By Dr. Rusty Lavender and Dr. Jacob Temple
Bell’s palsy in Sarasota: Few conditions are as frightening as waking up one morning, looking in the mirror, and realizing half of your face won’t move. The corner of your mouth droops. Your eyelid won’t close all the way. When you try to smile, only one side responds. Eating becomes a struggle, drinking spills out of the corner of your lips, and you can’t quite tell if you’re having a stroke or losing your mind. For most people who experience this, the answer is neither. It is Bell’s palsy — a sudden, often dramatic paralysis of the facial nerve that affects tens of thousands of Americans every year.
At Lavender Family Chiropractic in Sarasota, Florida, we see patients with Bell’s palsy at every stage of the condition — those in the acute phase desperate for answers, those a few months in who have been told to “just wait it out,” and those years past the original onset who are still living with residual weakness, synkinesis, twitching, or facial asymmetry that no one in conventional medicine has been able to address.
Through the precise, gentle Knee Chest Upper Cervical technique used by Dr. Rusty Lavender and Dr. Jacob Temple, we work to address one of the most overlooked contributors to facial nerve dysfunction: the relationship between the upper cervical spine, the brainstem, and the cranial nerves that originate there.
This guide is for anyone in Sarasota, Bradenton, Lakewood Ranch, or the surrounding areas who is searching for a deeper understanding of Bell’s palsy — what it actually is, why it happens, why some patients recover fully and others don’t, and why the upper cervical spine may be the missing piece in your healing puzzle. By the end, you’ll understand exactly why this condition responds to upper cervical care, what to expect from a consultation, and how to take the next step.
What Is Bell’s Palsy?
Bell’s palsy is an acute, idiopathic paralysis of the seventh cranial nerve — the facial nerve — that causes sudden weakness or complete paralysis of the muscles on one side of the face. The word “idiopathic” simply means that medicine has not been able to pin down a single, definitive cause. It is named after Sir Charles Bell, the Scottish anatomist who first described the condition in detail in the early 1800s.
The facial nerve, or cranial nerve VII, controls nearly every muscle of facial expression. It governs the ability to smile, frown, raise the eyebrows, close the eyes, puff the cheeks, and form words. It also carries fibers that influence taste on the front two-thirds of the tongue, regulates tear production, and modulates the stapedius muscle in the middle ear, which protects the eardrum from loud sounds. When the facial nerve becomes inflamed, compressed, or otherwise impaired, all of these functions can be disrupted at once.
The classic presentation is unmistakable. Symptoms typically appear suddenly — sometimes overnight, often peaking within 48 to 72 hours. One side of the face droops. The corner of the mouth pulls down. The eye on the affected side may not close fully, leading to dryness, irritation, or excessive tearing. Patients often experience pain behind the ear in the day or two before paralysis sets in. Some report a strange metallic or altered taste, hypersensitivity to sound (hyperacusis), or numbness around the face — though true sensory loss is rare and usually suggests another diagnosis.
Bell’s palsy is the most common cause of acute unilateral facial paralysis, accounting for roughly 60 to 75 percent of all cases. Population studies estimate an annual incidence between 15 and 30 cases per 100,000 people, with a lifetime risk of approximately one in 60. A large 2025 analysis of US claims data found the incidence climbing — averaging 24.5 cases per 100,000 adults annually between 2007 and 2022, with a measurable upward trend over that period. Recurrence happens in roughly 4 to 14 percent of patients, and bilateral cases (paralysis on both sides) are rare, accounting for less than 1 percent of presentations.
The condition affects both sexes roughly equally, though pregnant women — particularly in the third trimester — face a threefold increased risk. People with diabetes, hypertension, obesity, and a history of certain viral infections (especially herpes simplex) are also at elevated risk. The peak age range is between 20 and 40, but Bell’s palsy occurs across the lifespan, including in children and in adults over 70.
The conventional medical understanding is that Bell’s palsy is most often caused by reactivation of the herpes simplex virus, which lies dormant in the geniculate ganglion of the facial nerve. When the virus reactivates, the resulting inflammation causes the nerve to swell within the narrow bony canal it travels through in the temporal bone — the facial canal, also called the aqueductus fallopii.
Because the nerve has nowhere to expand, the swelling itself compresses the nerve fibers, leading to ischemia (lack of blood flow), demyelination, and loss of motor function. Standard treatment focuses on reducing this inflammation as quickly as possible with corticosteroids, sometimes combined with antiviral medications.
But this story, while accurate, is incomplete. It explains the immediate biology of the nerve swelling — but it does not fully explain why some patients recover completely while others are left with permanent deficits, why certain populations are more vulnerable, or why recurrence happens at all. To understand the full picture, we have to look beyond the facial nerve itself and consider the broader neuroanatomical context in which it functions — including the upper cervical spine.
The Facial Nerve and the Upper Cervical Spine: A Connection Most Doctors Miss
To understand why upper cervical chiropractic care may help patients with Bell’s palsy, it is essential to understand the anatomical relationships between the facial nerve, the brainstem, and the top of the cervical spine.
The facial nerve originates in the pons, a portion of the brainstem that sits just above the spinal cord and just below the midbrain. The motor nucleus of the facial nerve — the cluster of neurons that drive facial muscle movement — lies deep within the lower pons. From there, the nerve fibers loop around the abducens nucleus (which controls lateral eye movement), exit the brainstem at the cerebellopontine angle, and travel through the internal acoustic meatus before passing through the facial canal in the temporal bone and emerging at the stylomastoid foramen, where the nerve branches to innervate the muscles of facial expression.
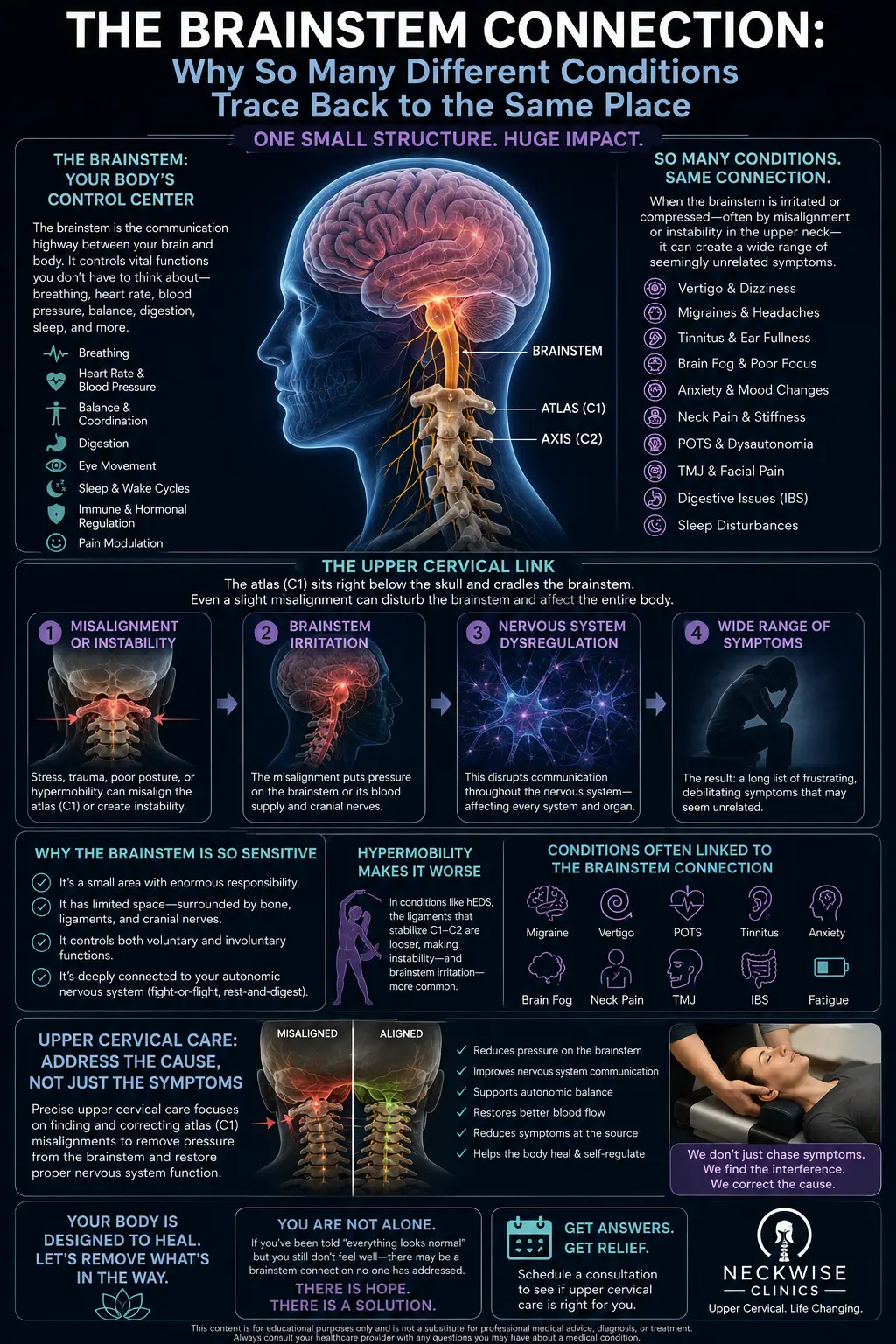
This entire pathway is exquisitely dependent on the health of the brainstem and the structures that surround it. And the brainstem, in turn, is housed at the very top of the spinal column — directly behind and below the atlas (C1) and axis (C2), the two uppermost vertebrae of the neck.
The atlas is a unique ring-shaped bone that cradles the base of the skull. The axis sits just below it, with the odontoid process projecting upward into the atlas to form the pivot joint that allows you to rotate your head. Together, C1 and C2 surround and protect the brainstem and the lower cranial nerves, including the vagus, spinal accessory, hypoglossal, and — by direct anatomical proximity — the nuclei from which the facial nerve originates.
When the atlas or axis becomes misaligned — even by fractions of a millimeter — several things can happen at the upper cervical level that affect facial nerve function. First, the misalignment can create asymmetric tension on the dural sheath, the tough membrane that wraps the brainstem and spinal cord. This tension can propagate upward into the brainstem itself, subtly altering the neurological environment in which cranial nerve nuclei operate.
Second, upper cervical misalignment can disrupt venous and lymphatic drainage from the head — including the drainage pathways that surround the facial nerve as it courses through the temporal bone. Reduced drainage means slower clearance of inflammatory byproducts, which could prolong the swelling that compresses the facial nerve in the first place.
Third — and this is the connection most often missed by conventional providers — the trigeminocervical nucleus, which sits at the upper cervical level, integrates input from the trigeminal nerve (cranial nerve V), the facial nerve (cranial nerve VII), and the upper cervical spinal nerves. This shared neural hub explains why patients with Bell’s palsy so often have concurrent neck pain, facial pain, or headaches.
A 2022 case report and literature review published in the American Journal of Case Reports analyzed thirteen Bell’s palsy cases treated with multimodal chiropractic care and found that 85 percent of these patients also had pain in the face or neck — a striking pattern that points directly at the trigeminocervical pathway as a participant in the disease process.
In other words, the upper cervical spine is not simply “near” the facial nerve in a vague anatomical sense. It is functionally and neurologically intertwined with the very systems that govern facial nerve health.
Why Upper Cervical Care Matters for Bell’s Palsy
At Lavender Family Chiropractic in Sarasota, we use the Knee Chest Upper Cervical technique — a precise, gentle, and research-backed approach to correcting atlas and axis misalignments without any twisting, popping, or forceful manipulation. The patient is positioned face-down on a specially designed knee chest table, the doctor uses a 3D CBCT scan and a thorough neurological evaluation to identify the exact direction and degree of misalignment, and the correction is delivered with sub-millimeter accuracy using a light, controlled thrust.
For Bell’s palsy patients, this matters for several reasons.
When the atlas is misaligned, the brainstem is operating in a less-than-optimal mechanical environment. The dural tension is asymmetric, the venous and lymphatic drainage pathways are partially compromised, and the proprioceptive input from the upper cervical region — which normally helps the brainstem regulate cranial nerve function — is distorted. Correcting the misalignment relieves this mechanical stress, normalizes the neurological environment around the brainstem, and removes one of the contributing factors that may be slowing or preventing full recovery.
For patients in the acute phase, this can mean faster reduction of inflammation and earlier return of facial movement. For patients in the chronic phase — those weeks, months, or years past the original onset — upper cervical correction can help address the residual deficits that have not resolved on their own. These patients often arrive at our office having been told that what they have is “just the new normal.” We do not accept that conclusion at face value, because the literature is full of cases where chronic Bell’s palsy patients have continued to improve once the upper cervical component was addressed.
A 2012 case study published in the Journal of Chiropractic Medicine documented a 47-year-old woman with chronic Bell’s palsy who received chiropractic care including cervical and thoracic adjustments. She reached 90 percent improvement after a year of care, with reductions in facial paralysis, sinus pressure, and intermittent facial tingling — symptoms that had persisted despite standard medical treatment.
A 2019 case study from the Journal of Upper Cervical Chiropractic Research documented an even more dramatic response: a patient whose Bell’s palsy showed 80 to 90 percent improvement in facial mobility after the initial upper cervical adjustment, with complete resolution of facial paralysis two visits later.
These are case reports, not randomized controlled trials. They do not prove that upper cervical care cures Bell’s palsy. But they do establish a credible mechanism and a meaningful clinical pattern — one we have personally observed in patients at our Sarasota office.
What Care Looks Like at Lavender Family Chiropractic
If you come to our office in Sarasota for a Bell’s palsy evaluation, here is what to expect.
Your first visit begins with a thorough consultation. Dr. Lavender or Dr. Temple will sit down with you, listen to your full history, and review every detail of your symptoms — when the paralysis started, what preceded it, what conventional treatment you have received, and what residual issues remain. We want to understand not just the Bell’s palsy but the broader context of your nervous system health.
From there, we conduct a complete upper cervical examination. This includes a 3D CBCT scan to visualize the alignment of your atlas and axis with sub-millimeter precision, neurological testing including cranial nerve assessment, postural and gait analysis, and functional nervous system scans to objectively measure how your nervous system is operating before care begins. This level of diagnostic detail is what separates upper cervical care from general chiropractic — we are not guessing, we are measuring.
If the examination reveals an upper cervical misalignment that is likely contributing to your condition, we will discuss our recommendations openly with you. Care is delivered through the Knee Chest Upper Cervical technique. There is no popping, no twisting, no cracking. The correction itself is so gentle that most patients describe it as anticlimactic — they expect something dramatic and instead feel only a light contact and a quiet shift. The work the body does in response, however, is anything but anticlimactic.
We offer personalized care plans tailored to each patient’s specific needs and goals. Bell’s palsy is not a condition where one or two visits will deliver lasting results — the nervous system needs time, repetition, and the right environment to remodel itself. Our care plans are designed to give your body that environment for as long as it takes to see meaningful, lasting change.
📞 Call (941) 243-3729 to schedule your complimentary consultation 📅 Book your consultation online 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
What the Research Says About Chiropractic Care and Bell’s Palsy
The body of research on chiropractic care and Bell’s palsy is growing, and while it consists primarily of case studies and case series rather than large randomized trials, it paints a coherent and clinically meaningful picture.
The most important recent contribution is the 2022 case report and literature review published in the American Journal of Case Reports, which documented a patient with concurrent Bell’s palsy and trigeminal neuropathy whose face and neck pain and facial paresis resolved within a month of multimodal chiropractic care including upper cervical and upper thoracic spinal manipulation.
The authors then reviewed twelve additional published cases of Bell’s palsy treated with chiropractic spinal manipulation and found that 85 percent of these patients also had pain in the face or neck, strongly suggesting that the trigeminocervical pathway plays a role in both the disease and the recovery response.
The 2012 Journal of Chiropractic Medicine case study, referenced above, documented sustained improvement in a chronic Bell’s palsy patient with 90 percent recovery over the course of a year of chiropractic care — a striking outcome for a patient who had not responded fully to standard medical management.
A comprehensive 2024 review in Cureus (PMC) examined the current state of Bell’s palsy management and explicitly listed chiropractic among the treatment modalities considered alongside corticosteroids, antivirals, acupuncture, and physical therapy — acknowledging that the condition responds to a broader range of interventions than conventional medicine alone has historically embraced.
A 2025 study in The Laryngoscope analyzing US claims data from 2007 to 2022 documented that the annual incidence of Bell’s palsy in US adults has increased significantly — climbing from previous estimates to 24.5 cases per 100,000 adults, with a statistically significant upward trend over the study period. This rising incidence makes effective, accessible treatment options more important than ever.
Finally, a 2025 real-world analysis of 281,600 patients published in PMC confirmed the strong associations between Bell’s palsy and herpes simplex virus, diabetes, depression, and pregnancy — risk factors that all share a common thread of immune system stress and inflammatory burden. Upper cervical care, by improving brainstem function and autonomic regulation, may help reduce the systemic stress load that primes these risk factors in the first place.
None of this research establishes upper cervical chiropractic as a stand-alone “cure” for Bell’s palsy. What it does establish is that there is a credible neurological mechanism, a growing clinical literature, and a meaningful pattern of patient response — particularly in the substantial subset of Bell’s palsy patients who have concurrent neck or facial pain.
Lifestyle Factors That Support Recovery from Bell’s Palsy
Upper cervical chiropractic care is powerful, but recovery from Bell’s palsy is multifactorial. The patients who do best are the ones who combine structural correction with intelligent lifestyle support that helps the nervous system heal.
Stress management. Bell’s palsy is strongly associated with periods of high stress — both physical and emotional. Stress depletes the immune system, increases inflammation, and can trigger reactivation of latent viruses like herpes simplex. Whatever stress management strategies work for you — meditation, breathwork, time outdoors, time away from screens — they belong in your recovery toolkit.
Sleep. The nervous system does most of its repair work during deep sleep. If you are not sleeping seven to nine hours of high-quality sleep per night, you are working against your own recovery. Prioritize a dark room, a cool temperature, and a consistent bedtime.
Nutrition. Anti-inflammatory eating — minimizing processed foods, refined sugars, and seed oils, while emphasizing whole foods, healthy fats, and adequate protein — supports nerve repair. Omega-3 fatty acids and B vitamins, particularly B12, have specific roles in nerve health.
Eye protection. If your blink reflex is impaired, your eye on the affected side is vulnerable to drying, infection, and corneal damage. Use lubricating eye drops liberally, consider an eye patch or moisture chamber at night, and follow your medical doctor’s guidance carefully on this point. Eye protection is non-negotiable during the active phase of Bell’s palsy.
Gentle facial exercises. Once you are past the acute inflammatory phase, gentle facial movement exercises can help retrain the neural pathways and reduce the risk of synkinesis (involuntary co-contraction of facial muscles during voluntary movement). Work with a qualified facial physical therapist if possible.
Hydration. The Florida heat and humidity in Sarasota make chronic low-grade dehydration extremely common. Aim for at least half your body weight in ounces of water daily.
If you found this guide useful, you may also want to read our pillar guide on vertigo and upper cervical care, which explores many of the same brainstem and cranial nerve principles in greater depth.
Serving Sarasota and the Surrounding Communities
Lavender Family Chiropractic is located in Sarasota, Florida, at 5899 Whitfield Avenue, Suite 107 — at the corner of University and Whitfield. From this central location, we serve patients throughout the region, including Bradenton, Lakewood Ranch, Palmetto, Parrish, Venice, Osprey, Nokomis, Ellenton, Ruskin, Myakka City, North Port, and the greater Tampa Bay area. Patients also travel from St. Pete, Ellington, Riverview, and Manatee County to receive specialized upper cervical care here.
Bell’s palsy is the kind of condition where patients are often willing to drive significant distances to find a provider who actually understands the upper cervical component of facial nerve dysfunction. If you are in the region and looking for that level of specialized care, we encourage you to reach out.
Top 15 FAQs About Bell’s Palsy and Upper Cervical Chiropractic Care
1. Is Bell’s palsy a stroke? No. Bell’s palsy is a peripheral facial nerve paralysis, while a stroke causes central facial weakness. The key distinguishing feature is that Bell’s palsy affects the entire side of the face including the forehead, while strokes typically spare the forehead because of how the upper face is innervated from both sides of the brain. That said, any sudden facial weakness should be evaluated by a medical professional immediately to rule out stroke.
2. How long does Bell’s palsy typically last? Most cases resolve significantly within three to six months. About 70 to 80 percent of patients recover fully on their own. However, 20 to 30 percent are left with some degree of permanent deficit — facial asymmetry, synkinesis, residual weakness, or twitching — which is where upper cervical care can be particularly valuable.
3. What causes Bell’s palsy? The conventional view is that reactivation of the herpes simplex virus causes inflammation and swelling of the facial nerve within its bony canal. Diabetes, pregnancy, high blood pressure, obesity, and immune system stress are known risk factors. Trauma to the upper neck — including whiplash and other cervical injuries — may also play a role in some cases.
4. Can chiropractic care help Bell’s palsy? Multiple published case studies and case series suggest that chiropractic care, particularly upper cervical care, can support recovery in both acute and chronic Bell’s palsy. The mechanism likely involves improving brainstem function, normalizing trigeminocervical input, and supporting venous and lymphatic drainage from the head.
5. Is upper cervical chiropractic safe for Bell’s palsy patients? Yes. The Knee Chest Upper Cervical technique used at Lavender Family Chiropractic is exceptionally gentle and precise. There is no twisting, popping, or forceful manipulation. The correction is delivered with sub-millimeter accuracy after detailed imaging and neurological examination.
6. How soon after onset should I seek upper cervical care? There is no wrong time. Some patients come in within the first few days of symptom onset hoping to support the fastest possible recovery. Others come years later seeking help with residual deficits. Both can benefit. The earlier you address the upper cervical component, the more likely you are to support a complete recovery — but it is never too late to start.
7. Will I need to stop my conventional medical treatment to receive upper cervical care? Absolutely not. Upper cervical chiropractic care is complementary to your medical treatment, not a replacement for it. Continue working with your medical doctor, neurologist, and any other specialists on your team. We coordinate with conventional care, we do not replace it.
8. What is the difference between Bell’s palsy and Ramsay Hunt syndrome? Ramsay Hunt syndrome is caused by reactivation of the varicella zoster virus (the chickenpox/shingles virus) affecting the facial nerve, and typically includes painful blisters in or around the ear along with facial paralysis. Bell’s palsy is idiopathic and does not include blisters. Both conditions can benefit from upper cervical care, but Ramsay Hunt requires specific antiviral treatment from your medical doctor.
9. Can stress trigger Bell’s palsy? Stress does not directly cause Bell’s palsy, but it depletes immune function and can trigger viral reactivation, which is a leading suspected mechanism. Many of our patients report a period of unusual stress in the weeks before their symptoms began.
10. Why does Bell’s palsy sometimes come back? Recurrence happens in 4 to 14 percent of patients. This often points to an unresolved underlying contributor — chronic stress, immune dysregulation, a persistent upper cervical misalignment that has never been addressed, or a metabolic risk factor like uncontrolled diabetes. Addressing the upper cervical component can be particularly important for patients with recurrent Bell’s palsy.
11. Can I still exercise during Bell’s palsy? Generally yes, with common-sense modifications. Avoid strenuous straining that increases intracranial pressure, protect your eye on the affected side, and listen to your body. Gentle movement, walking, and low-impact exercise are generally fine and may support recovery.
12. Does Bell’s palsy affect children? Yes, though less commonly than adults. The condition can occur at any age, including in children, with an estimated incidence of 11.5 to 30 per 100,000 in pediatric populations. Upper cervical care is safe and gentle enough to be appropriate for children as well as adults.
13. What about synkinesis and other long-term effects? Synkinesis — the involuntary co-contraction of facial muscles during voluntary movement, such as the eye closing when you smile — is one of the most common long-term complications of incomplete Bell’s palsy recovery. Upper cervical care, combined with targeted facial rehabilitation, may help reduce these residual issues by supporting the underlying neurological environment in which the facial nerve is trying to remodel itself.
14. How will I know if upper cervical care is right for me? The only way to know for certain is to come in for an evaluation. Our examination will identify whether you have an upper cervical misalignment that is likely contributing to your condition. If the answer is no, we will tell you honestly. If the answer is yes, we will explain exactly what we recommend and why.
15. How do I get started? Call our Sarasota office at (941) 243-3729 or book your consultation online. We will sit down with you, review your history, perform a thorough examination, and give you straight answers about whether upper cervical care is a good fit for your situation.
Take the Next Step Toward Recovery
Bell’s palsy is more than a cosmetic issue. It is a neurological condition that affects how you eat, how you speak, how you express yourself, and how you experience your own face in the mirror. Recovery is possible — for most patients, even full recovery — but the patients who do best are the ones who address every layer of the condition rather than waiting passively for it to resolve.
If you are in Sarasota, Bradenton, Lakewood Ranch, or anywhere in the surrounding region and you are dealing with Bell’s palsy — whether it began last week or last year — Dr. Rusty Lavender and Dr. Jacob Temple at Lavender Family Chiropractic are here to help you understand the upper cervical piece of your healing puzzle.
📞 Call (941) 243-3729 today to schedule your complimentary consultation 📅 Book online here 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield