By Dr. Rusty Lavender
Cluster Headaches: If you have experienced a cluster headache, you do not need anyone to tell you how severe it is. The pain is sudden, explosive, and almost unimaginable in its intensity — typically centered around one eye or the temple, often described as a hot poker or knife being driven into the head. The attacks are short by clock time, lasting 15 to 180 minutes, but the intensity is so unrelenting that patients cannot sit still, cannot lie down, and often pace, rock, or even strike their heads against walls trying to find relief. The eye on the affected side waters and reddens. The nostril on that side runs or congests. The eyelid may droop. And then, just as suddenly as it began, the attack ends — leaving you exhausted, drained, and dreading the next one. Because with cluster headache, there is always a next one. They come in clusters lasting weeks to months, often striking at the same time each day, sometimes waking patients from sleep with the precision of an alarm clock.
Cluster headaches have earned the grim nickname “suicide headaches” for a reason. They are considered among the most severe pain conditions in all of medicine, more painful by many patient accounts than kidney stones, childbirth, or gunshot wounds. We want to be honest with you from the very first sentence, because honesty matters most for a condition this severe: cluster headache is a serious neurological disorder driven primarily by hypothalamic dysfunction, and its acute management is a medical priority. The first-line acute treatments — high-flow oxygen and injectable or nasal triptans — are essential, evidence-based, and we strongly support them. Upper cervical chiropractic care is not a substitute for these treatments, and any provider who suggests otherwise is overpromising on a condition that demands proper medical care.
What we can offer at Lavender Family Chiropractic in Sarasota, Florida, is something specific and grounded in the actual research: the cervical-input component of cluster headache pathophysiology is genuine, the trigeminocervical complex at the C1-C2 dorsal horn is a well-documented part of the pain mechanism, and the greater occipital nerve — arising directly from C2 — is so important in cluster headache that occipital nerve blocks and stimulation are recognized treatment options in the medical literature. For cluster headache patients pursuing a multidisciplinary approach, addressing the upper cervical and occipital contribution may be a reasonable adjunctive piece of a broader strategy that remains anchored in proper medical management. This guide is for anyone in Sarasota, Bradenton, Lakewood Ranch, or the surrounding areas who is living with cluster headache and wants to understand it accurately — including where upper cervical care honestly fits.
What Are Cluster Headaches?
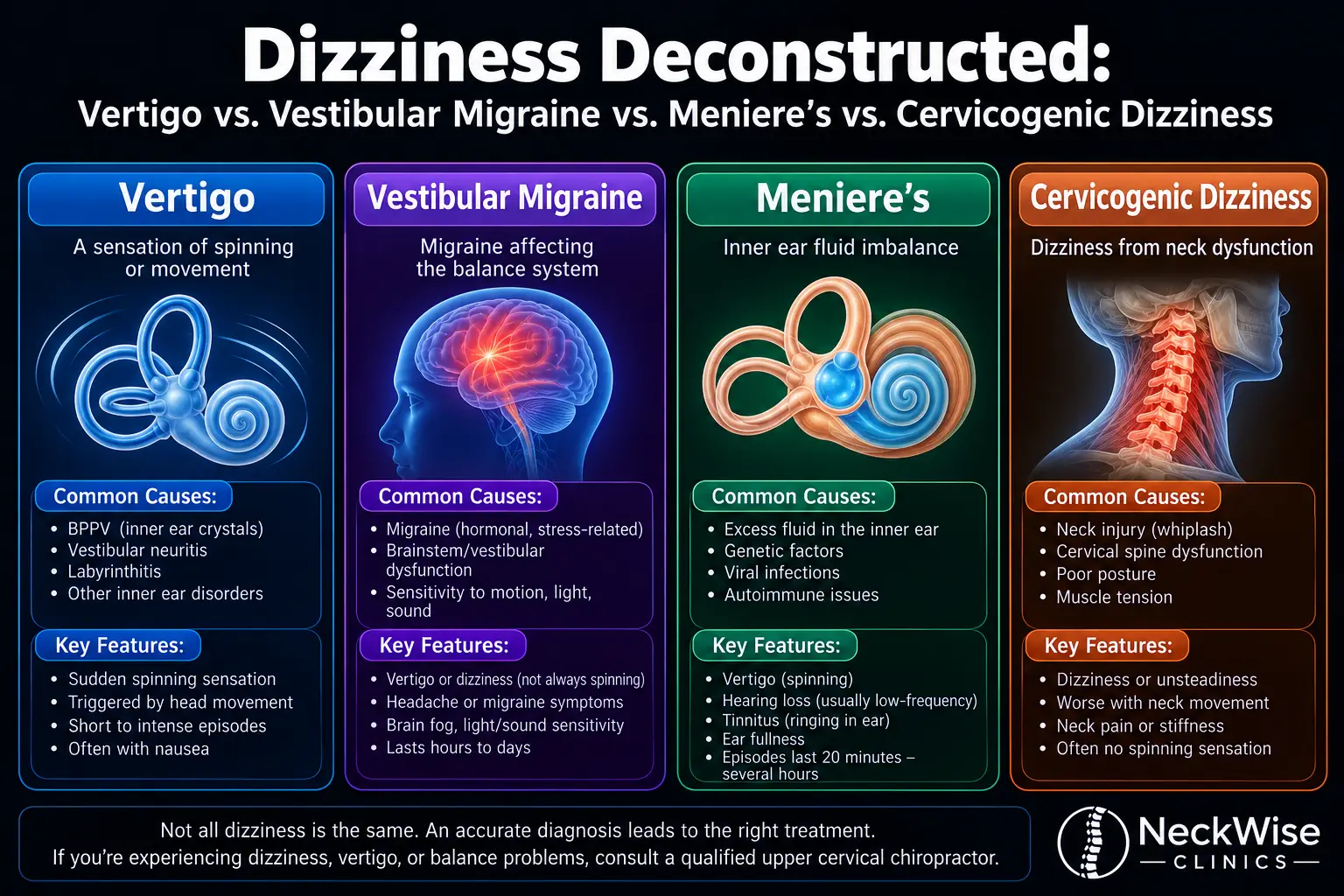
Cluster headache is the most common of a group of headache disorders called trigeminal autonomic cephalalgias (TACs). The defining features of a TAC are intense, strictly one-sided headache attacks accompanied by autonomic symptoms on the same side as the pain — features that distinguish cluster headache from migraine, tension headache, and most other primary headache disorders.
According to the International Classification of Headache Disorders (ICHD-3), the diagnostic criteria for cluster headache require: severe or very severe one-sided pain localized in the orbital, supraorbital, or temporal region; attacks lasting 15 to 180 minutes when untreated; and accompaniment by at least one of a specific set of autonomic features on the same side as the pain — including conjunctival redness or tearing, nasal congestion or runny nose, eyelid swelling, forehead and facial sweating, miosis (pupil constriction) or ptosis (drooping eyelid), or a sense of restlessness or agitation. The attack frequency ranges from once every other day up to eight per day during a cluster period.
The pattern of cluster headache divides patients into two subtypes. Episodic cluster headache is the more common form, in which attacks occur in cluster periods lasting weeks to months, followed by remission periods of at least three months. Chronic cluster headache is the more severe form, in which attacks continue for more than a year without significant remission or with remissions shorter than three months. Both forms produce the same characteristic attacks; they differ in how the condition cycles over time.
How common is cluster headache? It is genuinely rare, though more recent data suggests it may be more common than once thought. According to StatPearls, the prevalence of cluster headache is approximately 0.1% of the population, affecting about 1 in 1,000 people, and it is considered one of, if not the most severe, primary headache disorders. A 2025 large-scale electronic health record analysis using the Epic Cosmos database identified 152,727 patients with cluster headache across U.S. healthcare systems, with a five-year prevalence of 56.7 per 100,000, and notably, all four trigeminal autonomic cephalalgias showed higher prevalence in women — a finding that challenges the historical assumption of strong male predominance. Cluster headache patients in this study showed elevated rates of nicotine, alcohol, and cannabis use disorders, reflecting both the severity of the condition and the substances some patients turn to in trying to manage it.
Cluster headaches are also notoriously misdiagnosed. According to clinical references, patients with cluster headache often go up to five years without receiving the correct clinical diagnosis, commonly misdiagnosed as migraine, sinus headache, dental problems, or trigeminal neuralgia. The distinctive features — strict unilaterality, the relatively short duration, the autonomic symptoms, the cluster pattern over time, and the often clockwork-like timing — are what set cluster headache apart, but they are routinely missed in patients who do not see headache specialists.
The personal toll of cluster headache is severe. The pain intensity is comparable to or exceeds that of childbirth or kidney stones in many patient accounts, and the recurrent, predictable nature of attacks during cluster periods is devastating to work, family life, and mental health. Suicide rates and suicidal ideation are elevated in patients with this condition, which is one of the reasons aggressive, effective treatment is so important — and why honest, supportive care matters.
The Hypothalamic and Trigeminocervical Mechanism
Understanding cluster headache pathophysiology is essential to understanding where any intervention — including upper cervical care — fits into its management. And to be honest from the start, the primary driver of cluster headache is not in the cervical spine. The primary driver is in the hypothalamus.
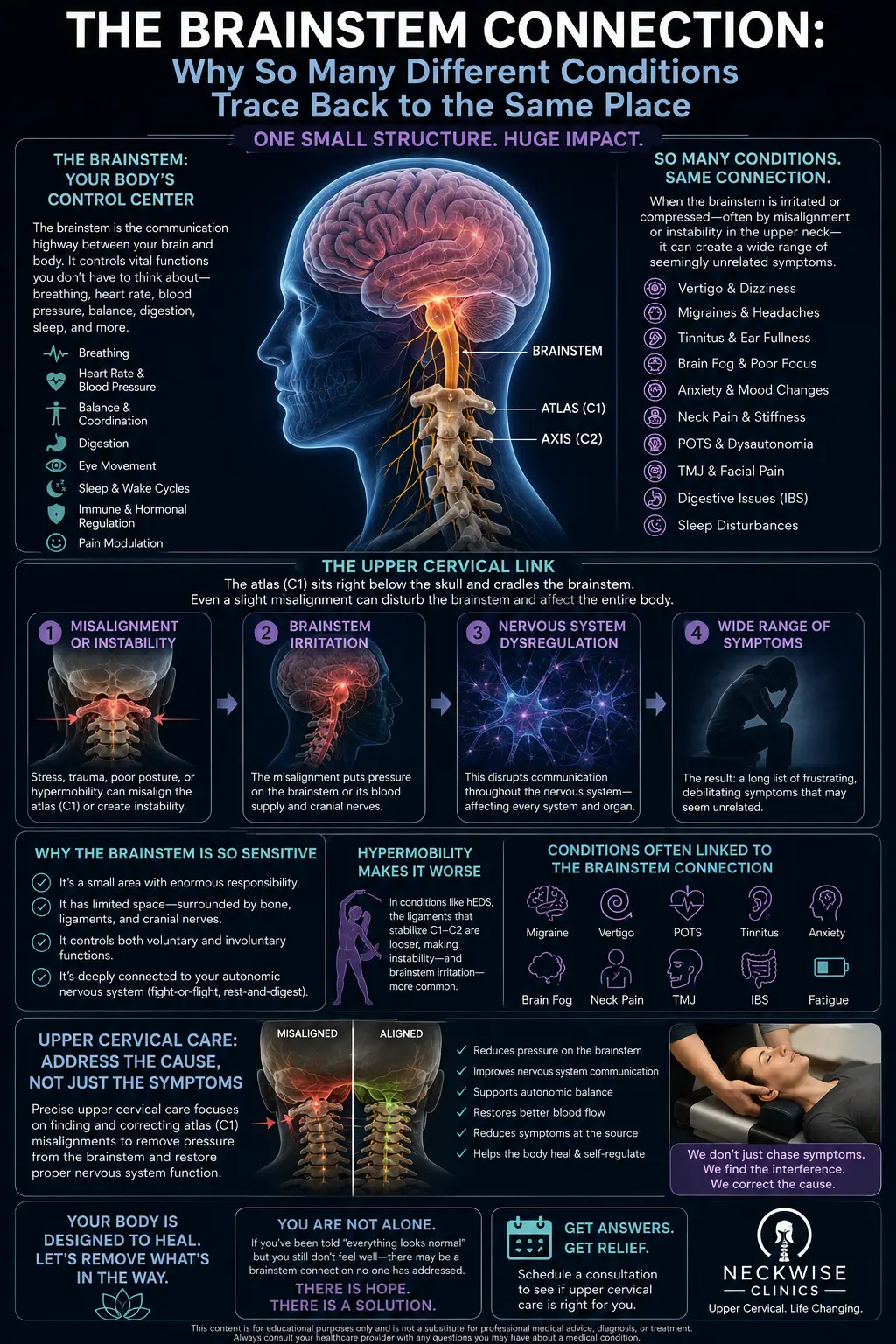
Functional imaging studies have consistently shown activation of the posterior hypothalamus during cluster attacks. The remarkably circadian and circannual patterns of cluster headache — attacks at the same time of day, cluster periods at the same time of year — are thought to reflect the hypothalamus’s role as the body’s master biological clock. The autonomic features of cluster attacks (the tearing, nasal congestion, partial Horner’s syndrome) reflect activation of the cranial parasympathetic outflow through the trigeminal-autonomic reflex, which is centrally coordinated.
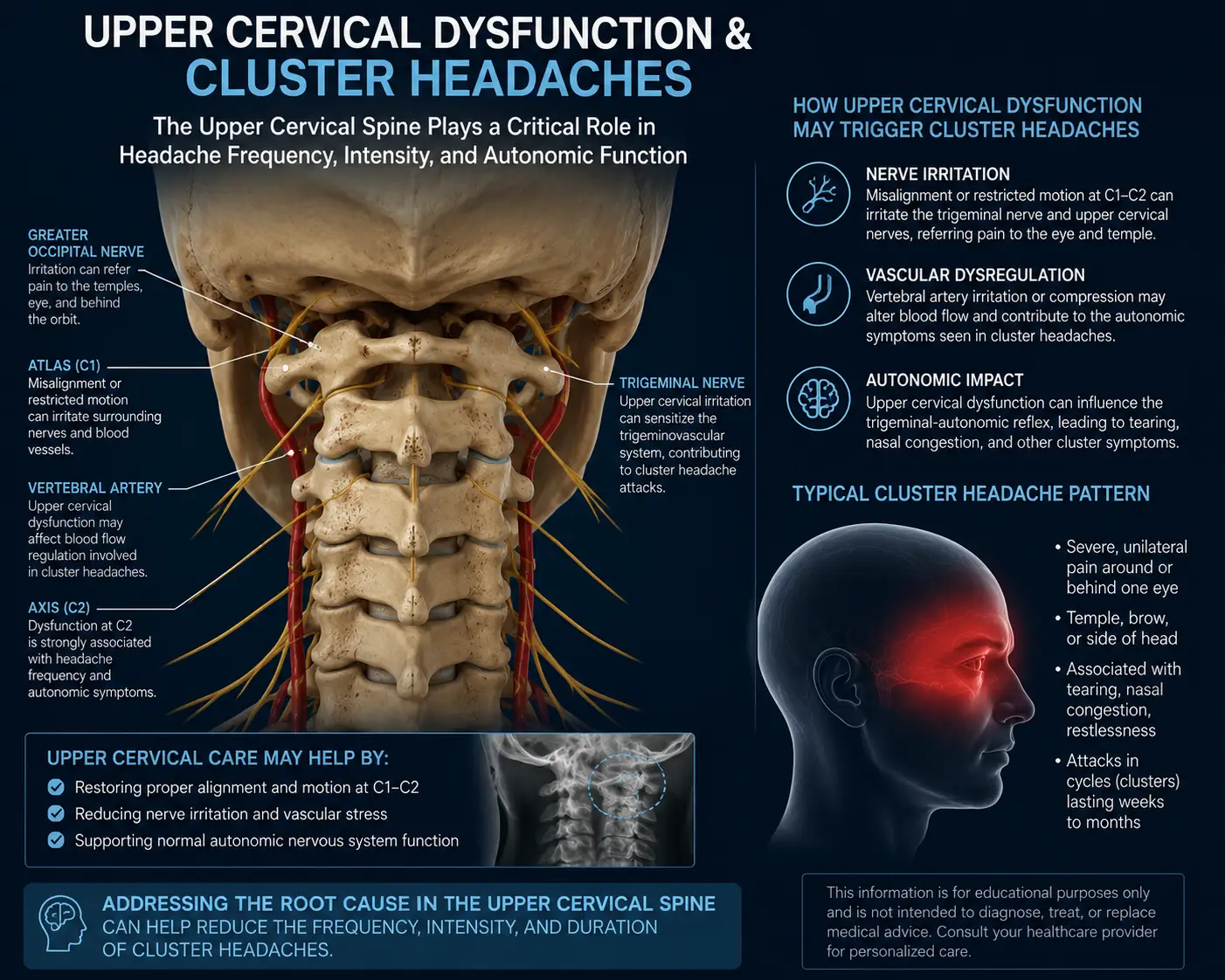
But here is the part that matters for the cervical connection: the pain itself is generated and processed through the trigeminocervical complex. According to a review of cluster headache pain mechanisms, the trigeminocervical complex is part of the brainstem and includes the caudal part of the trigeminal nucleus caudalis and the dorsal horns of the C1-C2 segments of the spinal cord, and is the central convergence point where trigeminal and cervical afferents come together. The same review establishes that cluster headache pain involves central sensitization of the trigeminocervical neurons — the same neurons that process input from both the face (via the trigeminal nerve) and the back of the head and upper neck (via the C1, C2, and C3 cervical nerves).
This convergence is not a small detail. It is precisely why cluster headache pain, although typically felt around the eye and temple, can be modulated by interventions targeting the cervical and occipital region. According to clinical research, the greater occipital nerve, which arises directly from C2, provides the most accessible peripheral access point to the trigeminocervical-hypothalamic system, and greater occipital nerve blocks have been shown to be effective for cluster headache through convergence of cervical and trigeminal afferents on second-order neurons in the brainstem. The same review notes the existence of a trigeminocervical-hypothalamic connection — meaning that interventions at the cervical and occipital level can, through this convergence, influence the central pain mechanism of cluster headache.
This is the evidence-based foundation for considering the cervical component in cluster headache, and it is more robust than many patients realize. The fact that occipital nerve stimulation and occipital nerve blocks are established treatments for cluster headache — and that their effectiveness is explained through the trigeminocervical convergence at C1-C2 — tells you that the cervical input to the cluster headache mechanism is real and clinically relevant.
We want to be precise about what this means. The hypothalamus is the primary driver of cluster headache, and we cannot directly modify the hypothalamus through chiropractic care. The trigeminocervical complex is a central part of the pain mechanism, and its cervical inputs (C1-C2-C3) are the part that upper cervical alignment can plausibly influence. Upper cervical care addresses the cervical-input side of a complex disorder; it does not address the hypothalamic side. This is why we frame upper cervical care as a potential adjunctive piece of management for selected patients, never as a primary or stand-alone treatment.
Why Upper Cervical Care May Help Some Cluster Headache Patients
At Lavender Family Chiropractic, we use the Knee Chest Upper Cervical technique — a precise, gentle method of correcting atlas and axis misalignments without any twisting, popping, or forceful manipulation. For cluster headache patients pursuing a comprehensive approach to their condition, addressing the cervical input to the trigeminocervical complex may offer a few specific benefits, all positioned as adjunctive to proper medical care.
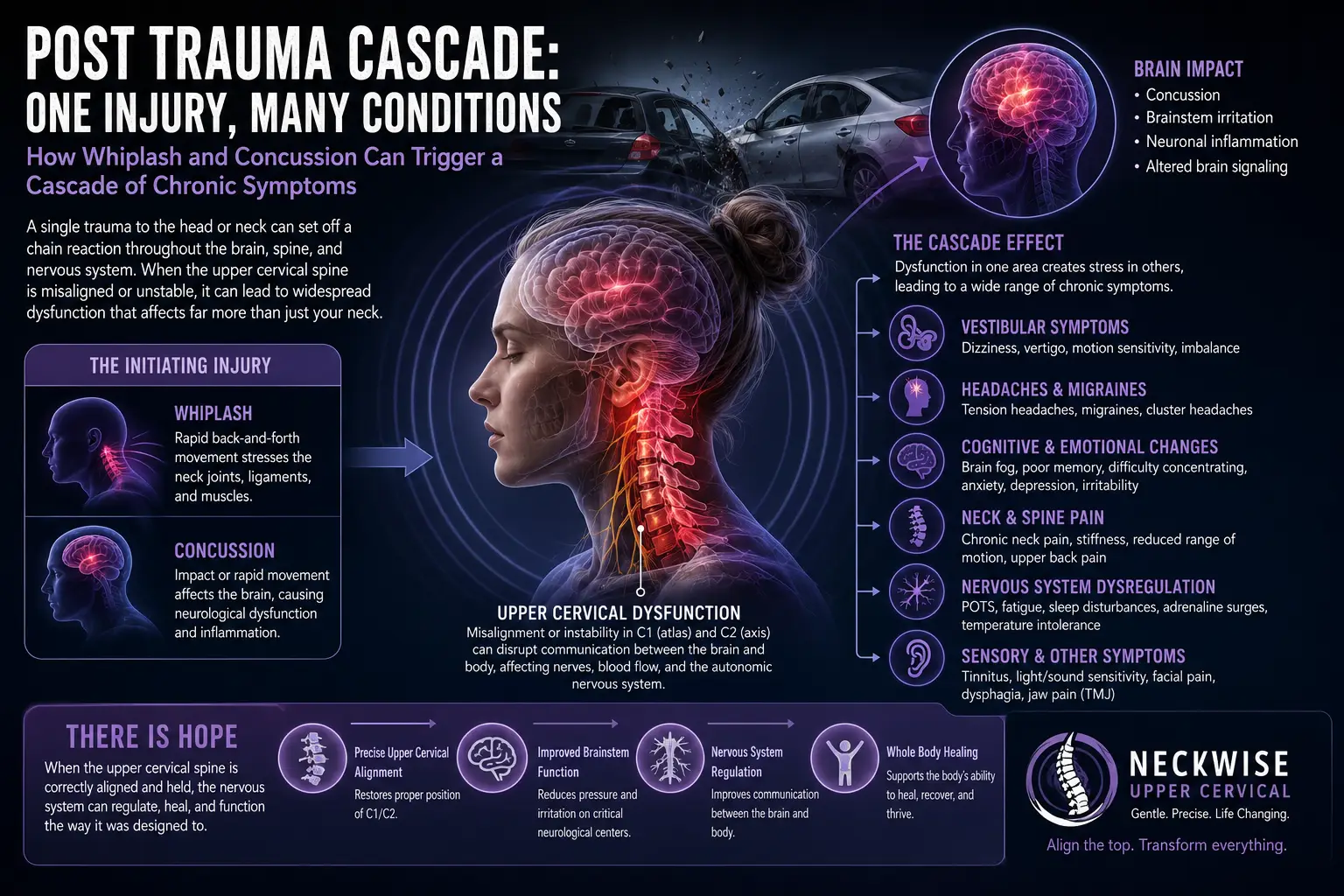
First, by correcting upper cervical misalignment, we reduce chronic afferent input from the C1-C2-C3 region — the cervical inputs to the trigeminocervical complex. Reducing this chronic cervical input may help decrease central sensitization in the same trigeminocervical neurons that generate cluster headache pain. Second, restoring proper upper cervical alignment helps relieve chronic suboccipital muscle tension that can irritate the greater occipital nerve, the same nerve targeted by the occipital nerve blocks that are an established cluster headache treatment. Third, for cluster headache patients who also have neck pain, postural strain, or a history of head or neck trauma contributing to their overall pain picture, addressing the upper cervical component may help with the broader chronic load on the system, even if it does not directly affect the hypothalamic mechanism.
We need to set very honest expectations here, more than with most conditions. Cluster headache requires aggressive medical management — high-flow oxygen for acute attacks, injectable or nasal triptans, preventive medications like verapamil during cluster periods, and in many cases galcanezumab, prednisone bridges, occipital nerve blocks, or other interventions guided by a neurologist or headache specialist. The medical management of cluster headache is well-evidenced and life-changing for many patients, and we strongly support it. Upper cervical care is not a substitute for these treatments. It is not an acute attack therapy. We do not claim it cures cluster headache, and we do not encourage patients to forego medical care in favor of it. What we offer is an adjunctive evaluation of the cervical contribution as one piece of a comprehensive, multidisciplinary approach.
There is also a critical safety point. Because cluster headache is so severe and because acute attacks require immediate intervention, any cluster headache patient must have a clear, working acute-attack plan in place with their medical team. Oxygen and triptans for acute attacks must be available. If you do not have an acute-attack plan, your first priority should be getting one from a neurologist or headache specialist — not adding a complementary therapy.
What Care Looks Like at Lavender Family Chiropractic
If you come to our Sarasota office for evaluation related to cluster headache, here is what to expect.
Your first visit begins with a thorough consultation. Dr. Lavender or Dr. Temple will review your full history — the character and pattern of your attacks, their duration and frequency, the autonomic features, your cluster periods and remission history, your acute and preventive medication regimen, your neurology/headache specialist involvement, and any other contributing factors. Because the diagnosis of cluster headache itself requires specialist evaluation, we want to know that you have or are pursuing appropriate medical care. If you have not yet been formally evaluated by a neurologist or headache specialist, we will strongly encourage that as your first priority before considering chiropractic care as adjunctive.
The examination includes a detailed neurological evaluation, assessment of the upper cervical region and suboccipital muscles, palpation of the greater occipital nerve and surrounding structures, postural and cervical range-of-motion assessment, and advanced 3D imaging to evaluate your upper cervical alignment. We screen carefully for red flags — any features suggesting a secondary cause (cluster-mimicking lesions in the pituitary, posterior fossa, or carotid region, for example) prompt immediate referral for appropriate medical evaluation.
If the examination suggests an upper cervical and occipital component that could be addressed as part of your broader management, we will explain honestly how upper cervical care might fit — and where its limits are. We coordinate closely with your headache specialist, because cluster headache fundamentally requires their involvement. We do not see ourselves as the primary manager of this condition; we see ourselves as a potential adjunctive piece for selected patients.
Care, when appropriate, is delivered through the gentle Knee Chest Upper Cervical technique. We offer customized treatment plans tailored to your specific situation, with realistic expectations about what upper cervical care can and cannot accomplish for a condition this complex.
📞 Call (941) 243-3729 to schedule your complimentary consultation 📅 Book your consultation online 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
What the Research Says About Cluster Headache and the Trigeminocervical Connection
The research on cluster headache is substantial, and the trigeminocervical and cervical aspects are well documented within it.
The epidemiological foundation is established. According to StatPearls, cluster headache affects approximately 0.1% of the population, is one of the most severe primary headache disorders, and is commonly misdiagnosed for up to five years before receiving the correct diagnosis, highlighting both the rarity and the diagnostic challenge.
A 2025 large-scale analysis of U.S. electronic health records identified 152,727 patients with cluster headache, established a five-year prevalence of 56.7 per 100,000, and notably documented that all four trigeminal autonomic cephalalgias showed higher prevalence in women — providing the most comprehensive U.S. prevalence data to date and updating long-held assumptions about sex distribution.
The pathophysiological foundation is well characterized. According to a comprehensive review in The Lancet Neurology, cluster headache is now thought to involve synchronized abnormal activity in the hypothalamus, the trigeminovascular system, and the autonomic nervous system, with cluster headache classified as the most common trigeminal autonomic cephalalgia — establishing the multi-system nature of the disorder.
The trigeminocervical role is documented in detail. According to a review of pain mechanisms, the trigeminocervical complex includes the caudal part of the trigeminal nucleus caudalis and the dorsal horns of the C1-C2 segments of the spinal cord, where trigeminal and cervical afferents converge — and central sensitization of these neurons is integral to the pain mechanism of cluster headache and related disorders — providing the anatomical and physiological basis for the cervical contribution.
The clinical relevance of the cervical and occipital component is confirmed by treatment evidence. A PMC case report on greater occipital nerve blockade documented that the greater occipital nerve, arising from C2, provides access to the trigeminocervical-hypothalamic system, and that GON blockade decreases sensory input to the spinal trigeminal nucleus and interrupts the trigeminal autonomic reflex pathway — making it an effective intervention for cluster headache attacks, with anatomical and functional convergence of cervical and trigeminal pathways established in humans.
This body of research establishes that cluster headache involves the hypothalamus, the trigeminovascular system, and the autonomic nervous system; that the trigeminocervical complex at C1-C2 is integral to pain processing; that the greater occipital nerve from C2 is a clinically relevant peripheral access point to the central mechanism; and that occipital-targeted interventions are recognized treatments. The cervical input to cluster headache is real, well-documented, and clinically meaningful — providing the evidence-based foundation for considering upper cervical care as one part of a multidisciplinary approach.
Lifestyle Factors That Support Cluster Headache Management
Because cluster headache is so severe and so dependent on proper medical management, lifestyle factors are best understood as supportive measures alongside — not substitutes for — medical care.
Strict alcohol avoidance during cluster periods. Alcohol is one of the most reliable triggers of cluster attacks during active cluster periods, often provoking an attack within an hour. Most patients learn to avoid alcohol completely while in a cluster period, though tolerance often returns during remission.
Smoking cessation. Cluster headache patients have notably elevated rates of nicotine use, and while smoking is not directly causative, there is an association that suggests cessation is wise — not least because smoking is harmful in many other ways.
Sleep regularity. Because cluster headache is so circadian, irregular sleep can disrupt the patterns and trigger attacks. Maintaining consistent sleep and wake times — particularly during cluster periods — supports the hypothalamic regulation that cluster headache disrupts.
Avoid altitude exposure during clusters. Reduced oxygen at altitude can trigger cluster attacks, and many patients learn to avoid flying or traveling to high altitudes during active periods.
Maintain your oxygen and acute medications. This is not optional. Make sure you have your high-flow oxygen tank serviced and refilled, your injectable or nasal triptan supply current, and a clear written acute-attack plan from your headache specialist. These save people from the worst of cluster headache.
Identify other triggers. Some patients have additional individual triggers — certain foods, strong smells, heat, emotional stress, or others. Tracking attacks in a headache diary can help identify patterns.
Mental health support. Cluster headache takes a profound toll on mental health, and suicidal ideation rates are elevated. Counseling, support groups, and proactive mental health care are not optional add-ons; they are essential parts of managing this condition.
Connect with the cluster headache community. Organizations like Clusterbusters provide community, resources, and advocacy specific to cluster headache patients. Knowing you are not alone — and learning from others who have managed this condition — is genuinely valuable.
If you found this guide useful, you may also want to read our blog on occipital neuralgia, another headache condition involving the greater occipital nerve and the C2 region that can sometimes coexist with or be confused for cluster headache.
Serving Sarasota and the Surrounding Communities
Lavender Family Chiropractic is located in Sarasota, Florida, at 5899 Whitfield Avenue, Suite 107 — at the corner of University and Whitfield. From this central location, we serve patients throughout the region, including Bradenton, Lakewood Ranch, Palmetto, Parrish, Venice, Osprey, Nokomis, Ellenton, Ruskin, Myakka City, North Port, and the greater Tampa Bay area. Patients also travel from St. Pete, Riverview, and Manatee County to receive specialized upper cervical care here.
Cluster headache is one of the most severe conditions in all of medicine, and patients who carry it deserve respectful, honest care from every provider on their team. We will not promise you a cure, because none exists for cluster headache. What we can offer is a careful, honest evaluation of whether the upper cervical and occipital component is part of your picture, gentle care directed at that component when appropriate, and close coordination with the neurologist or headache specialist who should be your primary care manager for this condition.
Top 15 FAQs About Cluster Headaches and Upper Cervical Chiropractic Care
1. What are cluster headaches? Cluster headache is a primary headache disorder classified as a trigeminal autonomic cephalalgia. It is characterized by attacks of severe, strictly one-sided pain around the eye or temple, lasting 15 to 180 minutes, accompanied by autonomic symptoms on the same side as the pain (tearing, nasal congestion, eyelid drooping), and occurring in cluster periods over time.
2. How is cluster headache different from migraine? Several ways. Cluster headache is strictly unilateral and stays on the same side during a cluster period; migraine can switch sides. Cluster attacks are shorter (15-180 minutes versus 4-72 hours for migraine). Cluster patients are typically restless and agitated during attacks, while migraine patients seek stillness. The autonomic features (tearing, runny nose, eyelid changes) and clockwork timing are characteristic of cluster, not migraine.
3. Can upper cervical chiropractic cure cluster headaches? No — and we want to be completely honest about this. Cluster headache is a serious neurological disorder driven primarily by hypothalamic dysfunction, and no cure exists. What upper cervical care can do is address the cervical input to the trigeminocervical complex, which is a real part of the pain mechanism, as one adjunctive piece of a broader, multidisciplinary approach anchored in proper medical care.
4. Is upper cervical care safe for cluster headache patients? The Knee Chest Upper Cervical technique is exceptionally gentle, with no twisting or forceful manipulation. It is generally very safe and is not known to trigger cluster attacks. We screen carefully for red flags and coordinate with your headache specialist.
5. Why is the cervical spine involved in cluster headache? Because the trigeminocervical complex — where trigeminal and cervical afferents converge in the brainstem and upper spinal cord at C1-C2 — is integral to the pain mechanism of cluster headache. The greater occipital nerve from C2 is so important that occipital nerve blocks and stimulation are recognized cluster headache treatments.
6. Should I still see a neurologist? Yes, absolutely. Cluster headache requires medical management by a neurologist or headache specialist. Acute attack treatments (high-flow oxygen, injectable or nasal triptans) and preventive medications (verapamil and others) are essential and evidence-based. Upper cervical care is at most an adjunctive piece of management.
7. What should I do during an acute attack? Use your acute attack plan from your headache specialist. High-flow oxygen by mask (typically 12-15 L/min for 15-20 minutes via a non-rebreather mask) and injectable or intranasal triptans are the gold-standard acute treatments. Chiropractic care has no role in acute attacks.
8. Will chiropractic care help during a cluster period? For some patients with a clear cervical and occipital component, upper cervical care may offer some adjunctive benefit between attacks during a cluster period, by reducing chronic cervical input to the trigeminocervical complex. It does not treat acute attacks.
9. How long does it take to see results? This varies enormously, and we set honest expectations: cluster headache is a severe, hypothalamically-driven condition, and adjunctive interventions like upper cervical care have limited and variable effects. Some patients with a strong cervical component may notice reduced background neck pain or muscle tension; significant impact on attack frequency or intensity, if it occurs, is generally a longer-term observation.
10. Are there triggers I should avoid? Yes. Alcohol is one of the most reliable triggers during cluster periods and is best avoided completely while in cluster. Altitude exposure can also trigger attacks. Disrupted sleep patterns can provoke clusters. Track your individual triggers in a diary.
11. Is there a genetic component to cluster headache? Yes — research has documented that first-degree relatives of cluster headache patients have a substantially elevated risk of developing the condition. Cluster headache has a clear familial pattern in some families, though most cases are sporadic.
12. What is the connection between cluster headache and the hypothalamus? Functional imaging consistently shows activation of the posterior hypothalamus during cluster attacks, and the remarkable circadian and circannual patterns of cluster headache reflect hypothalamic timing. The hypothalamus is considered the primary driver of cluster headache, which is why purely peripheral treatments cannot fully resolve it.
13. Are women affected by cluster headache? Yes. Historically cluster headache was thought to predominantly affect men, but a 2025 large-scale electronic health record analysis found that all four trigeminal autonomic cephalalgias, including cluster headache, showed higher prevalence in women — updating the long-held assumption of male predominance.
14. How will I know if upper cervical care is right for me? The only way to know is a thorough evaluation. We will assess whether your cluster headache picture includes a cervical and occipital component worth addressing, ensure you are receiving appropriate medical care, and give you an honest assessment. If we do not find evidence of a cervical contribution, we will tell you directly.
15. How do I get started? Call our Sarasota office at (941) 243-3729 or book your consultation online. We will review your history, perform a thorough examination, coordinate with your headache specialist, and give you an honest assessment of whether upper cervical care fits into your overall management.
Take the Next Step
Cluster headache is one of the most severe conditions in all of medicine, and the patients who carry it deserve aggressive, evidence-based medical management as their first priority. The high-flow oxygen, injectable triptans, and preventive medications guided by a neurologist or headache specialist are the foundation of cluster headache care — there is no responsible substitute for them.
For patients pursuing a multidisciplinary approach who are interested in evaluating the cervical contribution to their condition, upper cervical care may be a reasonable adjunctive consideration. The trigeminocervical complex at C1-C2 is genuinely part of the cluster headache pain mechanism, and the greater occipital nerve from C2 is a clinically relevant access point. We will be completely honest with you about the limits of what upper cervical care can offer and about the central importance of your medical management.
If you are in Sarasota, Bradenton, Lakewood Ranch, or anywhere in the surrounding region and you are living with cluster headache, Dr. Rusty Lavender and Dr. Jacob Temple at Lavender Family Chiropractic are here to give you an honest assessment of whether the upper cervical and occipital piece fits into your broader care strategy — and to be a thoughtful adjunctive part of your team.
📞 Call (941) 243-3729 today to schedule your complimentary consultation 📅 Book online here 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield