axis (C2) sit at the base of your skull and surround the brainstem. This region is the structural and neurological gateway between your brain and the rest of your body — and it’s deeply interconnected with everything that controls hearing, balance, blood flow to the inner ear, and somatosensory integration.
A misalignment here — even a millimeter or two — can:
- Disrupt C1, C2, and C3 nerve signaling, feeding abnormal somatosensory input into the dorsal cochlear nucleus
- Irritate the trigeminocervical complex, where upper cervical and trigeminal nerve signals converge
- Compromise vagus nerve function, since the vagus nerve exits the skull right next to the atlas
- Restrict vertebral artery blood flow to the brainstem and inner ear, contributing to vascular contributions to tinnitus
- Disturb cerebrospinal fluid flow around the brainstem
- Increase suboccipital muscle tension that further aggravates somatic input
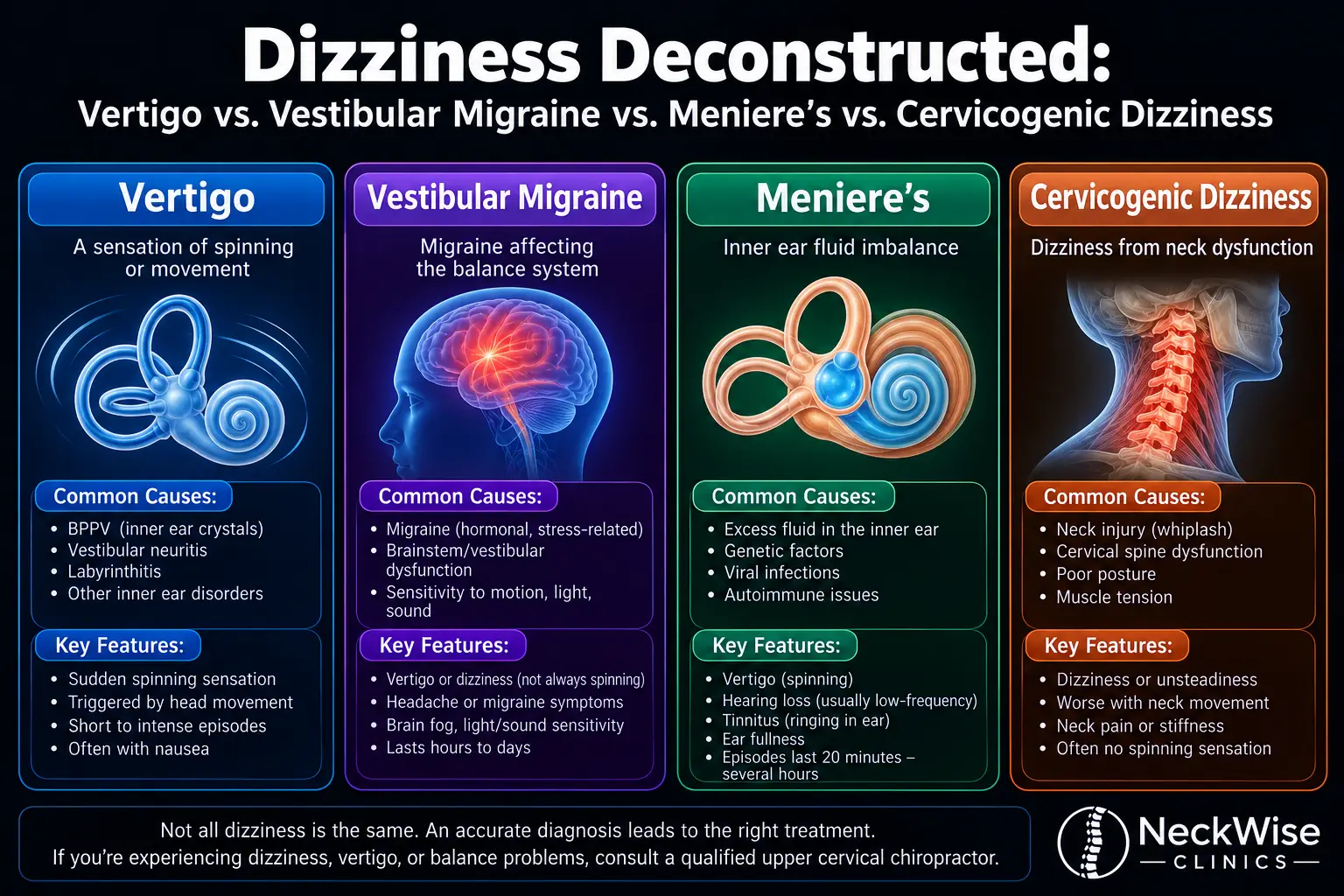
When you stack these mechanisms together, you understand why these symptoms so often coexists with TMJ dysfunction, vertigo, ear pressure, Meniere’s disease, and headaches — and why a precise upper cervical correction often addresses several of them simultaneously.
The Trauma Connection: Why Whiplash Often Precedes Tinnitus
This is one of the most underappreciated patterns in the literature. A history of head or neck trauma — even decades earlier — is a major risk factor for chronic tinnitus, particularly somatic tinnitus.
Levine’s original 1999 paper specifically called out whiplash and temporomandibular joint syndrome as the two non-auditory sensory conditions most clearly linked to this condition. Dr. Michael Burcon’s 2016 follow-up paper in the Journal of Upper Cervical Chiropractic Research followed 300 patients with Meniere’s disease (which includes tinnitus as a core symptom). All 300 patients had a prior history of whiplash trauma, with an average 15-year delay between the original injury and the onset of symptoms.
Common trauma sources we see in our Sarasota patients include:
- Motor vehicle accidents — even low-speed rear-end collisions
- Sports concussions, especially repeat exposures
- Falls — stairs, bicycles, slips on wet surfaces
- Difficult births (forceps or vacuum-assisted deliveries)
- Repetitive head impact activities — football, soccer, hockey, gymnastics
If you’ve had any of these and now live with chronic ringing, the connection is worth investigating. See our page on car accident chiropractic care for more on the post-trauma neurological cascade.
How Lavender Family Chiropractic Approaches Tinnitus
At Lavender Family Chiropractic, we don’t treat it directly — and we don’t claim to cure it. What we do is investigate whether upper cervical misalignment is a contributing factor in your case, and if it is, deliver a precise correction so your nervous system can function the way it’s designed to.
Here’s what makes our approach different.
1. We Use 3D CBCT Imaging, Not Flat X-rays
Our office is equipped with a 3D Cone Beam Computed Tomography (CBCT) scanner. This gives us a true three-dimensional view of your upper cervical spine — something flat X-rays simply can’t provide. We can see exactly how your atlas and axis are positioned, the angle and degree of misalignment, and the specific correction your spine needs.
For patients this matters because the misalignments we’re looking for are often subtle and rotational — easily missed on conventional imaging.
2. We Use the Knee Chest Upper Cervical Technique
Our doctors — Dr. Rusty Lavender and Dr. Jacob Temple — are trained in the Knee Chest Upper Cervical technique. You rest comfortably in a knee-chest position while we deliver a precise, low-force adjustment to the atlas or axis based on your individual imaging.
There’s no twisting, popping, or cracking. Just a specific, gentle correction. The Knee Chest technique is gentle enough for children, seniors, and patients with sensitive conditions like Ehlers-Danlos syndrome or post-concussion symptoms.
3. We Build Personalized Care Plans
Ringing that’s been brewing for years — especially when tied to old trauma — doesn’t resolve in a single visit. We design personalized care plans based on your imaging, exam findings, and symptom history. Your plan is built to:
- Correct the upper cervical misalignment
- Hold the correction over time
- Allow your nervous system to recalibrate
- Transition you into long-term wellness care
We explain your plan completely before you commit to anything. To learn more about our approach, visit Meet the Team or see What to Expect at your first visit.
Who Is the Best Candidate for Upper Cervical Care?
Honest answer: not everyone. Upper cervical care tends to help most when the tinnitus has features pointing toward a somatic origin. The strongest candidates are patients whose symptoms:
- Changes with neck movement, head position, jaw clenching, or pressure on the suboccipital muscles
- Localizes to one ear (especially on the side of known neck or jaw issues)
- Coexists with neck pain, headaches, TMJ symptoms, vertigo, or ear pressure
- Started or worsened after head or neck trauma
- Has a normal or near-normal audiogram
- Hasn’t responded fully to conventional ENT treatment
If your symptoms features fit several of these, the upper cervical pathway is worth exploring. If it doesn’t, we’ll tell you that honestly — and refer you elsewhere.
Tired of the Ringing, Buzzing, or Hissing?
You don’t have to keep living with it. Call Lavender Family Chiropractic at (941) 243-3729 to schedule your complimentary consultation. Dr. Rusty Lavender or Dr. Jacob Temple will sit down with you, look at your upper cervical spine, and tell you honestly whether the root cause of your ringing might be in your neck.
What the Research Says About Upper Cervical Care and Tinnitus
The peer-reviewed evidence linking the cervical spine to tinnitus is more extensive than most patients realize. Here’s what the literature actually shows.
The Somatic Tinnitus Framework
- Levine (1999) in the American Journal of Otolaryngology — the foundational paper proposing somatic (craniocervical) tinnitus and the dorsal cochlear nucleus hypothesis. Identified the clinical features that distinguish somatic tinnitus from other subtypes.
- Levine, Nam, Oron, and Melcher (2007) in Progress in Brain Research — provided evidence for a tinnitus subgroup responsive to somatosensory-based treatments.
- Ralli and colleagues (2017) — a comprehensive review summarizing current evidence on somatosensory tinnitus modulation.
Neuroanatomical Evidence
- Zhan, Pongstaporn, and Ryugo (2006) in the Journal of Comparative Neurology — anatomically documented direct projections from the C2 dorsal root ganglion to the cochlear nucleus.
- Shore, Koehler, Oldakowski, Hughes, and Syed (2008) in the European Journal of Neuroscience — showed dorsal cochlear nucleus responses to somatosensory stimulation are enhanced after noise-induced hearing loss.
- Bressi and colleagues (2017) in Medical Hypotheses — proposed the “triple hypothesis” connecting cervical spine disorders to tinnitus through DCN stimulation, vertebral artery blood flow alterations, and trigeminal irritation.
Treatment Outcome Studies
- Cherian, Cherian, Cook, and Kaltenbach (2013) in the Journal of the American Academy of Audiology — documented improvement in tinnitus following mechanical treatment of the cervical spine and jaw in a defined subgroup of tinnitus patients.
- Burcon (2016) in the Journal of Upper Cervical Chiropractic Research — followed 300 Meniere’s patients (with tinnitus as a core symptom) over six years of upper cervical specific care, reporting 97% improvement in vertigo intensity and substantial improvement in associated tinnitus.
- A 2004 case report in the Journal of Manipulative and Physiological Therapeutics documented clinical improvement in a 75-year-old patient with longstanding vertigo, tinnitus, and hearing loss following upper cervical-specific chiropractic care.
The Honest Limitations
Tinnitus research has well-known challenges. Most studies are case reports or small case series. Randomized controlled trials of upper cervical chiropractic specifically for tinnitus are limited. The neuroanatomy and case-level evidence are compelling — but the larger trials needed to definitively establish effect size haven’t yet been conducted.
What the evidence supports is this: a defined subset of tinnitus patients (somatic tinnitus) shows measurable response to cervical-focused interventions. The challenge clinically is identifying which patients fall into that subset — which is exactly what our exam, history, and 3D CBCT imaging are designed to do.
Lifestyle Habits That Support Tinnitus Relief
While correcting upper cervical misalignment addresses the structural and neurological root cause, these habits help reduce nervous system irritation, support brain health, and accelerate your results:
- Protect your hearing. Wear ear protection around loud machinery, concerts, and power tools. Noise-induced hearing loss makes the dorsal cochlear nucleus more sensitive to neck input — exactly what you don’t want.
- Improve your sleep. Tinnitus and poor sleep feed each other. A 2024 NHANES analysis found short sleep, long sleep, and sleep disturbances all significantly increase tinnitus risk. Aim for 7–9 hours nightly.
- Reduce caffeine and alcohol. Both can intensify tinnitus perception in sensitive individuals.
- Manage stress. Chronic stress tightens the suboccipital and TMJ-region muscles, increasing somatic input to the dorsal cochlear nucleus.
- Stop smoking. Tobacco constricts inner ear blood flow and is consistently associated with higher tinnitus prevalence.
- Maintain a healthy weight. The 2025 NHANES analysis found obesity independently increases tinnitus risk by approximately 35%.
- Avoid stomach sleeping. Hours of rotated neck position aggravates upper cervical misalignment.
- Practice gentle neck mobility daily. Slow rotations, side-bends, and chin tucks — never aggressive cracking or self-manipulation.
For patients whose tinnitus is whooshing or pulsatile (and tied to blood flow), see our companion guide on clicking in my ear and pulsatile tinnitus for the vascular angle on the same problem.
Serving Sarasota and the Surrounding Communities
Lavender Family Chiropractic is located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — right at the corner of University and Whitfield. We’re easy to reach from anywhere on the Suncoast and proud to serve patients from across the region, including Bradenton, Lakewood Ranch, Parrish, Ellenton, Palmetto, University Park, Longboat Key, Siesta Key, Osprey, Venice, Myakka City, Ruskin, Tampa, and St. Petersburg.
If you’ve been chasing tinnitus from one ENT to the next with no answers, we’d love to help you investigate whether the upper cervical spine is involved. See more about the areas we service and the conditions we help at our practice.
Top 15 FAQs About Tinnitus and Upper Cervical Care
1. Can a chiropractor really help tinnitus?
For the right patient, yes. We don’t treat tinnitus directly, but when upper cervical misalignment is contributing to somatic (cervically-driven) tinnitus, correcting that misalignment can produce meaningful improvement. The evidence is strongest for patients whose tinnitus changes with neck movement, jaw activity, or pressure on the head and neck muscles.
2. What’s the difference between somatic tinnitus and regular tinnitus?
Somatic (or somatosensory) tinnitus is a subtype where the sound is modulated by input from the neck or jaw rather than originating in the inner ear. Patients with somatic tinnitus can often change the volume, pitch, or character of their tinnitus by turning their head, clenching their jaw, or pressing on certain muscles.
3. How do I know if my tinnitus is somatic?
Common clues include: tinnitus that changes with head or jaw movement, coexists with neck pain or TMJ issues, started after head or neck trauma, localizes to one ear, and shows a normal audiogram. Our consultation and exam help identify which subtype is most likely in your case.
4. Does the adjustment hurt?
No. The Knee Chest Upper Cervical technique uses light, specific pressure while you rest comfortably in a knee-chest position. There’s no twisting, popping, or cracking. Most patients describe it as gentle and surprisingly subtle.
5. How long until I notice changes in my tinnitus?
It varies widely. Some patients notice changes within the first few visits — others need several weeks of consistent care, especially with long-standing tinnitus tied to old trauma. We’ll give you a realistic timeline based on your imaging and exam findings.
6. My ENT said there’s nothing wrong with my hearing. Can chiropractic still help?
That’s actually a good sign for somatic tinnitus candidates. A normal audiogram alongside tinnitus is one of Levine’s classic features of cervically-driven tinnitus — meaning the noise is being generated centrally (in the brainstem) rather than from peripheral hearing damage. These patients often respond best to cervical-focused care.
7. Will my tinnitus come back if I stop coming?
Holding the correction is the goal. That’s why we build personalized care plans designed to stabilize the upper cervical correction over time. Patients who complete the corrective phase and follow through with wellness care tend to see the longest-lasting results.
8. I had a car accident years ago — could that be causing my tinnitus today?
Possibly. The research consistently links head and neck trauma to chronic tinnitus, often with a long delay between the original injury and symptom onset. Dr. Burcon’s research found that all 300 of his Meniere’s patients (a closely related condition) had a prior whiplash history, with an average 15-year delay before symptoms began.
9. Is upper cervical care safe for older adults with tinnitus?
Yes. The Knee Chest technique is gentle enough for seniors, including those with osteoporosis, arthritis, or other sensitive conditions. We adapt our approach based on each patient’s age, history, and tolerance.
10. Do you accept insurance?
We’ll walk you through your options during your consultation. Our care plans are designed to make consistent, long-term care affordable regardless of insurance coverage.
11. What is 3D CBCT and why do you use it for tinnitus?
3D Cone Beam Computed Tomography gives us a true three-dimensional view of your upper cervical spine. For tinnitus patients this matters because the misalignments contributing to somatic tinnitus are often subtle — easily missed on standard X-rays but clearly visible in 3D.
12. Can stress make my tinnitus worse?
Absolutely. Stress tightens the suboccipital muscles at the base of your skull and increases somatosensory input to the dorsal cochlear nucleus — which can literally make your tinnitus louder. Stress management is part of every tinnitus care plan we build.
13. Will my tinnitus be cured?
We don’t make cure claims, and we’d be suspicious of anyone who does. What we can say is that many of our tinnitus patients experience meaningful improvement — reduced intensity, fewer flares, less impact on sleep and daily life — when upper cervical misalignment is a contributing factor and it’s properly corrected. The honest answer is: we’ll know more after your imaging and exam.
14. What if my tinnitus is from noise-induced hearing loss?
Noise-induced hearing loss is a peripheral problem, and we can’t reverse cochlear hair cell damage. However, research from Shore et al. (2008) shows that the dorsal cochlear nucleus actually becomes more sensitive to neck input after noise-induced hearing loss — meaning that even when the original injury was acoustic, the cervical contribution to ongoing tinnitus perception can still matter.
15. How do I get started?
Call (941) 243-3729 or book your complimentary consultation online. You’ll sit down with Dr. Rusty Lavender or Dr. Jacob Temple, talk through your symptoms, and find out whether upper cervical chiropractic is the right fit for you.
Ready to Investigate the Root Cause? Call Lavender Family Chiropractic
You don’t have to accept that your tinnitus is permanent or untreatable. For a meaningful subset of tinnitus sufferers — particularly those with somatic features, a history of trauma, or coexisting neck and jaw issues — the upper cervical spine is the missing piece no one has investigated.
At Lavender Family Chiropractic, Dr. Rusty Lavender and Dr. Jacob Temple use precise 3D CBCT imaging and the gentle Knee Chest Upper Cervical technique to identify whether the upper cervical spine is contributing to your tinnitus — and if it is, to correct it with the precision the condition demands.
📞 Call (941) 243-3729 today 📅 Book your complimentary consultation online 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
Related Articles
- Ear Pressure and Upper Cervical Chiropractic: Relief Through Precision Care
- Eustachian Tube Dysfunction in Sarasota: How Upper Cervical Care Addresses the Root Cause
- Clicking in My Ear and Pulsatile Tinnitus: The Vascular Side of the Connection
By Dr. Rusty Lavender, DC | Lavender Family Chiropractic, Sarasota, FL