By Dr. Rusty Lavender
Long Covid: You had COVID. Maybe it was mild, maybe it knocked you flat for a couple of weeks. Either way, you expected to recover and move on. But weeks turned into months, and the symptoms did not leave. The crushing fatigue that does not lift with rest. The brain fog that makes simple tasks feel impossible. The racing heart when you stand up. The shortness of breath that does not match any chest X-ray. The dizziness, the headaches, the sleep that no longer restores you, the strange new sensitivities to foods and exertion and stress. You went back to your doctor, and your tests came back normal, and you were told — perhaps kindly, perhaps not — that there was nothing obviously wrong. And yet you know, with absolute certainty, that something is wrong.
At Lavender Family Chiropractic in Sarasota, Florida, we see long COVID patients regularly, and we believe them. Long COVID is real, it is biological, and it is one of the defining chronic illnesses of this decade. Many of the patients we see also carry diagnoses of POTS, dysautonomia, mast cell activation syndrome, or ME/CFS — and many of them have never been evaluated for what the most recent research has identified as a central mechanism in their illness: dysfunction of the vagus nerve and the autonomic control centers in the brainstem, the very structures housed at and protected by the upper cervical spine.
This guide is for anyone in Sarasota, Bradenton, Lakewood Ranch, or the surrounding areas who has been living with long COVID — diagnosed or suspected, mild or severe, recent or longstanding — and who is searching for an angle that addresses the underlying autonomic nervous system dysfunction rather than just chasing individual symptoms. Through the precise, gentle Knee Chest Upper Cervical technique used by Dr. Rusty Lavender and Dr. Jacob Temple, we work to support the autonomic regulation and vagal function that recent research has placed at the center of the long COVID story.
What Is Long COVID?
Long COVID — known clinically as post-acute sequelae of SARS-CoV-2 infection (PASC), post-COVID condition, or post-COVID syndrome — refers to the continuation or development of symptoms that persist or appear after the acute phase of a COVID-19 infection has resolved. The World Health Organization and other bodies generally define it as symptoms that develop during or after a SARS-CoV-2 infection, continue for at least two to three months, and cannot be explained by an alternative diagnosis.
What makes long COVID so difficult to define, diagnose, and treat is the sheer breadth of its presentation. It is not one symptom or even one syndrome — it is a multi-system condition that can affect nearly every part of the body. The most common symptoms include profound fatigue, post-exertional malaise (a worsening of symptoms after physical, cognitive, or emotional exertion), cognitive dysfunction or “brain fog,” shortness of breath, heart palpitations, dizziness and orthostatic intolerance, headaches, sleep disturbances, loss or alteration of taste and smell, gastrointestinal symptoms, joint and muscle pain, and a wide range of neurological and autonomic symptoms. Episodes often fluctuate, with good days and bad days, and many patients describe a pattern of pushing too hard on a good day and then crashing for days afterward — the same post-exertional malaise pattern seen in ME/CFS.
How common is long COVID? The numbers are staggering, even with the wide variation in estimates that comes from different definitions and study methods. A 2025 updated systematic review and meta-analysis estimated a pooled global long COVID prevalence of approximately 34% among studied populations, with estimates ranging widely from 3% to 80% depending on the population and definition used. The RECOVER Initiative, analyzing real-world data from nationwide electronic health record networks, found that 8.5% to 26.4% of adults developed long COVID depending on the classification algorithm used, with an excess incidence of 4% to 7% attributable specifically to SARS-CoV-2 infection. Globally, it has been estimated that more than 65 million people are living with long COVID, with the prevalence continuing to rise as reinfections accumulate.
These are not abstract numbers. In a region the size of Sarasota and its surrounding communities, they translate to thousands of people living with persistent, life-altering symptoms — many of them undiagnosed, many of them disbelieved, and many of them cycling through a medical system that does not yet have a clear treatment pathway for their condition.
What is increasingly clear from the research, however, is that long COVID is not “in your head,” is not simple deconditioning, and is not a psychological condition. It is a biological, multi-system illness with identifiable mechanisms — and one of the most important of those mechanisms involves the autonomic nervous system and the vagus nerve.
The Autonomic and Vagus Nerve Connection: Where the Upper Cervical Spine Comes In
Here is the piece of the long COVID puzzle that has emerged most powerfully in the research over the past few years, and that connects directly to upper cervical care: a substantial portion of long COVID symptoms appear to be driven by dysfunction of the autonomic nervous system — dysautonomia — and by inflammation and impairment of the vagus nerve and the autonomic control centers in the brainstem.
The autonomic nervous system controls everything you do not consciously think about: heart rate, blood pressure, breathing, digestion, temperature regulation, and the balance between the “fight or flight” sympathetic system and the “rest and digest” parasympathetic system. When this system is dysregulated, the result is dysautonomia — and the symptom list of dysautonomia reads almost identically to the symptom list of long COVID: fatigue, brain fog, racing heart, dizziness on standing, temperature dysregulation, gastrointestinal problems, and exercise intolerance.
The research connecting long COVID to autonomic dysfunction is now substantial. A 2024 review in Clinical Microbiology and Infection explicitly examined the role of vagus nerve dysfunction and dysautonomia in long COVID, noting that hypothetical pathophysiological pathways include neurological signalling dysfunction in the brainstem and/or vagus nerve, and that there is considerable overlap between long COVID and ME/CFS in clinical presentation, with dysautonomia as a shared clinical feature that may stem from direct damage to vagal nervous cells. The review highlighted that since SARS-CoV-2 can invade the vagus nerve cells, local vagal inflammation during the acute phase may lead to the long-lasting autonomic dysfunction seen in long COVID.
This is not speculation. A landmark 2023 study published in Acta Neuropathologica by Woo and colleagues provided direct tissue evidence, documenting that SARS-CoV-2 induces vagus nerve inflammation, with increased immune cells in the vagal nuclei of the brainstem, followed by autonomic dysfunction — a mechanism that may contribute to the dysautonomia observed in long COVID. The investigators found the virus’s entry receptors expressed directly on the vagus nerve, and documented a strong inflammatory response in the brainstems of deceased COVID-19 patients.
The brainstem itself appears to be a central site of long COVID pathology. A 2025 commentary in a peer-reviewed journal proposed that neuroinflammation at the dorsolateral inferior medulla — a specific region of the brainstem — is a possible central nervous system localization for both POTS and long COVID, based on the neurological manifestations of both disorders and the emerging neuroimaging evidence. A 2022 review in Autonomic Neuroscience similarly proposed that direct invasion of the hypothalamus or medulla by SARS-CoV-2, affecting the autonomic centers in the brainstem, is one of the primary mechanisms of autonomic dysfunction in long COVID.
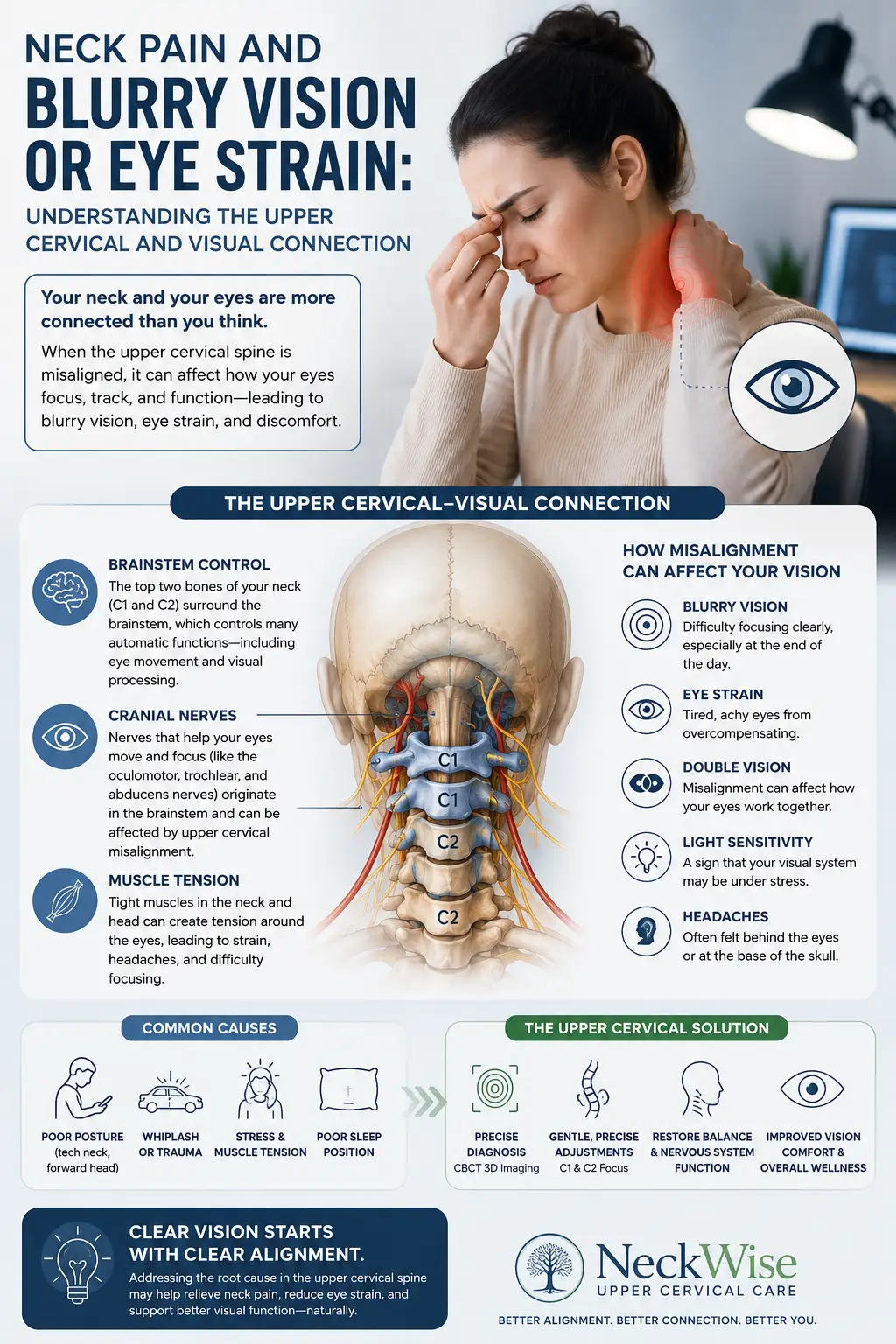
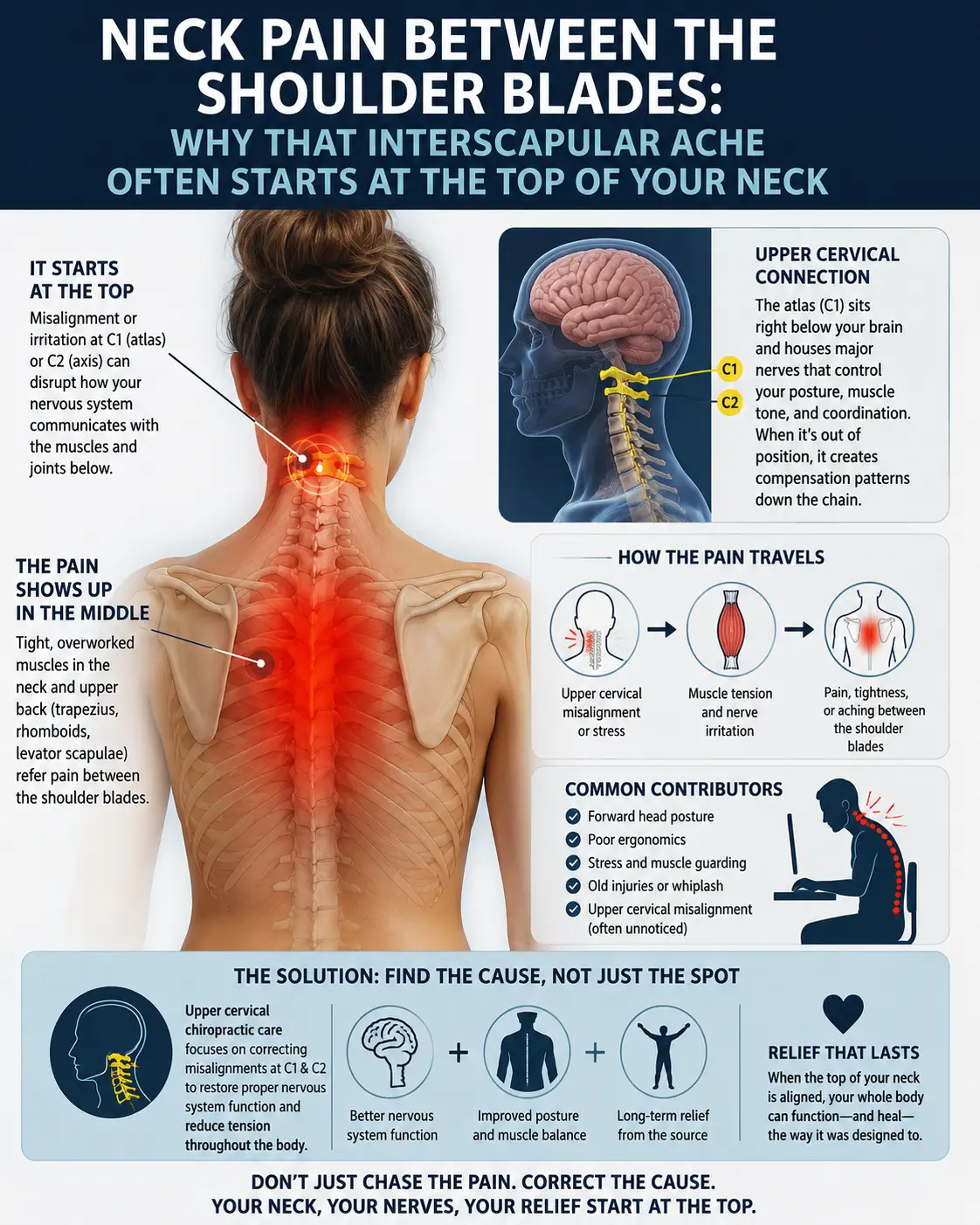
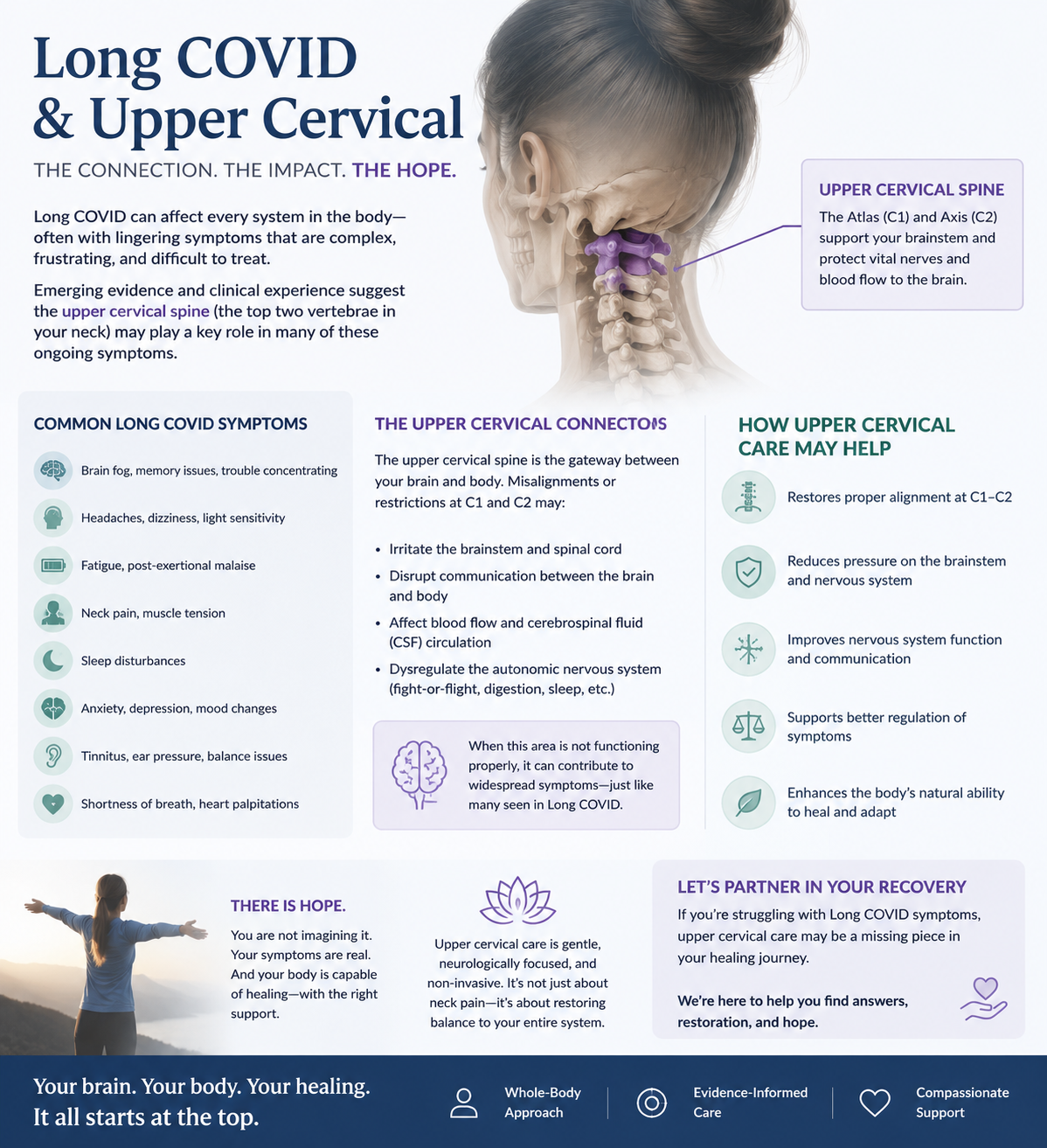
Now connect this to the upper cervical spine. The brainstem — including the medulla, where the vagal nuclei and autonomic control centers reside — sits directly behind and below the atlas (C1) and axis (C2). The vagus nerve exits the skull through the jugular foramen, immediately adjacent to the atlas. The upper cervical spine is the structural housing and protective foundation for exactly the neuroanatomical structures that the long COVID research has implicated. When the upper cervical spine is misaligned, it can affect the mechanical environment around the brainstem, alter venous and lymphatic drainage from the head (impairing clearance of inflammatory byproducts), distort the proprioceptive input the brainstem uses to calibrate autonomic output, and influence vagal tone.
The logic is straightforward. If long COVID symptoms are substantially driven by brainstem neuroinflammation and vagus nerve dysfunction producing autonomic dysregulation, and if the upper cervical spine is the structural foundation that influences the brainstem environment and vagal function, then optimizing upper cervical alignment is one of the few interventions that addresses this upstream mechanism rather than chasing the downstream symptoms one at a time. This is precisely why our service page on vagus nerve dysfunction is so frequently relevant to the long COVID population.
Long COVID, POTS, ME/CFS, and the Autonomic Illness Cluster
One of the most striking features of long COVID is how closely it overlaps with conditions we have long seen in upper cervical practice. Many long COVID patients develop POTS — postural orthostatic tachycardia syndrome — a form of dysautonomia in which the heart rate spikes abnormally upon standing. Many meet the criteria for ME/CFS, the post-viral fatigue syndrome that shares long COVID’s cardinal feature of post-exertional malaise. Many develop mast cell activation symptoms, new food sensitivities, and the constellation of autonomic and immune dysregulation that characterizes the broader cluster of complex chronic illnesses.
This overlap is not coincidental. A 2022 review documented that POTS frequently develops as part of long COVID, with dysautonomia as the underlying mechanism, and noted the substantial overlap between long COVID, POTS, and ME/CFS. All of these conditions share a common thread of autonomic nervous system dysfunction, brainstem and vagal involvement, and post-viral or post-infectious onset. They travel together because they share mechanisms.
For the long COVID patient who has also developed POTS, ME/CFS-like symptoms, or mast cell activation, this matters enormously. It means the upper cervical and autonomic angle is not relevant to just one of their diagnoses — it is potentially relevant to the shared mechanism underlying all of them. Addressing the upper cervical foundation may be a single intervention that supports multiple overlapping conditions simultaneously.
Why Upper Cervical Care Matters for Long COVID Patients
Let us be clear, as we are with every patient we see: upper cervical chiropractic does not cure long COVID. There is no cure for long COVID at this time, and the underlying viral, immune, and inflammatory processes are not something chiropractic care can directly eliminate. What upper cervical care can offer is support for the autonomic regulation and vagal function that the research has placed at the center of long COVID — and for many patients, supporting that upstream mechanism produces meaningful improvement across multiple symptoms at once.
At Lavender Family Chiropractic, we use the Knee Chest Upper Cervical technique — a precise, gentle approach to correcting atlas and axis misalignments without any twisting, popping, or forceful manipulation. For long COVID patients specifically, this gentleness is essential. Long COVID patients are frequently in a hypervigilant, sympathetically dominant autonomic state, often with significant post-exertional malaise, and aggressive manipulation can provoke flares. The Knee Chest technique avoids those forces entirely while still delivering structural correction with sub-millimeter precision.
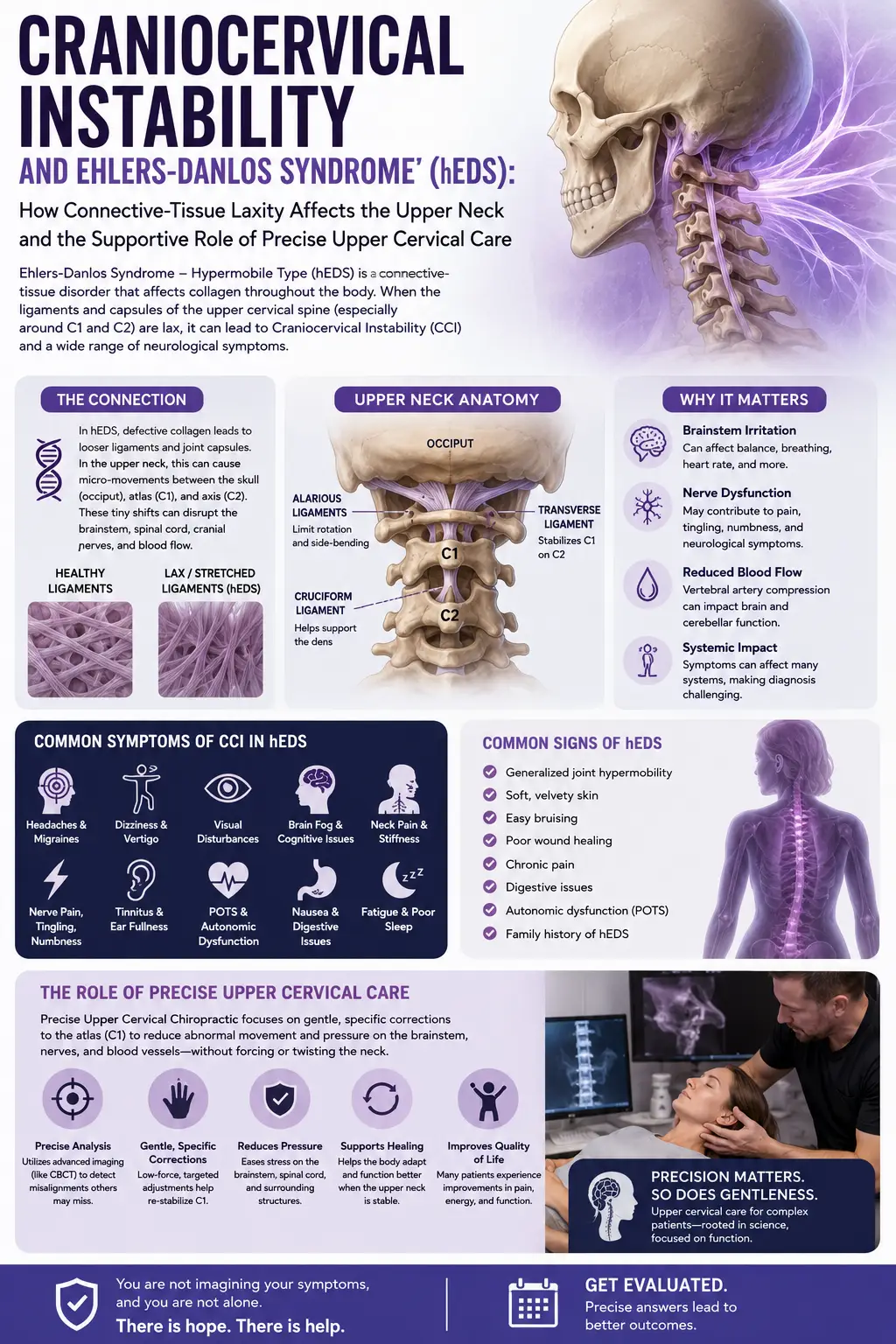
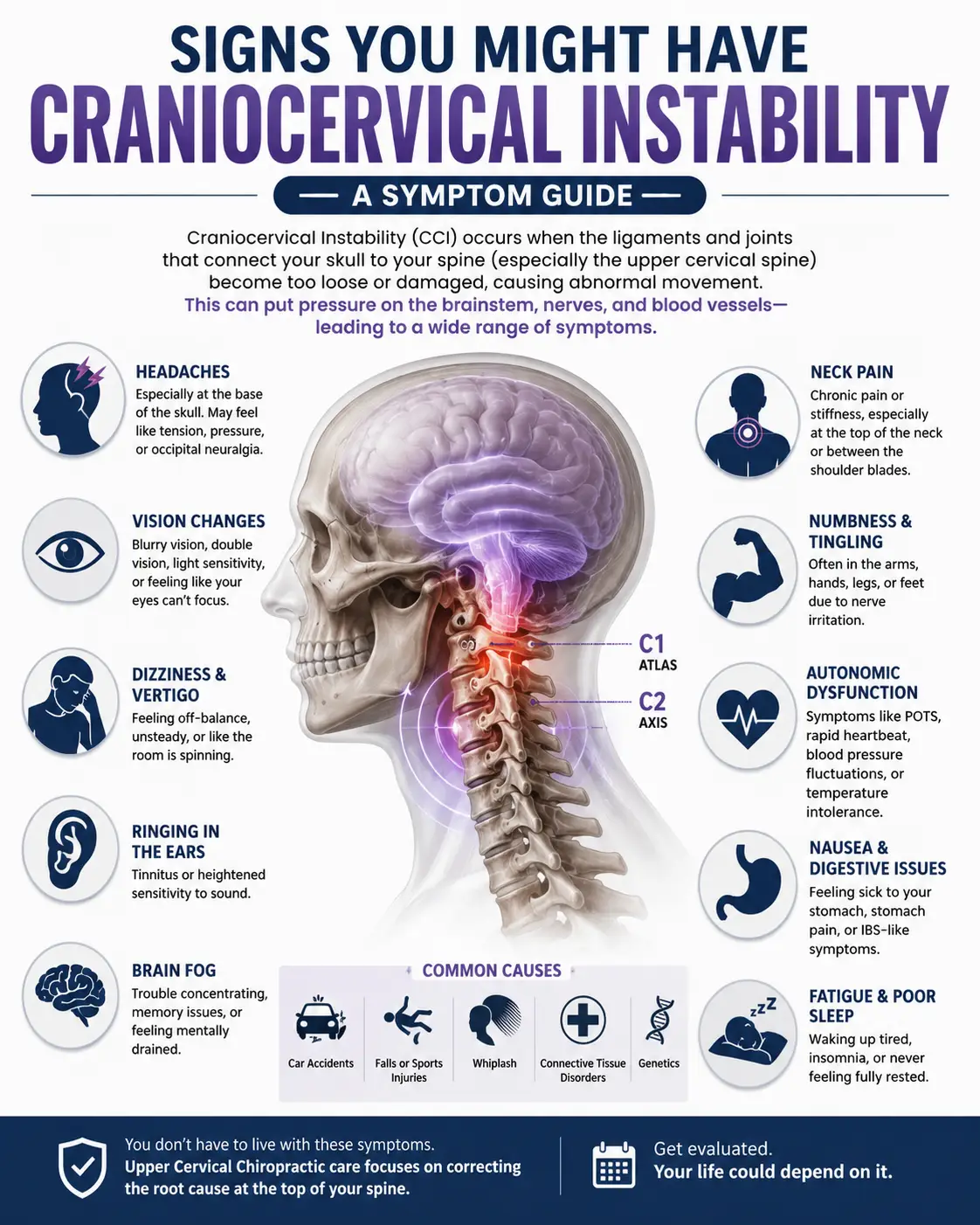
For long COVID patients, upper cervical care can matter in several specific ways. First, by optimizing the alignment of the structures surrounding the brainstem and the vagus nerve’s exit pathway, upper cervical correction supports vagal tone and parasympathetic function — directly addressing the autonomic dysregulation that drives so many long COVID symptoms. Second, improving upper cervical alignment supports venous and lymphatic drainage from the head, which may aid clearance of the inflammatory mediators implicated in brainstem neuroinflammation. Third, restoring proper proprioceptive input from the upper cervical joints helps the brainstem recalibrate the autonomic balance that has been thrown into sympathetic dominance. Fourth, for the substantial subset of long COVID patients with concurrent POTS, ME/CFS, or hypermobility-related craniocervical instability, upper cervical care addresses a shared structural and autonomic contributor.
The honest reality is that long COVID patients vary widely in their response to upper cervical care. Some experience meaningful improvement in fatigue, orthostatic tolerance, brain fog, and sleep within weeks to months. Others experience more gradual or partial improvement. A minority do not respond meaningfully, and we are honest with these patients when we do not see what we hoped to see. What we can promise is a thorough evaluation, a clear explanation of what we find, and an honest assessment of whether upper cervical care is likely to be a meaningful part of your overall recovery strategy.
We pace care very carefully for long COVID patients, exactly as we do for ME/CFS patients. The standard visit frequency for the general patient population is often too much for someone with significant post-exertional malaise, and we adjust accordingly — slower, gentler, more spaced visits often produce better long-term outcomes than aggressive initial loading.
What Care Looks Like at Lavender Family Chiropractic
If you come to our Sarasota office for evaluation related to long COVID, here is what to expect.
Your first visit begins with a thorough consultation. Dr. Lavender or Dr. Temple will sit down with you and review your full history — your acute COVID course, when long COVID symptoms began, your full symptom profile, any comorbid diagnoses (POTS, ME/CFS, MCAS, dysautonomia), your medications and supplements, what other providers have told you, and your post-exertional malaise thresholds. Long COVID patients have often been through extensive and frustrating medical workups, and we want all of that context. We ask carefully about activity tolerance so we can structure care in a way that does not provoke crashes.
The examination is adapted for long COVID patients. We use advanced 3D imaging to visualize your upper cervical alignment with sub-millimeter precision, autonomic function testing to objectively measure your nervous system state, postural and gait analysis, and a careful neurological examination. For patients with concurrent POTS or orthostatic intolerance, we incorporate orthostatic assessment. For patients with severe post-exertional malaise, we may schedule shorter initial visits and break the evaluation into multiple sessions.
If the examination reveals upper cervical findings consistent with someone who is likely to benefit, we will explain our recommendations openly. We will also be honest about what upper cervical care can and cannot do, and we strongly encourage you to continue working with your other providers — long COVID clinics, cardiologists, neurologists, and others — as part of a multidisciplinary approach. We are one part of your care team, never a substitute for it.
Care is delivered through the gentle Knee Chest Upper Cervical technique. We offer customized treatment plans tailored to each patient’s specific situation, recognizing that no two long COVID patients present identically and that pacing is essential.
Because long COVID so frequently involves multi-system, multi-diagnosis complexity, our work with these patients often touches on the territory covered by our complex neurological conditions care — designed precisely for patients whose symptoms cross multiple systems and whose conditions do not fit neatly into a single specialty.
📞 Call (941) 243-3729 to schedule your complimentary consultation 📅 Book your consultation online 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
What the Research Says About Long COVID, Autonomic Dysfunction, and the Vagus Nerve
The research on long COVID has grown explosively, and the autonomic and vagal mechanisms are among the most robustly documented.
The epidemiological foundation is well established. A 2025 updated systematic review and meta-analysis estimated a pooled global long COVID prevalence of approximately 34%, with wide variation across populations and definitions, confirming long COVID as a major global public health challenge. The RECOVER Initiative’s real-world data study documented that 8.5% to 26.4% of adults developed long COVID, with an excess incidence of 4% to 7% directly attributable to SARS-CoV-2 infection, establishing that long COVID is a genuine consequence of infection and not merely background illness.
The mechanistic research on vagus nerve involvement is particularly strong. The 2023 Acta Neuropathologica study by Woo and colleagues provided direct tissue evidence that SARS-CoV-2 induces vagus nerve inflammation, with increased immune cells in the brainstem vagal nuclei, followed by autonomic dysfunction that may contribute to long COVID dysautonomia — one of the most important pieces of mechanistic evidence connecting the virus directly to the autonomic nervous system.
The 2024 Clinical Microbiology and Infection review on vagus nerve dysfunction in long COVID synthesized the evidence and concluded that neurological signalling dysfunction in the brainstem and vagus nerve is among the leading hypothesized mechanisms of long COVID, with substantial overlap between long COVID and ME/CFS in clinical presentation and pathogenesis — placing autonomic and vagal dysfunction at the center of the long COVID story.
The 2025 commentary on brainstem neuroinflammation proposed that neuroinflammation at the dorsolateral inferior medulla is a possible central nervous system localization for both POTS and long COVID, based on the shared neurological manifestations of both disorders — directly implicating the brainstem region housed and protected by the upper cervical spine.
Finally, the 2022 review on long COVID and POTS documented that POTS frequently develops as part of long COVID, with dysautonomia as the underlying mechanism, and substantial overlap among long COVID, POTS, and ME/CFS — establishing the autonomic illness cluster that upper cervical care is positioned to address.
This body of research does not prove that upper cervical chiropractic resolves long COVID. What it does establish is that autonomic dysfunction, vagal impairment, and brainstem neuroinflammation are central, well-documented mechanisms of long COVID — and that the upper cervical spine is the structural foundation that influences exactly those mechanisms.
Lifestyle Factors That Support Long COVID Recovery
Upper cervical chiropractic care is one tool among many. For long COVID patients, the lifestyle scaffolding around care is essential, and the patients who do best tend to be the ones working multiple angles simultaneously and patiently.
Pacing. This is the single most important skill for any long COVID patient with post-exertional malaise. Stay within your “energy envelope” — do less than you think you can on good days to avoid crashing afterward. Heart rate monitoring, step counting, and HRV-based pacing tools can provide objective feedback. Aggressive “push through it” exercise programs frequently make long COVID worse and are no longer recommended.
Vagal tone work. Because vagal dysfunction is central to long COVID, practices that support vagal tone are especially relevant. Slow diaphragmatic breathing with longer exhales than inhales, humming, gargling, gentle cold exposure to the face, and meditation all stimulate vagal pathways. These are gentle, accessible, and can be done at home within your energy limits.
Sleep optimization. Unrefreshing sleep is a hallmark of long COVID, and improving sleep quality often improves the broader symptom picture. Seven to nine hours, dark and cool room, consistent timing. Work with your medical provider on sleep support if needed.
Orthostatic support. For long COVID patients with POTS or orthostatic intolerance, salt and fluid loading, compression garments, and gradual recumbent-to-upright conditioning can provide meaningful relief. Your treating physician can guide this.
Anti-inflammatory eating. Minimizing processed foods, refined sugars, and inflammatory seed oils while emphasizing whole foods, omega-3-rich fish, and adequate protein supports the inflammatory regulation that long COVID disrupts. Patients with mast cell activation may also benefit from a low-histamine approach.
Hydration. Critical for any patient with autonomic dysfunction or orthostatic intolerance. The Florida climate makes it even more important. Aim for at least half your body weight in ounces of water daily, often with added electrolytes.
Stress management. Chronic sympathetic activation worsens nearly every long COVID symptom and further suppresses vagal tone. Gentle, energy-appropriate stress reduction — meditation, time in nature, supportive relationships, restorative practices — supports the parasympathetic recovery your nervous system needs.
Gentle, paced movement. When tolerated, gentle recumbent-friendly movement supports circulation and autonomic function. But it must be carefully paced to avoid triggering post-exertional malaise. Many long COVID patients do better with gradual increases in daily movement than with structured exercise programs.
Medical management. Continue working with your treating physicians and any long COVID clinic involved in your care. Various targeted treatments for the autonomic, immune, and other components of long COVID are emerging. Upper cervical care complements this work — it does not replace it.
If you found this guide useful, you may also want to read about ME/CFS, the post-viral fatigue syndrome that overlaps extensively with long COVID and shares many of the same autonomic and brainstem mechanisms we work with here.
Serving Sarasota and the Surrounding Communities
Lavender Family Chiropractic is located in Sarasota, Florida, at 5899 Whitfield Avenue, Suite 107 — at the corner of University and Whitfield. From this central location, we serve patients throughout the region, including Bradenton, Lakewood Ranch, Palmetto, Parrish, Venice, Osprey, Nokomis, Ellenton, Ruskin, Myakka City, North Port, and the greater Tampa Bay area. Patients also travel from St. Pete, Riverview, and Manatee County to receive specialized upper cervical care here.
Long COVID has affected an enormous number of people in our region, and many of them have been left without a clear treatment path. We recognize that travel itself can be a burden for long COVID patients with significant fatigue, and we work with patients on care schedules that accommodate their energy limitations. If you have been searching for a provider who believes you, understands the autonomic and vagal mechanisms of your illness, and will work within your real-world limits, we encourage you to reach out.
Top 15 FAQs About Long COVID and Upper Cervical Chiropractic Care
1. Can chiropractic care cure long COVID? No. There is no cure for long COVID at this time, and upper cervical care does not eliminate the underlying viral, immune, or inflammatory processes. What it can do is support the autonomic and vagal regulation that research has placed at the center of long COVID — which for many patients produces meaningful improvement across multiple symptoms.
2. Is upper cervical chiropractic safe for long COVID patients? The Knee Chest Upper Cervical technique is exceptionally gentle and avoids the forceful manipulation that can trigger flares in sensitive patients. We pace care thoughtfully, recognizing that post-exertional malaise is real and that long COVID patients often benefit from slow, gentle care.
3. What is the connection between long COVID and the upper cervical spine? Research has identified vagus nerve dysfunction and brainstem neuroinflammation as central mechanisms of long COVID. The brainstem and the vagus nerve’s exit pathway are housed at and protected by the upper cervical spine. Upper cervical alignment influences the mechanical and neurological environment of exactly these structures.
4. What is dysautonomia and why does it matter in long COVID? Dysautonomia is dysfunction of the autonomic nervous system, which controls heart rate, blood pressure, digestion, temperature, and the balance between “fight or flight” and “rest and digest.” Long COVID frequently involves dysautonomia, and its symptom list — fatigue, brain fog, racing heart, dizziness, temperature dysregulation — closely matches the long COVID symptom list.
5. Will an upper cervical adjustment trigger a crash? This is a real concern for long COVID patients with post-exertional malaise, and we take it seriously. The Knee Chest technique is significantly gentler than most chiropractic adjustments and is usually well tolerated. We start slowly, pace carefully, and watch for individual responses.
6. I developed POTS after COVID. Can upper cervical care help? POTS is one of the most common manifestations of long COVID dysautonomia, and the autonomic and brainstem mechanisms involved are directly relevant to upper cervical care. Many POTS patients respond meaningfully to upper cervical correction. We have experience with this patient population.
7. Is long COVID the same as ME/CFS? They overlap substantially — many long COVID patients meet ME/CFS criteria, and both share the cardinal feature of post-exertional malaise. The mechanisms appear to overlap significantly, particularly the autonomic and brainstem involvement. Upper cervical evaluation is potentially relevant for both.
8. Will my long COVID doctor approve of chiropractic care? Many long COVID clinicians are increasingly aware of the autonomic and vagal mechanisms involved and are open to multidisciplinary approaches. We encourage open communication with your medical team and do not ask patients to stop any other treatment.
9. How long does it take to see results? This varies enormously among long COVID patients. Some notice changes in orthostatic tolerance, sleep, or brain fog within weeks. Others experience more gradual improvement over months. We give honest timelines based on your examination findings and what we observe.
10. Why do my COVID tests come back normal if I’m still sick? Long COVID involves dysfunction in nervous system regulation, autonomic balance, and inflammatory signaling that standard tests are not designed to measure. Normal routine labs do not mean nothing is wrong — they mean the standard tests are not capturing what is happening. Long COVID is a real, biological condition.
11. Will I need to stop my medications? No. Continue all medications as prescribed by your treating physicians. Upper cervical care is complementary, not a replacement. If your medical team eventually wants to adjust your regimen based on clinical improvement, that is a discussion for you and them.
12. Can stress make long COVID worse? Yes, significantly. Stress activates the sympathetic nervous system and further suppresses vagal tone, which is already impaired in long COVID. Managing stress and supporting parasympathetic recovery is an important part of overall management.
13. Is the vagus nerve really involved in long COVID? The evidence is strong. A 2023 study in Acta Neuropathologica found direct tissue evidence of SARS-CoV-2-induced vagus nerve inflammation and brainstem involvement, and multiple reviews have placed vagal dysfunction at the center of long COVID dysautonomia. The vagus nerve’s anatomical relationship to the upper cervical spine is what makes this mechanism relevant to our care.
14. How will I know if upper cervical care is right for me? The only way to know definitively is a thorough evaluation. We will assess whether your upper cervical and autonomic findings are consistent with someone likely to benefit. If they are not, or if your situation calls for a different kind of help, we will tell you honestly.
15. How do I get started? Call our Sarasota office at (941) 243-3729 or book your consultation online. We will review your full history, perform a thorough examination, and give you a straight answer about whether upper cervical care is a good fit for your specific situation.
Take the Next Step Toward Recovery
Long COVID is one of the defining chronic illnesses of this era — real, biological, multi-system, and still poorly served by a medical system that is racing to catch up. The patients who do best are the ones who build a broad multidisciplinary team, address the condition from multiple angles, and refuse to accept disbelief as an answer. The autonomic nervous system and the vagus nerve sit at the center of the long COVID story, and the upper cervical spine is the structural foundation that influences both. For the substantial subset of long COVID patients whose illness is being driven, in meaningful part, by autonomic and vagal dysfunction, addressing the upper cervical contributor can be an important piece of recovery.
If you are in Sarasota, Bradenton, Lakewood Ranch, or anywhere in the surrounding region and you are living with long COVID, Dr. Rusty Lavender and Dr. Jacob Temple at Lavender Family Chiropractic are here to help you understand whether the upper cervical, autonomic, and vagal piece is the missing part of your recovery. It will not cure the condition. It may be one of the most important pieces nobody has yet offered you.
📞 Call (941) 243-3729 today to schedule your complimentary consultation 📅 Book online here 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield