By Dr. Rusty Lavender and Dr. Jacob Temple
Occipital Neuralgia Treatment in Sarasota: It often begins at the base of the skull — a sharp, stabbing, electric jolt that shoots up the back of the head, sometimes all the way to the scalp behind the ear or even behind the eye. Between the jolts, there may be a deep aching or burning. The scalp can become so tender that brushing your hair, lying on a pillow, or even a light touch is painful. The pain is frequently on one side, and it can be triggered by simple neck movements. Many people describe it as feeling like an electric shock, an ice pick, or a hot wire running up the back of the head.
For many patients, this distinctive pattern is occipital neuralgia — and it is one of the most commonly misdiagnosed headache conditions there is. Because the pain radiates up into the head, it is frequently mistaken for migraine, tension headache, or “just a bad headache,” and patients are treated with migraine medications that do not address the actual source. The real problem, in most cases, lies in the occipital nerves — and specifically in the upper cervical spine, where these nerves originate.
At Lavender Family Chiropractic in Sarasota, Florida, occipital neuralgia is one of the conditions where the upper cervical connection is most direct and most clear. The greater occipital nerve, which is responsible for the large majority of occipital neuralgia cases, arises directly from the C2 nerve root and passes through the upper cervical region on its way to the scalp. This means the alignment and function of the upper cervical spine — the atlas (C1) and axis (C2) — is intimately tied to the very nerve that generates the pain. This guide is for anyone in Sarasota, Bradenton, Lakewood Ranch, or the surrounding areas who has been dealing with this distinctive head pain and wants to understand what occipital neuralgia really is, why the upper neck is so central to it, and how the precise, gentle Knee Chest Upper Cervical technique used by Dr. Rusty Lavender and Dr. Jacob Temple fits into care.
What Is Occipital Neuralgia?
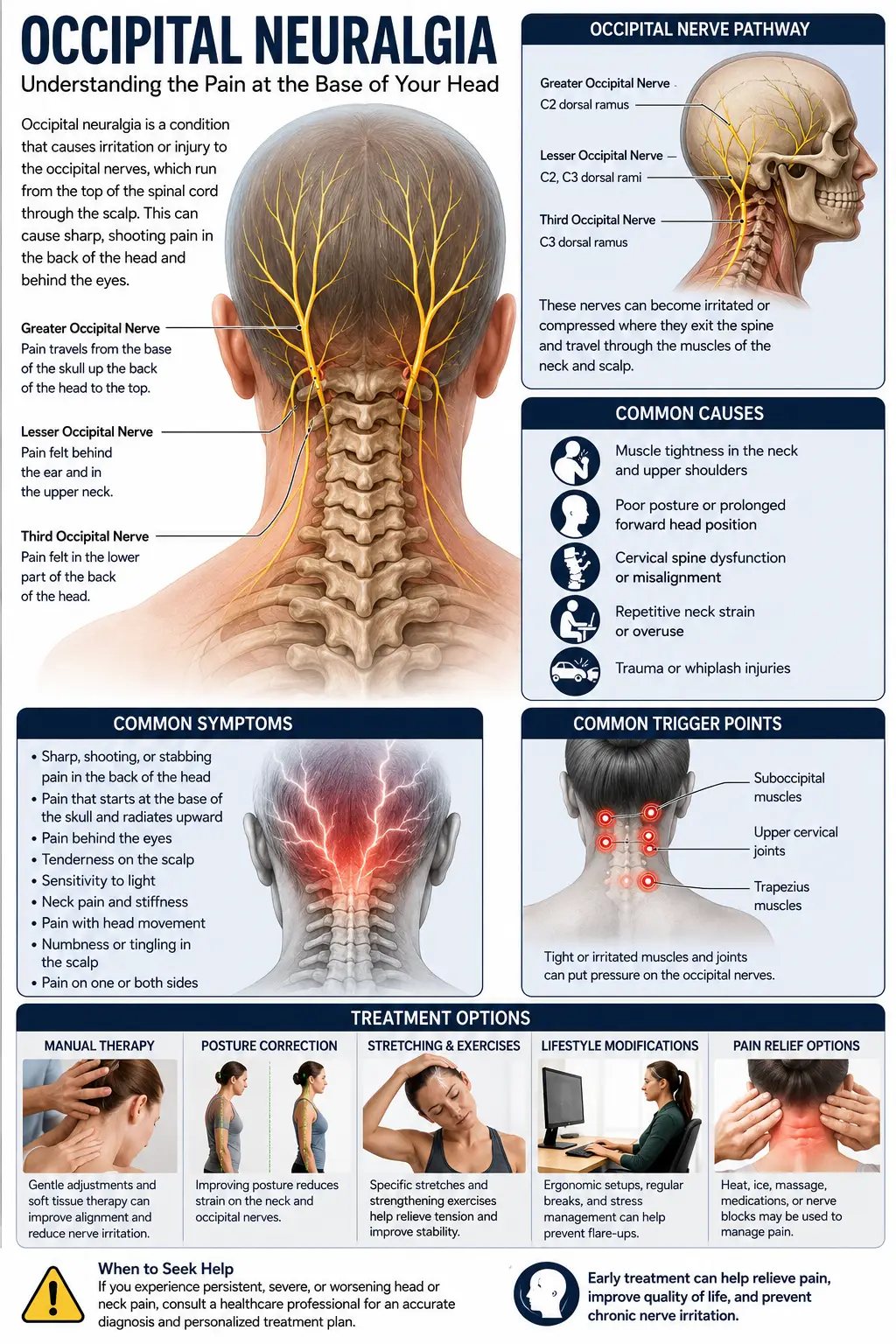
Occipital neuralgia is a distinct headache condition caused by injury, irritation, compression, or inflammation of the occipital nerves — the nerves that supply sensation to the back of the head and scalp. It is sometimes called C2 neuralgia or Arnold’s neuralgia, and it is classified as a form of cervicogenic (neck-origin) head pain.
There are three occipital nerves involved. The greater occipital nerve, which arises primarily from the dorsal ramus of the C2 spinal nerve, supplies the majority of the back of the scalp and is responsible for the large majority of occipital neuralgia cases. The lesser occipital nerve, arising from the C2 and C3 region, supplies the area behind the ear. The third (least) occipital nerve, from the C3 region, supplies a smaller area at the base of the skull. According to clinical references, approximately 90% of occipital neuralgia patients have greater occipital nerve involvement.
The hallmark of occipital neuralgia is its distinctive pain pattern. The International Headache Society defines it as paroxysmal — meaning it comes in sudden attacks — jabbing pain in the distribution of the occipital nerves, accompanied by diminished sensation or abnormal sensation in the affected area, and often tenderness over the affected nerve. The pain is typically described as sharp, stabbing, shooting, or electric-shock-like, lasting from seconds to minutes, often superimposed on a more constant aching or burning. It usually begins at the base of the skull and radiates upward over the back and side of the head, frequently on one side. Patients commonly report scalp tenderness (sometimes so severe that combing the hair or resting on a pillow is painful), sensitivity to light, and in some cases pain referred behind the eye.
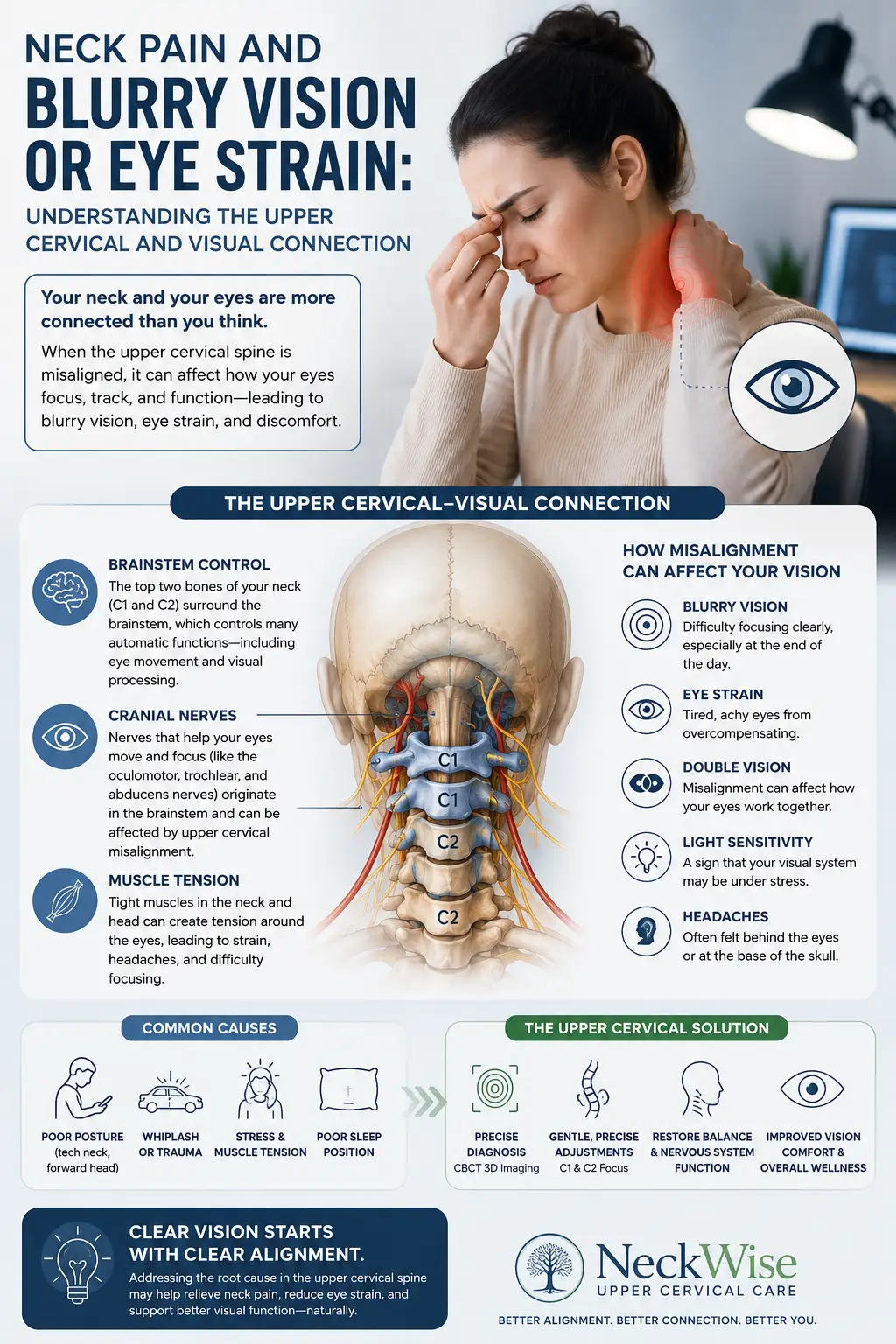
That last feature — pain behind the eye — points to one of the most fascinating and clinically important aspects of occipital neuralgia: its connection to the trigeminocervical complex. The sensory fibers of the upper cervical nerves (C2 in particular) converge in the brainstem and upper spinal cord with the trigeminal nerve fibers that supply the face. This convergence, in a region called the trigeminocervical complex at the C2 dorsal horn, means that pain originating in the occipital nerves can be referred forward to the front of the head and behind the eye, and explains why occipital neuralgia and conditions like migraine and trigeminal pain can overlap and feed one another. This is the same neuroanatomical crossroads that underlies the relationship between the upper neck and many headache conditions.
How common is occipital neuralgia? The true prevalence is genuinely uncertain, because the condition is frequently misdiagnosed and underrecognized. One study of facial pain in the Netherlands found an incidence of occipital neuralgia of 3.2 per 100,000 people per year, with a mildly higher incidence in females, though many experts believe the real figure is higher because so many cases are misattributed to migraine or tension headache. What is clear is that occipital neuralgia is a real, distinct, and treatable condition that affects a meaningful number of people — and that getting the diagnosis right is the first step toward relief.
The Upper Cervical Connection: Why the C2 Region Is the Source
This is where occipital neuralgia stands apart from many of the other conditions where the upper cervical connection requires careful explanation. Here, the connection is direct, anatomical, and central to the condition itself.
The greater occipital nerve is formed from fibers of the dorsal ramus of the C2 spinal nerve. After arising from C2, it travels between the C1 (atlas) and C2 (axis) vertebrae, courses through the suboccipital muscles — passing between the inferior oblique and semispinalis capitis muscles — pierces the semispinalis and trapezius, and then becomes superficial to supply the skin of the posterior scalp. There is also an important anatomical vulnerability here: the C2 ganglion emerges between the atlas and axis and is not protected by bone the way other spinal ganglia are, which makes it more susceptible to compression and irritation than nerves elsewhere in the spine.
This anatomy is the entire story of why the upper cervical spine matters so directly in occipital neuralgia. The nerve that generates the pain originates at C2 and passes through the C1-C2 region. When the upper cervical spine is misaligned, several things can happen that irritate this nerve. Misalignment of the atlas and axis can alter the mechanical relationship between the bones and the C2 nerve and ganglion. The suboccipital muscles through which the nerve passes can become tight and spastic, entrapping the nerve along its course — a mechanism known as muscular entrapment that is one of the recognized causes of occipital neuralgia. And the chronic irritation feeds the trigeminocervical complex, contributing to the referred pain and central sensitization that make the condition so persistent.
The recognized causes of occipital neuralgia map directly onto this upper cervical picture. The medical literature identifies the causes as including trauma (such as whiplash), muscular entrapment along the nerve’s path from C2 to the trapezius, degenerative cervical spine disease, irritation of the C1-C2 region, inflammation, and, in rare cases, vascular anomalies, tumors, or other structural lesions. Most cases, however, are considered idiopathic or related to cervical and muscular factors — exactly the territory that upper cervical alignment influences.
Occipital neuralgia is also formally classified as a subset of cervicogenic headache — head pain that originates in the neck. This classification matters because it places the condition squarely in the domain where upper cervical care is most relevant. When the upper cervical spine is the source or a major contributor, addressing the spine addresses the actual generator of the pain rather than chasing the downstream symptom with medication.
We can be more confident here than with conditions like sciatica or carpal tunnel, where the upper cervical role requires careful qualification. With occipital neuralgia, the nerve that generates the pain originates in the upper cervical spine. That does not mean upper cervical care resolves every case — some occipital neuralgia is caused by structural lesions, vascular problems, or other factors that require different treatment, and we screen carefully for those. But for the substantial majority of cases that involve cervical and muscular factors, the upper cervical spine is not a distant influence; it is the home of the problem.
Why Upper Cervical Care Matters for Occipital Neuralgia
At Lavender Family Chiropractic, we use the Knee Chest Upper Cervical technique — a precise, gentle method of correcting atlas and axis misalignments without any twisting, popping, or forceful manipulation. For occipital neuralgia, this gentleness is especially valuable, because the region being treated is the very region where the painful nerve lives, and forceful manipulation of an already-irritated area can aggravate symptoms.
For occipital neuralgia patients, upper cervical care can matter in several direct ways. First, by correcting atlas and axis misalignment, we address the mechanical relationship between the C1-C2 vertebrae and the C2 nerve and ganglion from which the greater occipital nerve arises. When the structural relationship is improved, the chronic irritation of the nerve can decrease. Second, restoring proper upper cervical alignment helps relieve the chronic tension and spasm in the suboccipital muscles through which the occipital nerve passes — addressing the muscular entrapment that is a recognized cause of the condition. Third, by reducing the chronic afferent input from the irritated occipital nerve, upper cervical correction can help calm the trigeminocervical complex sensitization that drives the referred pain and the persistence of the condition.
This is also why occipital neuralgia connects so closely to the other head-pain conditions we address. Because of the trigeminocervical convergence, occipital neuralgia frequently overlaps with migraines and shares neuroanatomical territory with conditions like trigeminal neuralgia. For patients whose head pain is a mix of occipital and other components, addressing the upper cervical foundation can influence the shared mechanism underlying several of them.
It is worth understanding how occipital neuralgia is conventionally treated, because it helps clarify where upper cervical care fits. Conventional management is typically stepwise: it begins with conservative measures including posture correction and anti-inflammatory approaches, then progresses to medications (anticonvulsants like carbamazepine or gabapentin, muscle relaxers), and then to occipital nerve blocks — injections of anesthetic and steroid around the nerve that serve both to confirm the diagnosis and to provide relief. According to clinical references, occipital nerve blocks target the sensory fibers of the C2 distribution to interrupt pain transmission, often resulting in rapid relief, and the diagnostic value of these blocks confirms that the C2 region is indeed the source. Upper cervical care addresses that same C2 region — the source the nerve blocks confirm — but does so by correcting the underlying structural and muscular factors rather than temporarily numbing the nerve.
We are honest about candidacy. For occipital neuralgia caused by structural lesions, tumors, vascular anomalies, or other secondary causes, upper cervical care is not the answer, and we screen for these and refer appropriately. For the common forms of occipital neuralgia related to upper cervical and muscular factors, upper cervical care addresses the source directly. The thorough evaluation determines which applies to you.
What Care Looks Like at Lavender Family Chiropractic
If you come to our Sarasota office for evaluation related to occipital neuralgia, here is what to expect.
Your first visit begins with a thorough consultation. Dr. Lavender or Dr. Temple will sit down with you and carefully review your history — the exact character and location of your pain, whether it is one-sided, what triggers it, whether you have scalp tenderness or referred pain behind the eye, any history of head or neck trauma, and what treatments you have tried. Because occipital neuralgia is so often confused with migraine and other headaches, we pay close attention to the distinctive features that distinguish it — the sharp, electric, occipital-origin pain in the distribution of the occipital nerves.
The examination includes a detailed neurological evaluation, palpation of the occipital nerves and suboccipital region (tenderness over the greater occipital nerve is a classic finding), assessment of cervical range of motion and posture, and advanced 3D imaging to evaluate your upper cervical alignment with precision. We screen carefully for red flags and secondary causes — if your presentation suggests a structural lesion, vascular problem, or other condition requiring medical workup, we will tell you directly and help you get the appropriate evaluation and imaging.
If the examination reveals an upper cervical and muscular component driving your occipital neuralgia, we will explain how upper cervical care addresses the C2 region where the pain originates. We coordinate with other providers — neurologists, pain specialists, and others — particularly for patients who may benefit from nerve blocks or medication as part of a comprehensive approach.
Care is delivered through the gentle Knee Chest Upper Cervical technique. We offer customized treatment plans tailored to your specific situation, with transparent timelines and honest expectations.
📞 Call (941) 243-3729 to schedule your complimentary consultation 📅 Book your consultation online 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
What the Research Says About Occipital Neuralgia and the C2 Connection
The research on occipital neuralgia consistently confirms its origin in the upper cervical nerves and the C2 region.
The anatomical foundation is well established. According to a PMC anatomical study, the greater occipital nerve is composed of fibers from the dorsal ramus of the C2 spinal nerve, travels between the C1 and C2 vertebrae, and passes between the suboccipital muscles before supplying the posterior scalp, where its close relationship with these muscles makes it susceptible to compression. This is the direct anatomical basis for the upper cervical connection.
The clinical characterization confirms the C2-C3 origin. According to clinical references, occipital neuralgia is caused by irritation or compression of the cervical spinal nerves in the C2 and C3 region, with approximately 90% of patients having greater occipital nerve involvement, and the condition documented at an incidence of 3.2 per 100,000 — establishing both the upper cervical origin and the predominance of the greater occipital nerve.
The vulnerability of the C2 ganglion is specifically documented. According to a review, the C2 ganglion emerges posteriorly between the atlas and axis vertebrae and is not protected by bone, rendering it more susceptible to compression than other ganglia — a vulnerability that is significant in the pathogenesis of occipital neuralgia, and the same source identifies muscular entrapment along the nerve’s path and cervical degenerative factors among the causes.
The diagnostic and therapeutic role of the C2 region is confirmed by nerve block research. According to StatPearls, the greater occipital nerve block targets the sensory fibers of the C2 distribution to interrupt pain transmission, often resulting in rapid and sustained relief, and serves both diagnostic and therapeutic purposes — confirming that the C2 region is the source that effective treatment targets.
Finally, the trigeminocervical connection is documented in the literature. A PMC case report demonstrated that chronic occipital neuralgia from greater occipital nerve irritation can produce referred facial pain through sensitization of the second-order neurons in the trigeminocervical complex at the C2 dorsal horn, which receives convergent input from both cervical and trigeminal structures — explaining the referred pain behind the eye and the overlap with other headache conditions.
This body of research establishes that occipital neuralgia originates in the upper cervical nerves at the C2-C3 region, that the greater occipital nerve’s anatomy makes it vulnerable to compression and muscular entrapment in the C1-C2 area, and that the C2 region is both the diagnostic and therapeutic target. This is the strongest and most direct anatomical basis for upper cervical care of any condition we treat.
Lifestyle Factors That Support Occipital Neuralgia Recovery
Whether or not upper cervical care is part of your strategy, the daily inputs you control can meaningfully affect occipital neuralgia, particularly the muscular and postural factors.
Posture correction. Forward head posture places chronic strain on the suboccipital muscles through which the occipital nerve passes, contributing to entrapment and irritation. Keeping the head stacked over the shoulders, bringing screens to eye level, and avoiding prolonged forward-head positions reduces this strain.
Suboccipital tension relief. Because the greater occipital nerve passes through the suboccipital muscles, chronic tension in these muscles is a direct contributor. Gentle suboccipital stretches, warmth applied to the base of the skull, and avoiding sustained neck flexion (such as prolonged looking down at phones) can help. A physical therapist can teach targeted release techniques.
Stress management. Stress increases tension in the neck and suboccipital muscles, which can directly aggravate occipital nerve irritation. Stress-reduction practices are genuinely relevant to this condition.
Sleep position and pillow support. Sleeping positions that strain the neck or place pressure on the back of the head can aggravate occipital neuralgia. A supportive pillow that maintains neutral neck alignment, and avoiding positions that compress the tender area, can reduce nighttime aggravation.
Screen and device habits. The sustained downward head tilt of phone and tablet use is a major contributor to suboccipital strain. Raising devices to eye level and taking frequent breaks reduces the cumulative load on the upper neck.
Heat and gentle movement. Many patients find that gentle heat applied to the upper neck and base of the skull, along with gentle range-of-motion movement, helps relax the suboccipital muscles and reduce nerve irritation during a flare.
Anti-inflammatory measures. Because inflammation contributes to nerve irritation, an anti-inflammatory eating pattern and adequate hydration support nerve health. Some patients find this reduces the frequency or intensity of flares.
Avoid aggravating activities. Identify and modify activities that consistently trigger your pain — certain neck positions, heavy overhead work, or sustained postures — to reduce the frequency of attacks.
If you found this guide useful, you may also want to read our blog on forward head posture and tech neck, the postural pattern that places chronic strain on the suboccipital region where the occipital nerve is vulnerable to entrapment.
Serving Sarasota and the Surrounding Communities
Lavender Family Chiropractic is located in Sarasota, Florida, at 5899 Whitfield Avenue, Suite 107 — at the corner of University and Whitfield. From this central location, we serve patients throughout the region, including Bradenton, Lakewood Ranch, Palmetto, Parrish, Venice, Osprey, Nokomis, Ellenton, Ruskin, Myakka City, North Port, and the greater Tampa Bay area. Patients also travel from St. Pete, Riverview, and Manatee County to receive specialized upper cervical care here.
Occipital neuralgia is one of the most commonly misdiagnosed head-pain conditions, and many patients have spent months or years being treated for migraine when the real source is the occipital nerves at the top of the neck. If you recognize the distinctive pattern of occipital neuralgia in your own symptoms, we encourage you to reach out for an evaluation that considers the upper cervical source.
Top 15 FAQs About Occipital Neuralgia and Upper Cervical Chiropractic Care
1. What is occipital neuralgia? Occipital neuralgia is a distinct headache condition caused by irritation, compression, or inflammation of the occipital nerves, which supply the back of the head. It produces sharp, stabbing, electric-shock-like pain that typically begins at the base of the skull and radiates up the back and side of the head, often on one side, frequently with scalp tenderness.
2. How is it different from a migraine? Occipital neuralgia produces sharp, jabbing, electric pain in the distribution of the occipital nerves at the back of the head, often with scalp tenderness, while migraine is typically a throbbing pain often accompanied by nausea, light sensitivity, and sometimes aura. They are frequently confused, and they can overlap through the trigeminocervical complex — which is one reason accurate diagnosis matters.
3. Why is occipital neuralgia connected to my neck? Because the greater occipital nerve, responsible for about 90% of cases, arises directly from the C2 nerve root in the upper cervical spine and passes between the C1 and C2 vertebrae. The nerve that generates the pain originates in your upper neck — this is one of the most direct neck-to-head-pain connections in all of medicine.
4. Can upper cervical chiropractic help occipital neuralgia? For the common forms related to upper cervical and muscular factors, yes — this is one of the conditions where the upper cervical connection is most direct, because the painful nerve originates at C2. Upper cervical care addresses the mechanical and muscular factors irritating the nerve at its source. For occipital neuralgia caused by structural lesions or other secondary causes, different treatment is needed, and we screen for those.
5. Why is the back of my scalp so tender? The tenderness occurs because the irritated occipital nerve makes the scalp it supplies hypersensitive. Tenderness over the greater occipital nerve at the base of the skull is a classic diagnostic finding in occipital neuralgia, and severe cases can make combing the hair or resting on a pillow painful.
6. Why do I sometimes feel pain behind my eye? This is referred pain through the trigeminocervical complex — a region in the upper spinal cord where the C2 sensory fibers converge with the trigeminal nerve fibers that supply the face. Chronic occipital nerve irritation can be referred forward to behind the eye through this convergence.
7. Is upper cervical care safe for occipital neuralgia? The Knee Chest Upper Cervical technique is exceptionally gentle, with no twisting or forceful manipulation. This gentleness is particularly valuable for occipital neuralgia because the region being treated is where the irritated nerve lives, and gentle care avoids aggravating an already-sensitive area.
8. What causes occipital neuralgia? Recognized causes include trauma (such as whiplash), muscular entrapment of the nerve in the suboccipital region, degenerative cervical spine disease, irritation of the C1-C2 region, and inflammation. Rare causes include vascular anomalies, tumors, and other structural lesions. Most cases relate to cervical and muscular factors.
9. How is occipital neuralgia diagnosed? Diagnosis is based on the characteristic pain pattern, tenderness over the occipital nerves, and exclusion of other causes. An occipital nerve block — injecting anesthetic around the nerve — is often used to confirm the diagnosis: if it relieves the pain, it confirms the occipital nerve as the source.
10. What is an occipital nerve block? It is an injection of anesthetic and usually a steroid around the occipital nerve, used both to confirm the diagnosis and to provide relief. It targets the C2 distribution — the same region upper cervical care addresses. Nerve blocks provide temporary relief; upper cervical care aims to address the underlying structural and muscular factors.
11. Can a car accident cause occipital neuralgia? Yes. Whiplash and other head or neck trauma are recognized causes of occipital neuralgia, because they can injure the upper cervical region and the occipital nerves. Our car accident chiropractic care addresses the upper cervical injuries that can lead to post-traumatic occipital neuralgia.
12. Will I need medication or surgery? Many patients are managed without surgery. Conventional care is stepwise — conservative measures, then medications, then nerve blocks, with surgery (such as nerve decompression or stimulation) reserved for refractory cases. Upper cervical care can be part of the conservative approach that addresses the underlying source.
13. How long does it take to see results? This varies by patient and by how much of the condition is driven by upper cervical and muscular factors. Some patients notice meaningful improvement within weeks. We provide honest timelines based on your specific findings.
14. How will I know if upper cervical care is right for me? The only way to know is a thorough evaluation. We will determine whether your occipital neuralgia has an upper cervical and muscular component, screen for secondary causes, and give you an honest assessment of whether upper cervical care is likely to help.
15. How do I get started? Call our Sarasota office at (941) 243-3729 or book your consultation online. We will review your history, perform a thorough examination, screen for red flags, and give you a straight answer about how upper cervical care fits into your recovery.
Take the Next Step Toward Relief
Occipital neuralgia is one of the most distinctive and most treatable head-pain conditions there is — and one of the most frequently misdiagnosed. The sharp, electric pain that shoots up the back of the head originates in the occipital nerves, and specifically in the C2 region of the upper cervical spine. This makes it one of the conditions where the upper cervical connection is not a distant influence but the actual home of the problem. For the many patients whose occipital neuralgia is driven by upper cervical and muscular factors, addressing that source can make a meaningful difference.
If you are in Sarasota, Bradenton, Lakewood Ranch, or anywhere in the surrounding region and you are dealing with the distinctive pain of occipital neuralgia — or you have been treated for migraine without relief and suspect your pain is coming from the back of your head — Dr. Rusty Lavender and Dr. Jacob Temple at Lavender Family Chiropractic are here to give you an honest evaluation of whether the upper cervical source is part of your picture.
📞 Call (941) 243-3729 today to schedule your complimentary consultation 📅 Book online here 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield