By Dr. Rusty Lavender
New Daily Persistent Headache (NDPH): You remember the exact day it started. Not approximately — exactly. For most people, headaches build gradually, come and go, and blur together over time. But for those with new daily persistent headache, the experience is uniquely jarring: one day you did not have a headache, and the next day you did, and it simply never left. It became constant, daily, unremitting — and it has stayed that way ever since, whether for weeks, months, or years. You can point to the date on a calendar. And, in many cases, you have cycled through medication after medication, specialist after specialist, with little or no relief, while the headache continues, day after day, without a break.
New daily persistent headache (NDPH) is one of the most challenging and least understood headache disorders in all of neurology. It is rare, it is frequently misdiagnosed, and it is notoriously resistant to treatment. We want to be honest with you from the very beginning of this guide, because honesty matters most with a condition this difficult: there is no known cure for NDPH, its underlying mechanism is poorly understood, and no single treatment works reliably for everyone. Any provider who promises to cure your NDPH is overpromising on a condition that the medical literature itself describes as “enigmatic.”
What we can offer at Lavender Family Chiropractic in Sarasota, Florida, is something more modest but genuinely worthwhile: a careful evaluation of whether a cervical or upper cervical component is contributing to your headache, and gentle care aimed at that component when it is present. The research on NDPH explicitly identifies cervicogenic factors — problems originating in the neck — as one of the possible contributors to this disorder. For the subset of NDPH patients in whom the upper cervical spine is part of the picture, addressing it may be a meaningful piece of a broader, multidisciplinary approach. This guide is for anyone in Sarasota, Bradenton, Lakewood Ranch, or the surrounding areas who is living with this difficult condition and wants to understand it clearly and honestly — including where upper cervical care fits, and where it does not.
What Is New Daily Persistent Headache?
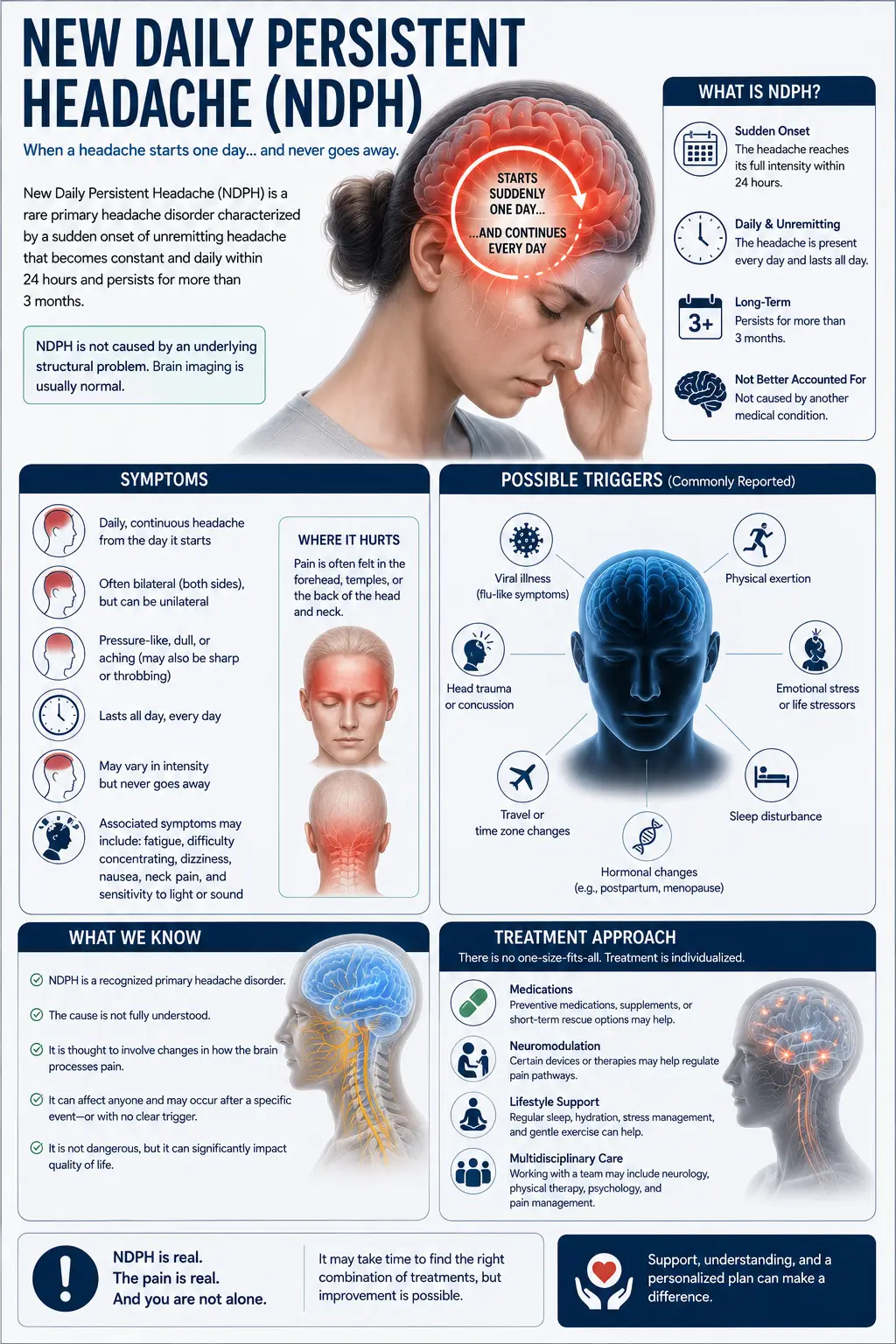
New daily persistent headache is a primary headache disorder defined by a very specific and unusual feature: it is daily and unremitting from the moment it begins. According to the International Classification of Headache Disorders (ICHD-3), NDPH is characterized by a headache that is daily from onset, becomes continuous and unremitting within 24 hours, persists for more than three months, and occurs in individuals who can clearly and accurately recall the distinct moment it started — often in someone with no significant prior headache history.
That last feature is what sets NDPH apart from nearly every other headache disorder. Most chronic headaches evolve gradually: episodic migraines that become more frequent, tension headaches that creep up over years. NDPH does not do this. It arrives suddenly, becomes constant almost immediately, and the patient can pinpoint the exact date. As one set of diagnostic criteria notes, patients with this disorder invariably recall and can accurately describe the onset; if they cannot do so, another diagnosis should be considered.
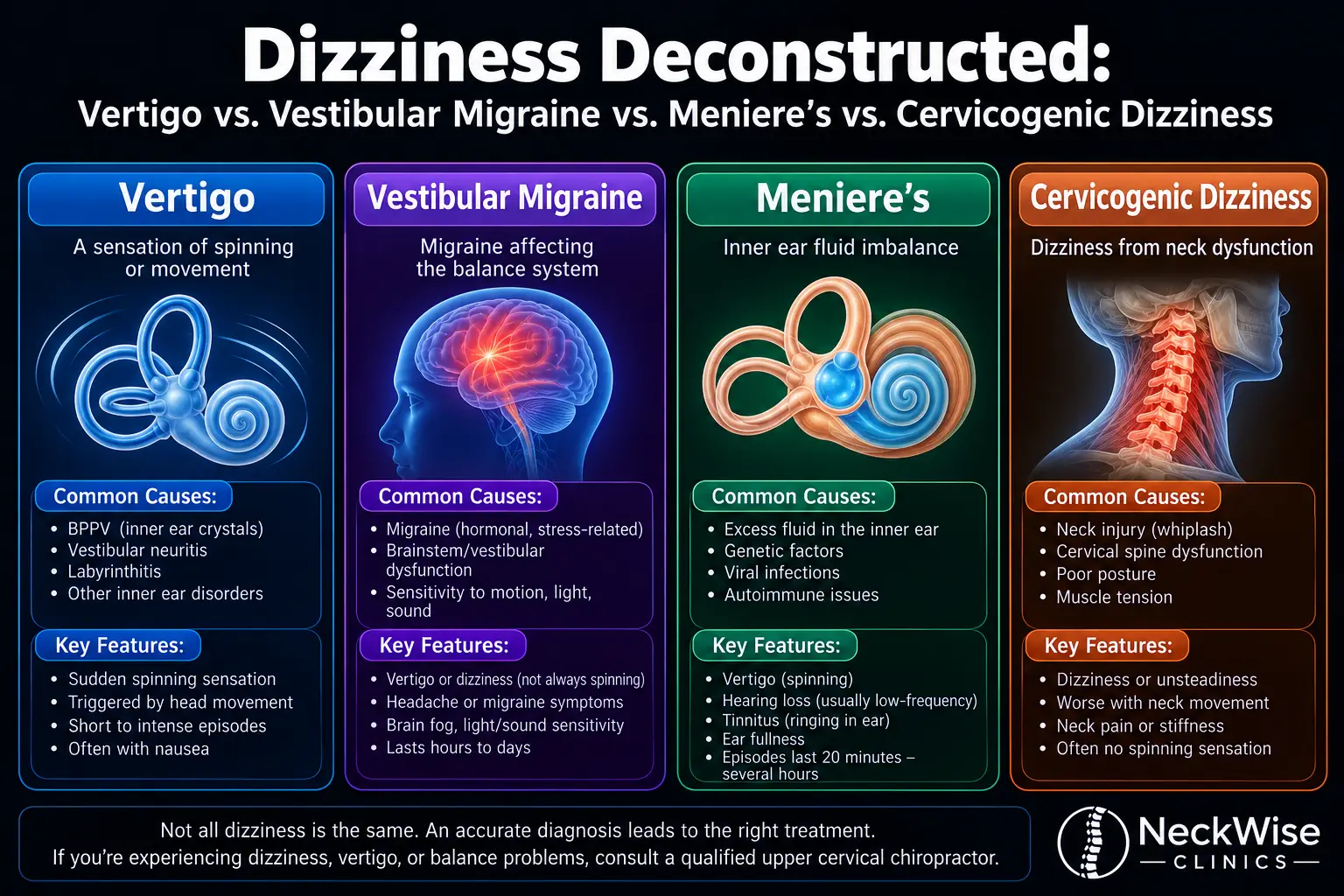
The pain itself often lacks distinctive features. It may feel like a constant pressure, aching, or tightness, and in some patients it carries migraine-like features (throbbing, light and sound sensitivity, nausea) while in others it resembles a chronic tension-type headache. It can be one-sided or affect the whole head. The intensity ranges from moderate background pain to severe, debilitating pain. What unites all cases is the relentless, daily, unremitting nature of the headache.
How common is NDPH? It is genuinely rare. According to a systematic review, the prevalence of NDPH is estimated at 0.03% to 0.1% in the general population, and it is higher in children and adolescents than in adults. The Akershus study of chronic headache in Norway, a population-based study of 30,000 people, found a one-year prevalence of just 0.03%. Despite its rarity, NDPH is clinically important precisely because it is so persistent and so treatment-refractory — it can disrupt lives for years and significantly affect quality of life and mental health.
NDPH affects women somewhat more often than men, though the ratio is more balanced than in migraine. The mean age of onset is around the fourth decade of life, though it can begin anywhere from childhood to old age. And critically for understanding the condition, the onset is frequently associated with a triggering event: an infection or flu-like illness, a stressful life event, minor head or neck trauma, or surgery. Infection and stressful life events are the most commonly cited triggers — a pattern that has become especially relevant in the era of COVID-19.
Why NDPH Is So Often Misdiagnosed
One of the reasons NDPH is so frustrating for patients is that it is frequently mislabeled. Because the pain can have migraine-like or tension-type features, many patients are diagnosed with chronic migraine or chronic tension-type headache and treated accordingly — often without the response those diagnoses would predict.
The ICHD-3 criteria are actually quite specific on this point: even when a patient’s NDPH has features that would otherwise meet criteria for chronic migraine or chronic tension-type headache, the default diagnosis is NDPH whenever its criteria are met. The distinguishing feature is always the history — the daily-from-onset, clearly-remembered, unremitting pattern. A patient who describes increasing headache frequency before the daily pattern began does not have NDPH; a patient who woke up one day with a headache that never left does.
Getting the diagnosis right matters because NDPH behaves differently from the conditions it mimics. It tends to be more treatment-refractory, it follows different prognostic patterns, and it warrants a different evaluation — including ruling out the secondary causes that can imitate NDPH. This is why a careful, accurate diagnosis is the essential first step, and why we take diagnostic clarity so seriously.
It is also why ruling out serious secondary causes is critical. A number of potentially serious conditions can produce a new, persistent headache that resembles NDPH, including spontaneous cerebrospinal fluid leak, idiopathic intracranial hypertension, cerebral venous thrombosis, cervical artery dissection, Chiari malformation, and others. A responsible evaluation of any new persistent headache must consider and screen for these — and we are emphatic that anyone with a new persistent headache, especially with any red-flag features, needs a proper medical and neurological workup. Upper cervical care is never a substitute for that workup.
The Cervicogenic Connection: Where the Neck May Fit
Here is where we can offer something specific and evidence-based, while remaining honest about its limits.
The systematic review of NDPH explicitly states that, while the exact mechanism is unknown, pro-inflammatory cytokines and cervicogenic problems might play a role in its development. “Cervicogenic” means originating in the cervical spine — the neck. This is a meaningful acknowledgment in the research literature that, for at least some NDPH patients, the neck may be part of the picture.
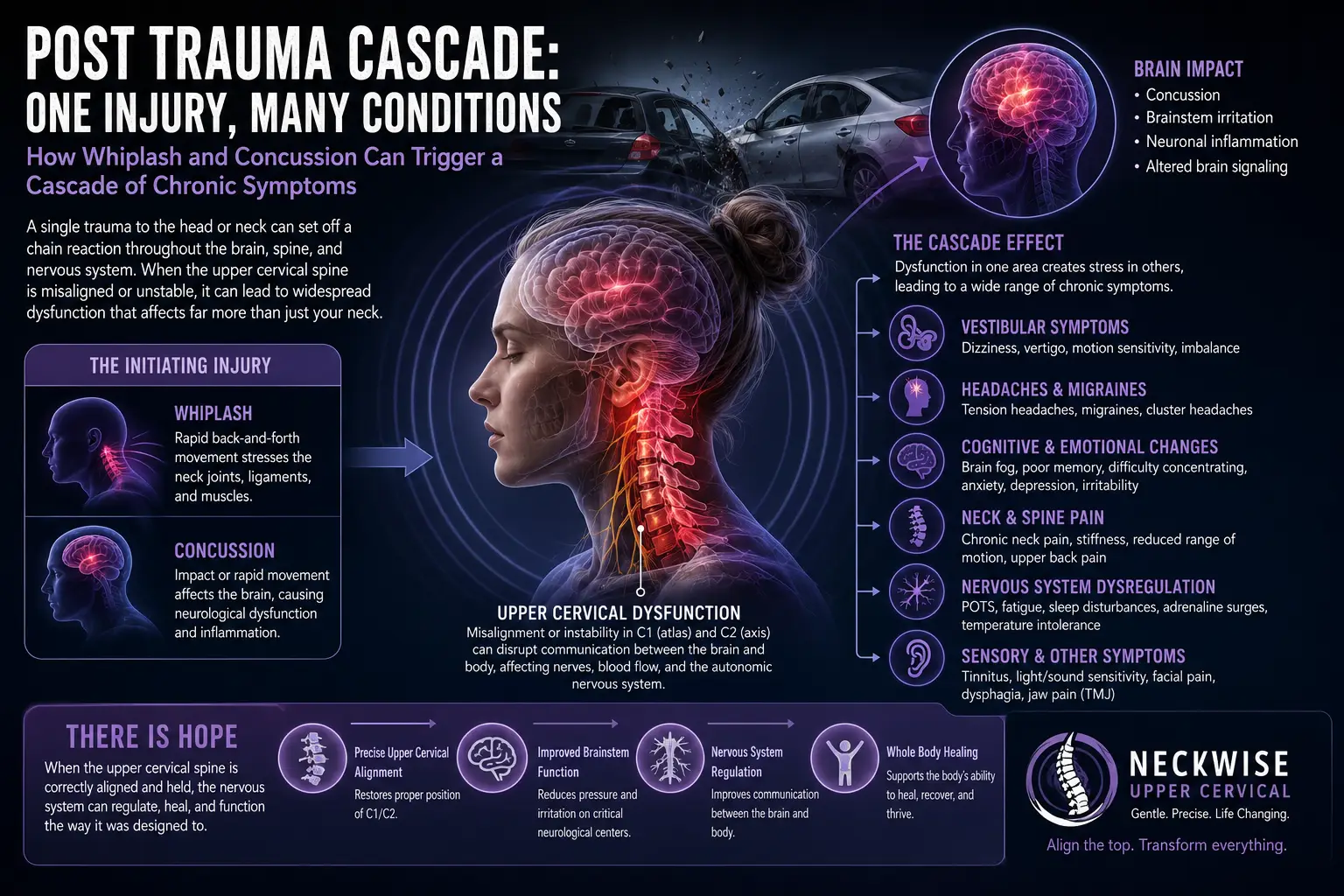
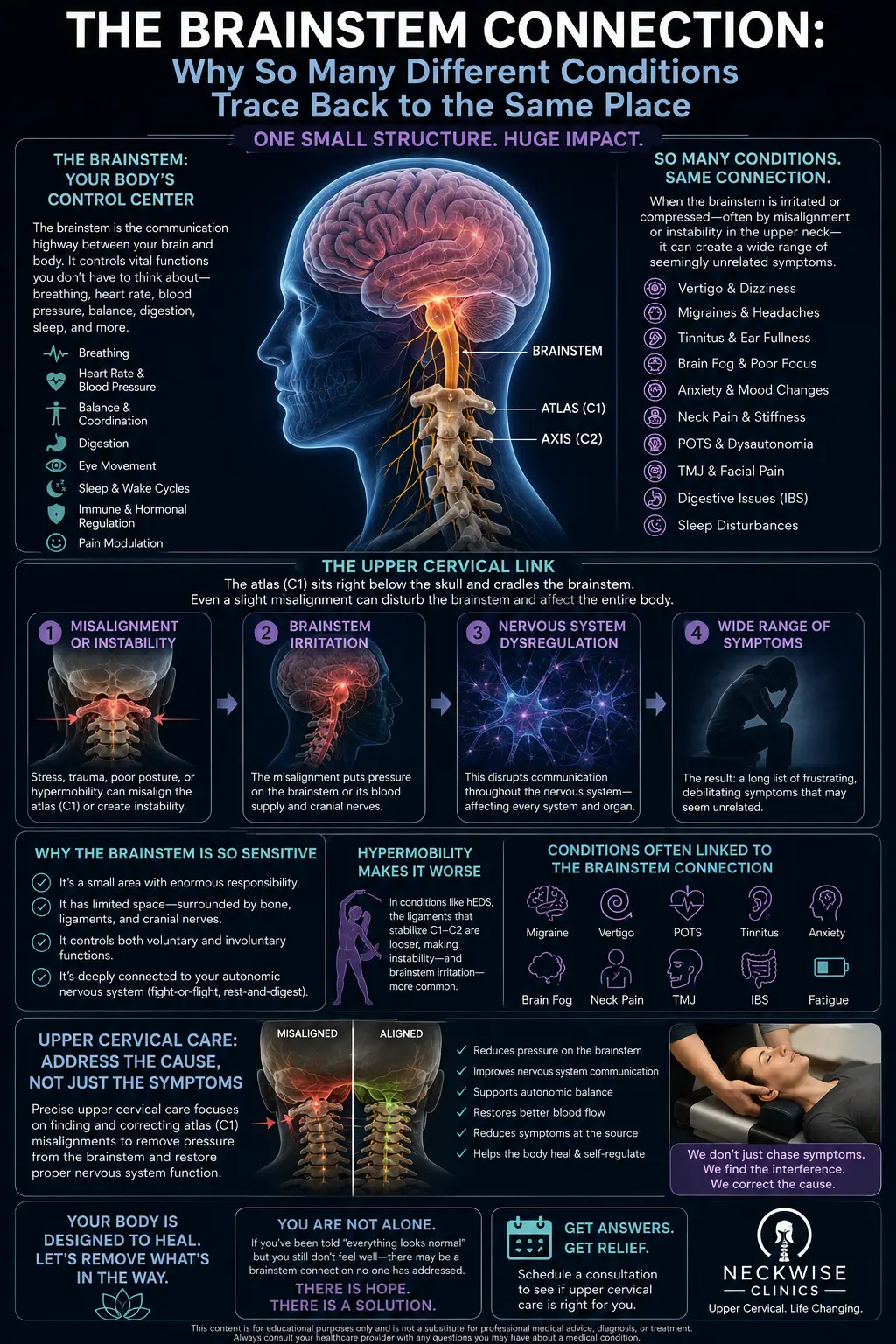
This makes anatomical sense through a structure we have discussed in the context of several headache conditions: the trigeminocervical complex. The trigeminocervical nucleus, located in the brainstem and upper cervical spinal cord, receives sensory input from both the trigeminal nerve (which supplies the face and front of the head) and the upper three cervical spinal nerves (C1, C2, C3, which supply the back of the head and neck). According to clinical references, the trigeminocervical nucleus receives afferents from the trigeminal nerve and the upper three cervical spinal nerves, and this convergence is the neuroanatomical basis for how problems in the upper cervical spine can generate or contribute to head pain. Irritation arising from the upper cervical structures feeds into the same pain-processing center that handles head and facial pain, and chronic input from this region can contribute to the central sensitization that helps perpetuate chronic daily headaches.
There is also the post-infectious angle, which connects NDPH to territory we have explored in depth. Infection is one of the most commonly cited triggers of NDPH, and the COVID-19 pandemic has brought new attention to this. A cross-sectional study in Latin America found that one in four participants with post-COVID headache met NDPH diagnostic criteria, with occipital location, severe intensity, and burning, radiating pain among the most predominant clinical characteristics. The occipital (back of the head) predominance in these post-infectious cases is notable, because it points toward the upper cervical and occipital region — exactly the area that upper cervical care addresses. The pro-inflammatory and post-viral mechanisms implicated in NDPH overlap with those we discuss in conditions like long COVID, where neuroinflammation and the upper cervical region both play roles.
We want to be very clear and very honest here, because this is exactly the kind of condition where careful framing matters most. The cervicogenic contribution is one possible factor among several in a disorder whose mechanism remains genuinely unknown. Upper cervical care is not a proven cure for NDPH — no such cure exists. What the research supports is that the neck may be a contributing factor for some patients, that the trigeminocervical anatomy provides a plausible pathway, and that for patients with a genuine cervicogenic component, addressing the upper cervical spine is a reasonable part of a comprehensive approach. That is a measured, honest claim, and it is the only one the evidence supports.
Why Upper Cervical Care May Help Some NDPH Patients
At Lavender Family Chiropractic, we use the Knee Chest Upper Cervical technique — a precise, gentle method of correcting atlas and axis misalignments without any twisting, popping, or forceful manipulation. For NDPH patients in whom a cervical component is present, this approach may help in a few specific ways.
First, by correcting upper cervical misalignment, we address irritation arising from the C1-C2-C3 region — the upper cervical nerves that feed directly into the trigeminocervical complex. Reducing this chronic afferent input is one way to potentially decrease the input that contributes to the central sensitization underlying chronic daily headache. Second, restoring proper upper cervical alignment helps relieve the chronic suboccipital muscle tension and postural strain that can contribute to cervicogenic head pain. Third, for NDPH patients whose condition followed neck trauma or who have a clear cervicogenic component, addressing the structural source is more logical than only managing the symptom with medication.
We need to set honest expectations, more so than with almost any other condition we discuss. NDPH is one of the most treatment-refractory headache disorders in existence. Even in specialized headache centers, many patients do not respond fully to any intervention, and the literature on NDPH treatment is largely composed of case reports rather than robust trials. Upper cervical care is not a guaranteed solution, and for patients whose NDPH has no cervical component, it may provide little benefit. What we can promise is a thorough, honest evaluation to determine whether a cervical contribution is present, gentle care directed at that component if it is, and complete honesty about what we observe — including telling you directly if we do not see the response we hoped for.
We also strongly believe NDPH should be managed by a multidisciplinary team. We see upper cervical care as one potential component of a broader approach that should include a neurologist or headache specialist, appropriate medical workup to rule out secondary causes, and the medication and other interventions those specialists provide. We coordinate with these providers rather than positioning ourselves as a substitute for them.
What Care Looks Like at Lavender Family Chiropractic
If you come to our Sarasota office for evaluation related to NDPH, here is what to expect.
Your first visit begins with a thorough consultation. Dr. Lavender or Dr. Temple will carefully review your history — the exact date and circumstances of your headache’s onset, any triggering event (infection, stress, trauma, surgery), the character and location of your pain, what has and has not helped, and critically, what medical and neurological workup you have already had. Because ruling out secondary causes is so important in NDPH, we want to know what imaging and specialist evaluation you have undergone, and if you have not had an adequate workup, we will strongly encourage you to get one.
The examination includes a detailed neurological evaluation, assessment of the upper cervical region and suboccipital muscles, palpation for cervical tenderness and trigger points, postural and cervical range-of-motion assessment, and advanced 3D imaging to evaluate your upper cervical alignment. We screen carefully for red flags — any features suggesting a serious secondary headache (fever, progressive worsening, neurological deficits, visual changes, and others) prompt immediate referral for appropriate medical evaluation. Patient safety always comes first.
If the examination suggests a cervical or upper cervical component to your NDPH, we will explain honestly how upper cervical care might fit into your overall management — and we will be equally honest if we do not find evidence of a cervical contribution. We coordinate closely with your neurologist or headache specialist, because NDPH genuinely requires a team approach.
Care, when appropriate, is delivered through the gentle Knee Chest Upper Cervical technique. We offer customized treatment plans tailored to your specific situation, with realistic, honest expectations about what upper cervical care can and cannot accomplish for a condition this challenging.
📞 Call (941) 243-3729 to schedule your complimentary consultation 📅 Book your consultation online 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
What the Research Says About New Daily Persistent Headache
The research on NDPH is limited compared to more common headache disorders, which is itself part of the challenge — but what exists paints a consistent picture of a rare, distinctive, and difficult condition.
The defining systematic review of NDPH established the core facts: the prevalence is estimated at 0.03% to 0.1%, the condition is one of the most treatment-refractory primary headache disorders, patients can pinpoint the exact date of onset, and while the exact mechanism is unknown, pro-inflammatory cytokines and cervicogenic problems may play a role. This review remains the most comprehensive synthesis of what is known about the disorder, and its explicit mention of cervicogenic factors is the key evidence basis for considering the neck.
The ICHD-3 diagnostic framework, summarized in clinical references, establishes that NDPH is daily and unremitting from onset, with patients able to clearly recall the distinct onset, and that NDPH remains the default diagnosis even when migraine or tension-type features are present — reinforcing the importance of the onset history in distinguishing NDPH from the conditions it mimics, and noting the importance of screening for serious secondary causes.
A 2025 retrospective characterization of 466 NDPH cases at a major healthcare system documented the clinical reality: NDPH is classically treatment-resistant, with a mean age of onset around 37 years and a female predominance, though case reports have demonstrated occasional therapeutic benefit from a variety of interventions including osteopathic manipulation — confirming both the refractory nature of the condition and the reality that some patients do respond to some interventions.
The post-infectious connection is documented in the COVID-19 literature. The Latin American cross-sectional study found that one in four participants with post-COVID headache met NDPH criteria, with occipital location, severe intensity, and burning, radiating pain predominating — highlighting both the infectious trigger and the occipital (upper cervical) predominance in these cases.
Finally, the trigeminocervical anatomy that underlies the cervicogenic contribution is well established. According to clinical references on cervicogenic headache, the trigeminocervical nucleus receives afferents from both the trigeminal nerve and the upper three cervical spinal nerves, and aseptic inflammation and neurotransmission within the C-fibers can produce and worsen head pain — providing the anatomical pathway by which upper cervical irritation can contribute to chronic head pain.
This body of research establishes that NDPH is rare, distinctive, and treatment-refractory, that its mechanism is genuinely unknown, that cervicogenic factors are among the possible contributors, and that the trigeminocervical anatomy provides a plausible pathway for upper cervical involvement. It does not establish that upper cervical care cures NDPH — and we do not claim that it does. It establishes that the neck is worth evaluating in a condition where every reasonable avenue deserves consideration.
Lifestyle Factors That Support NDPH Management
Because NDPH is so treatment-refractory, the daily inputs you control take on real importance — not as a cure, but as part of giving yourself every advantage in managing a difficult condition.
Sleep regulation. Poor or irregular sleep worsens nearly every chronic headache disorder. Consistent sleep and wake times, a dark and cool room, and good sleep hygiene support your nervous system’s capacity to regulate pain. Treat sleep as a genuine part of your management plan.
Stress management. Stressful life events are one of the most commonly cited triggers of NDPH onset, and ongoing stress can worsen the condition. Practices that down-regulate the nervous system — meditation, breathwork, gentle movement, therapy, time in nature — are genuinely relevant. Cognitive behavioral therapy in particular has support for chronic headache management.
Posture and screen habits. Forward head posture and sustained downward head tilt strain the upper cervical and suboccipital region that feeds the trigeminocervical complex. Keeping screens at eye level, taking frequent breaks, and maintaining good posture reduces this cervical load.
Avoid medication overuse. One of the most important things to understand about chronic daily headache is that frequent use of acute pain medications can create medication-overuse headache, which compounds the problem. Work with your headache specialist to avoid this trap — it is one of the most common reasons chronic headaches fail to improve.
Anti-inflammatory nutrition. Because pro-inflammatory mechanisms are implicated in NDPH, an anti-inflammatory eating pattern — minimizing processed foods, refined sugars, and seed oils while emphasizing whole foods and omega-3-rich fish — is a reasonable supportive measure. Staying well hydrated matters too.
Hydration. Dehydration is a common headache trigger, and the Florida climate makes it especially relevant. Consistent, adequate hydration is a simple but genuine support.
Identify and track patterns. Keeping a headache diary — noting any fluctuations, triggers, and what helps even slightly — can provide valuable information for you and your care team and can help identify modifiable factors.
Build a support system. NDPH is isolating and can take a real toll on mental health. Connection with supportive people, and professional mental health support when needed, is an important part of living with a chronic, difficult condition.
If you found this guide useful, you may also want to read our blog on occipital neuralgia, another headache condition with a direct upper cervical connection that can sometimes overlap with or be confused for persistent daily headache.
Serving Sarasota and the Surrounding Communities
Lavender Family Chiropractic is located in Sarasota, Florida, at 5899 Whitfield Avenue, Suite 107 — at the corner of University and Whitfield. From this central location, we serve patients throughout the region, including Bradenton, Lakewood Ranch, Palmetto, Parrish, Venice, Osprey, Nokomis, Ellenton, Ruskin, Myakka City, North Port, and the greater Tampa Bay area. Patients also travel from St. Pete, Riverview, and Manatee County to receive specialized upper cervical care here.
NDPH is the kind of condition where patients have often searched for years for someone who takes their experience seriously, understands the disorder, and offers an honest assessment of every reasonable avenue. We cannot promise to cure a condition that has no known cure — but we can offer a careful evaluation of whether the upper cervical component is part of your picture, and honest, gentle care if it is. If that is what you are looking for, we encourage you to reach out.
Top 15 FAQs About New Daily Persistent Headache and Upper Cervical Chiropractic Care
1. What is new daily persistent headache? NDPH is a primary headache disorder defined by a headache that is daily and unremitting from the moment it begins. Patients can pinpoint the exact date of onset, the headache becomes continuous within 24 hours, and it persists for more than three months — typically in someone without a significant prior headache history.
2. How is NDPH different from chronic migraine? The key difference is the onset. Chronic migraine usually evolves gradually from episodic migraine that becomes more frequent. NDPH is daily and constant from day one, with a clearly remembered onset. Even when NDPH has migraine-like features, the daily-from-onset history makes it NDPH rather than chronic migraine.
3. Can upper cervical chiropractic cure NDPH? No — and we want to be completely honest about this. There is no known cure for NDPH, and its mechanism is poorly understood. What upper cervical care can do is address a cervical or cervicogenic component if one is present, which the research identifies as a possible contributor for some patients. It is one part of a broader, multidisciplinary approach, not a cure.
4. Why might my neck be involved in NDPH? The systematic review of NDPH explicitly identifies cervicogenic (neck-origin) problems as a possible contributing factor. Anatomically, the upper cervical nerves feed into the trigeminocervical complex — the same pain-processing center that handles head and facial pain — so upper cervical irritation can contribute to chronic head pain.
5. My NDPH started after an illness. Is that common? Yes. Infection or flu-like illness is one of the most commonly cited triggers of NDPH. Research on post-COVID headache found that a substantial portion of patients met NDPH criteria, frequently with occipital (back of the head) location — pointing toward the upper cervical region.
6. Is upper cervical care safe for NDPH? The Knee Chest Upper Cervical technique is exceptionally gentle, with no twisting or forceful manipulation. It is generally very safe. We perform a thorough evaluation, screen for red flags, and coordinate with your medical providers.
7. Do I still need to see a neurologist? Yes, absolutely. NDPH should be managed by a multidisciplinary team that includes a neurologist or headache specialist. A proper medical workup to rule out serious secondary causes is essential. We see upper cervical care as one potential component of a broader approach, never a substitute for appropriate medical care.
8. What serious conditions can mimic NDPH? Several, including spontaneous cerebrospinal fluid leak, idiopathic intracranial hypertension, cerebral venous thrombosis, cervical artery dissection, and Chiari malformation, among others. This is why a thorough medical and neurological workup is essential for anyone with a new persistent headache, and why we screen carefully and refer when needed.
9. Why is NDPH so hard to treat? Because its mechanism is poorly understood and it is inherently treatment-refractory. Even specialized headache centers find many NDPH patients do not respond fully to any intervention. The treatment literature is largely case reports rather than robust trials, which is part of why a comprehensive, multi-angle approach is reasonable.
10. How will I know if upper cervical care might help me? The only way to know is a thorough evaluation. We will assess whether your NDPH has a cervical or upper cervical component, and give you an honest assessment. If we do not find evidence of a cervical contribution, we will tell you that directly rather than recommend care that is unlikely to help.
11. Can stress cause NDPH? A stressful life event is one of the most commonly cited triggers of NDPH onset, and ongoing stress can worsen the condition. Stress management is a genuinely relevant part of overall management, though it is not a cure.
12. Will I have this headache forever? NDPH follows different courses in different people. Some patients have a self-limiting form that eventually resolves; others have a persisting form that continues for years; and some have a relapsing-remitting pattern. The course is difficult to predict, which is one of the frustrating aspects of the condition.
13. Can a head or neck injury cause NDPH? Minor head trauma is among the recognized triggers of NDPH. For patients whose NDPH followed neck trauma, a cervicogenic component is more plausible, and the upper cervical evaluation is especially relevant.
14. What should I avoid with NDPH? One of the most important things to avoid is medication-overuse headache from frequent use of acute pain medications, which can compound the problem. Work with your headache specialist on this. Also avoid the trap of trying treatments without an accurate diagnosis and proper workup first.
15. How do I get started? Call our Sarasota office at (941) 243-3729 or book your consultation online. We will review your history, perform a thorough examination, screen for red flags, coordinate with your medical team, and give you an honest assessment of whether upper cervical care fits into your management.
Take the Next Step
New daily persistent headache is one of the most challenging conditions in all of headache medicine — rare, poorly understood, and notoriously resistant to treatment. We will not promise you a cure, because none exists, and because honesty is the foundation of trustworthy care. What we can offer is a careful, honest evaluation of whether a cervical or upper cervical component is contributing to your headache, gentle care directed at that component when it is present, and close coordination with the neurologists and specialists who should be part of your team.
If you are in Sarasota, Bradenton, Lakewood Ranch, or anywhere in the surrounding region and you are living with the relentless daily pain of NDPH, Dr. Rusty Lavender and Dr. Jacob Temple at Lavender Family Chiropractic are here to give you an honest assessment of whether the upper cervical piece is part of your picture — and to be a thoughtful part of your broader care team.
📞 Call (941) 243-3729 today to schedule your complimentary consultation 📅 Book online here 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield