By Dr. Rusty Lavender
Dysautonomia: You stand up and your heart races. You feel lightheaded, sometimes to the point of nearly passing out. Your hands and feet are cold one moment and burning the next. Your stomach does not empty properly, your bladder either does not empty or empties too often, your body cannot regulate its temperature, and your sleep no longer restores you. You feel exhausted in a way that no rest fixes, and your nervous system seems to overreact to small stresses while underperforming on the things it should handle automatically. You have been to specialist after specialist — cardiologists, neurologists, gastroenterologists, endocrinologists — and your tests keep coming back essentially normal. And yet you know with absolute certainty that something is wrong.
What you are likely describing is dysautonomia — and one of the most important things to understand is that you are not alone, you are not imagining it, and the condition is genuinely real, biologically rooted, and worthy of serious care. Dysautonomia is an umbrella term for disorders of the autonomic nervous system, the part of your nervous system that runs everything you do not consciously think about: heart rate, blood pressure, digestion, breathing, temperature, sweating, bladder function, sexual function, and the moment-to-moment regulation that keeps your body in balance. When the autonomic nervous system malfunctions, the result is a constellation of symptoms that can affect nearly every organ system at once — which is exactly why dysautonomia is so commonly misdiagnosed and undertreated.
At Lavender Family Chiropractic in Sarasota, Florida, dysautonomia is one of the most important diagnostic categories we consider for the complex patients who find their way to our office. Many carry related diagnoses — POTS, ME/CFS, MCAS, long COVID, fibromyalgia, hypermobile Ehlers-Danlos syndrome — and many have never been formally evaluated for the broader autonomic dysfunction underlying their symptoms, nor for the upper cervical contribution that recent research has identified as a meaningful factor. This guide is for anyone in Sarasota, Bradenton, Lakewood Ranch, or the surrounding areas who is living with autonomic dysfunction — diagnosed or suspected — and who wants to understand the condition broadly and accurately, including where upper cervical chiropractic care honestly fits.
What Is Dysautonomia?
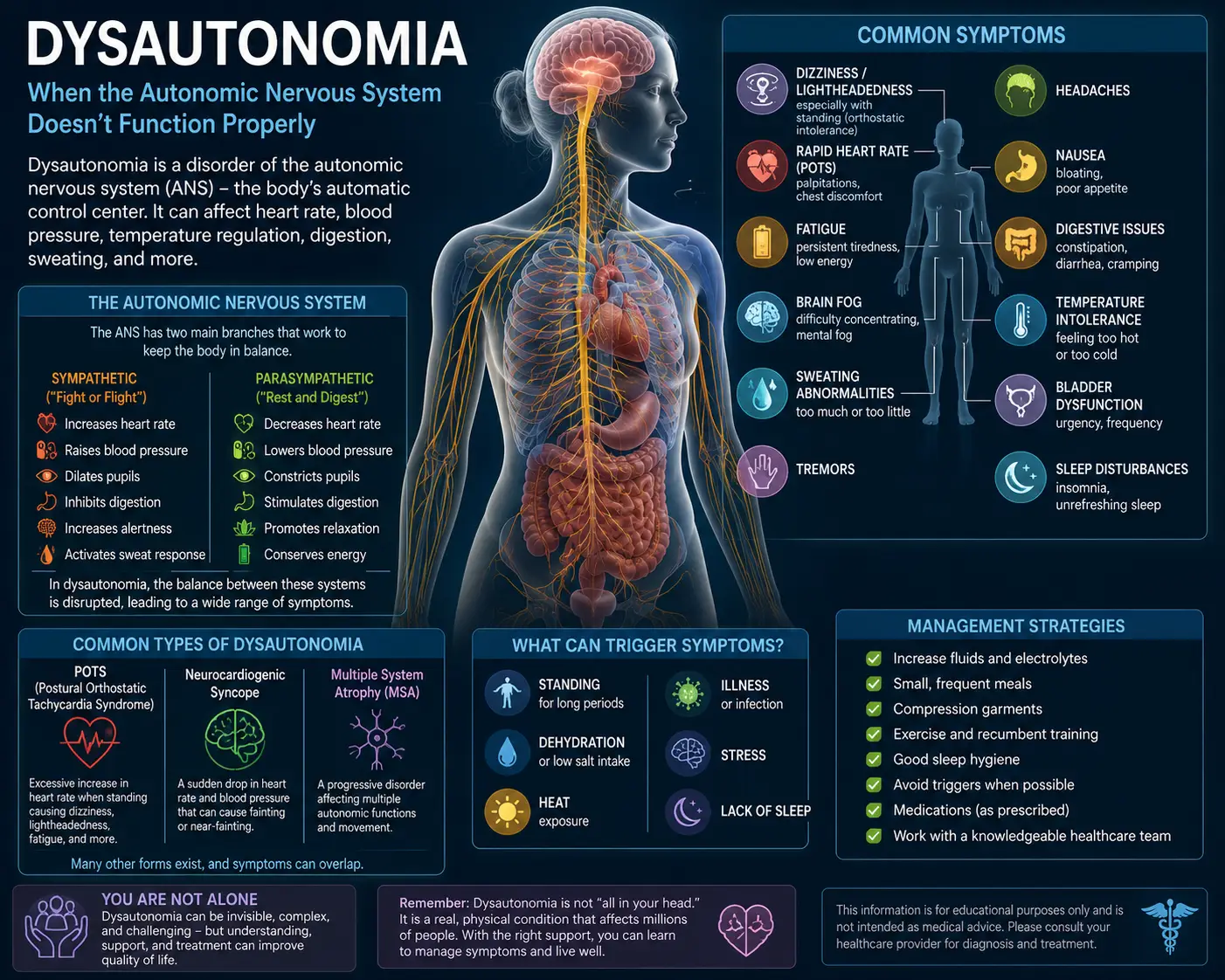
Dysautonomia is not a single disease. It is a broad term for a family of disorders that share a common feature: dysfunction of the autonomic nervous system. The autonomic nervous system controls the involuntary functions that keep you alive — heart rate, blood pressure, body temperature, digestion, breathing rate, kidney function, sexual function, bladder control, sweating, pupil response, and many more. When this system malfunctions, the symptoms can affect any of these functions, often several at once.
The autonomic nervous system has two main branches that normally work in balance. The sympathetic branch is your “fight or flight” system — it raises heart rate, raises blood pressure, dilates pupils, mobilizes energy, and prepares the body to respond to challenge or threat. The parasympathetic branch, mediated largely by the vagus nerve, is your “rest and digest” system — it lowers heart rate, supports digestion, promotes recovery, and maintains the calm, restorative state your body needs to heal and repair. Dysautonomia, in its many forms, involves dysfunction of one or both branches or an imbalance between them.
The condition can be primary (occurring on its own, with no other obvious cause) or secondary (developing as a consequence of another condition such as diabetes, autoimmune disease, infection, or trauma). It can affect any combination of organ systems, and it can range from mild and intermittent to severe and life-altering.
How common is dysautonomia? Far more common than its profile suggests. According to advocacy organizations and epidemiological estimates, approximately 70 million people worldwide are affected by disorders of the autonomic nervous system, with the actual figure likely far larger because dysautonomia frequently presents as a secondary component of high-prevalence neurological or autoimmune disorders, where the autonomic symptoms are often unrecognized or misattributed. This translates to a vast undiagnosed population — patients carrying autonomic dysfunction without ever receiving the diagnostic recognition or targeted care it warrants.
The diagnostic challenge is staggering. According to a patient-reported outcome study of 672 adults with various forms of dysautonomia, the average time from symptom onset to diagnosis was 7.7 years, with patients commonly cycling through cardiologists, neurologists, and primary care physicians before receiving accurate recognition. The same study identified the conditions most commonly accompanying dysautonomia: Ehlers-Danlos syndrome, mast cell disorders, vitamin deficiencies, fibromyalgia, and myalgic encephalomyelitis. This is the diagnostic cluster pattern many of our patients recognize themselves in.
Dysautonomia takes many forms, and understanding the major types matters for understanding where any treatment, including upper cervical care, can and cannot help.
The Major Forms of Dysautonomia
While dysautonomia includes more than a dozen recognized forms, several are particularly common and clinically important — and several connect directly to conditions we have addressed in depth.
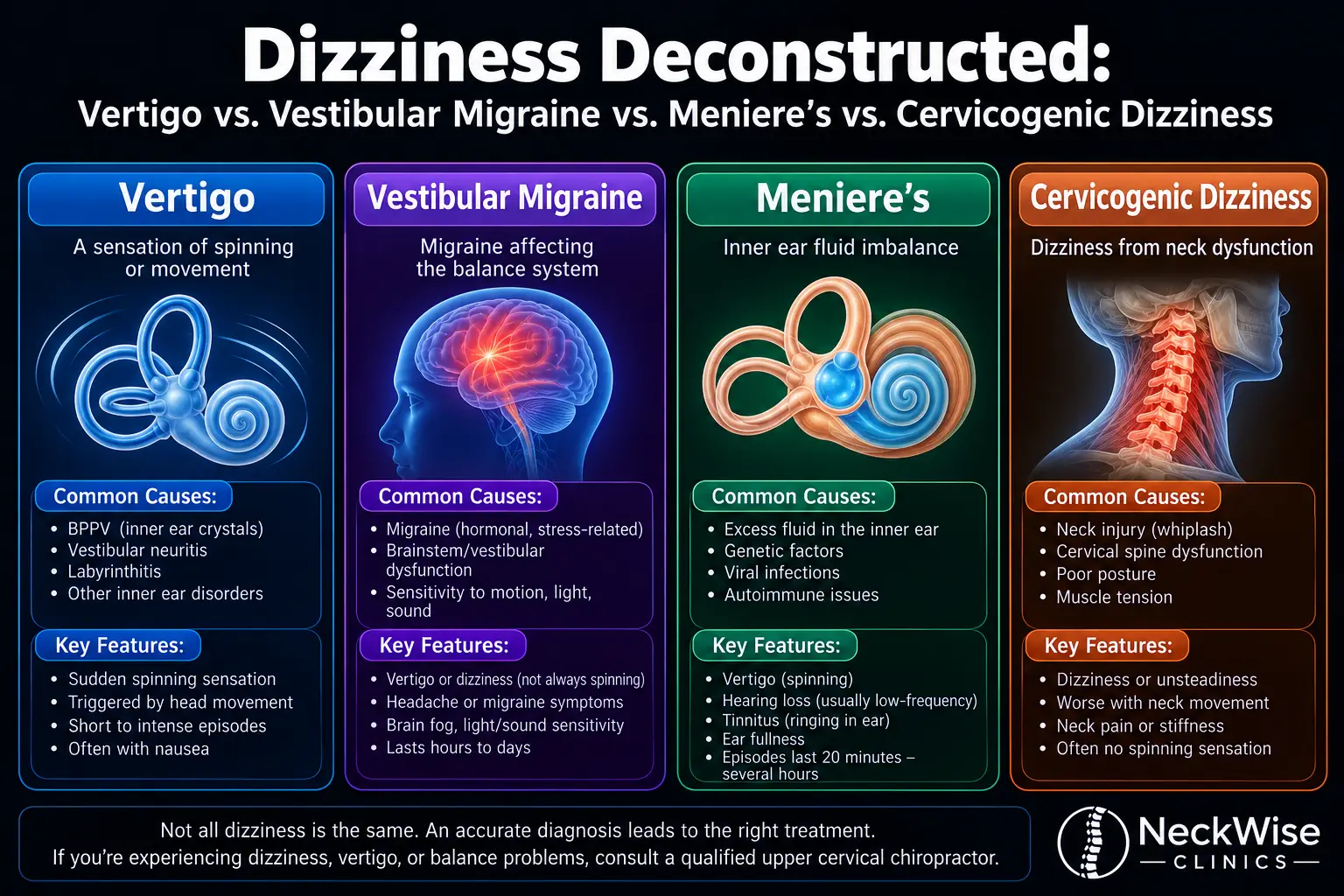
Postural orthostatic tachycardia syndrome (POTS) is one of the most common forms of dysautonomia, characterized by an abnormal heart rate increase upon standing accompanied by lightheadedness, fatigue, brain fog, and a constellation of other symptoms. POTS affects an estimated 1 to 3 million people in the United States, primarily young women, and overlaps substantially with ME/CFS, MCAS, and hypermobile Ehlers-Danlos syndrome. Our service page on POTSaddresses this condition in detail.
Neurocardiogenic syncope (also called vasovagal syncope) involves fainting or near-fainting from sudden drops in blood pressure and heart rate, often triggered by standing, emotional stress, pain, or other stimuli. It is one of the more common forms of dysautonomia and ranges from mild to severely disabling.
Vagus nerve dysfunction, addressed in detail on our vagus nerve dysfunction service page, involves impairment of the major nerve of the parasympathetic branch. Vagal dysfunction contributes to many of the conditions in the dysautonomia spectrum and is a central mechanism in long COVID, ME/CFS, and a number of other chronic illnesses.
Post-viral autonomic dysfunction, especially as documented in long COVID, has become one of the fastest-growing forms of dysautonomia. Estimates suggest dysautonomia is present in a substantial portion of long COVID patients — by some accounts approaching the majority of those with significant persistent symptoms. The post-infectious mechanism connecting viral illness to autonomic dysfunction is now extensively documented in the medical literature.
Pure autonomic failure (PAF) is a rare disorder characterized by degeneration of the autonomic nervous system, primarily affecting middle-aged and older adults and producing severe orthostatic hypotension. It is associated with conditions like Parkinson’s disease and dementia. PAF is a serious neurodegenerative condition that requires specialist medical management.
Multiple system atrophy (MSA) is another rare, progressive neurodegenerative disorder affecting the autonomic nervous system along with motor and other functions. It is a serious condition requiring specialist care and is not something chiropractic care can meaningfully address.
Diabetic autonomic neuropathy is a complication of diabetes affecting cardiovascular, gastrointestinal, and other autonomic functions. It is one of the most common secondary causes of dysautonomia and requires medical management of the underlying diabetes.
Familial dysautonomia and other inherited autonomic neuropathies are rare genetic conditions, typically presenting in childhood, that require specialist medical care.
This is just a partial list. Other forms include orthostatic hypotension, autonomic dysreflexia (in spinal cord injury), inflammatory autoimmune autonomic neuropathies, paraneoplastic autonomic dysfunction, and others. Each has different causes, different treatments, and different prognoses.
The reason this matters is honesty. Upper cervical chiropractic care is not a treatment for MSA, pure autonomic failure, diabetic autonomic neuropathy, familial dysautonomia, or the other primarily degenerative or systemic causes of dysautonomia — and we want to be completely clear about that. Where upper cervical care may be relevant is in the forms of dysautonomia where cervical input to the brainstem autonomic centers, vagal tone, and central autonomic regulation are part of the picture: POTS, post-infectious autonomic dysfunction, dysautonomia following neck trauma, and the autonomic component of conditions like ME/CFS and MCAS that we have addressed in detail.
The Brainstem, the Upper Cervical Spine, and the Autonomic Nervous System
To understand where upper cervical care fits into dysautonomia, you have to understand a piece of neuroanatomy that conventional autonomic workups rarely address.
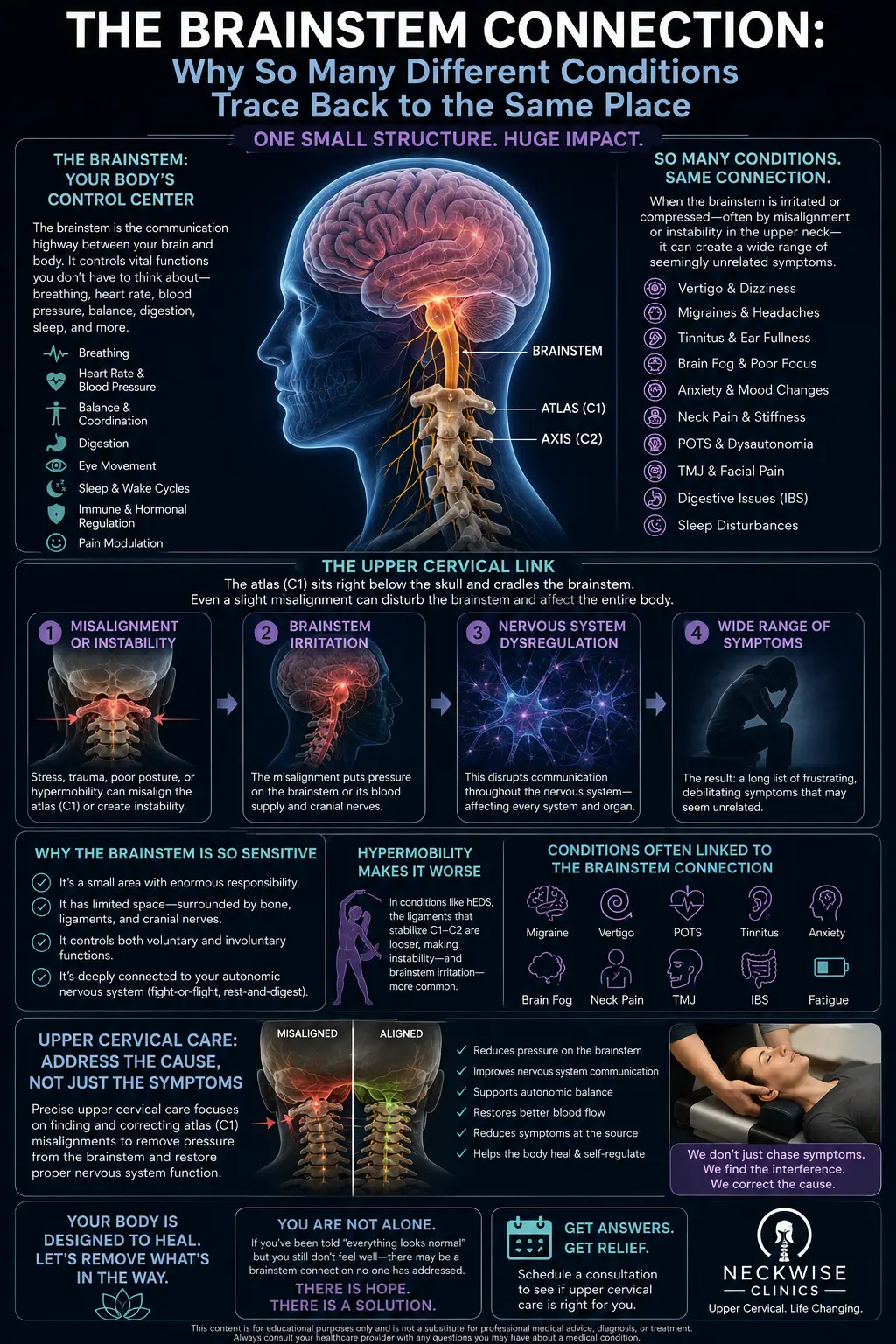
The autonomic nervous system does not run on autopilot from nowhere. It is centrally coordinated by a network of brain regions, with the brainstem — and specifically the medulla — serving as the primary site for moment-to-moment autonomic regulation. According to neuroscience references on autonomic control, the medulla oblongata is the primary site in the brain for regulating sympathetic and parasympathetic outflow to the heart and blood vessels, with the hypothalamus and higher centers modifying the activity of medullary centers, and the parasympathetic control of the heart primarily mediated by the vagus nerve, which originates in the brainstem at the medulla. This is the central command center for autonomic function.
Now here is the structural reality that makes the upper cervical connection more than a metaphor: the medulla sits directly behind and below the atlas (C1) and axis (C2) at the top of the cervical spine. The vagus nerve, which carries the majority of parasympathetic outflow to the body, exits the skull through the jugular foramen immediately adjacent to the atlas. The trigeminocervical complex — the brainstem region where head and neck sensory input converges — is housed in this same upper cervical region. In short, the upper cervical spine is the structural foundation for, and physical protector of, the entire autonomic command center.
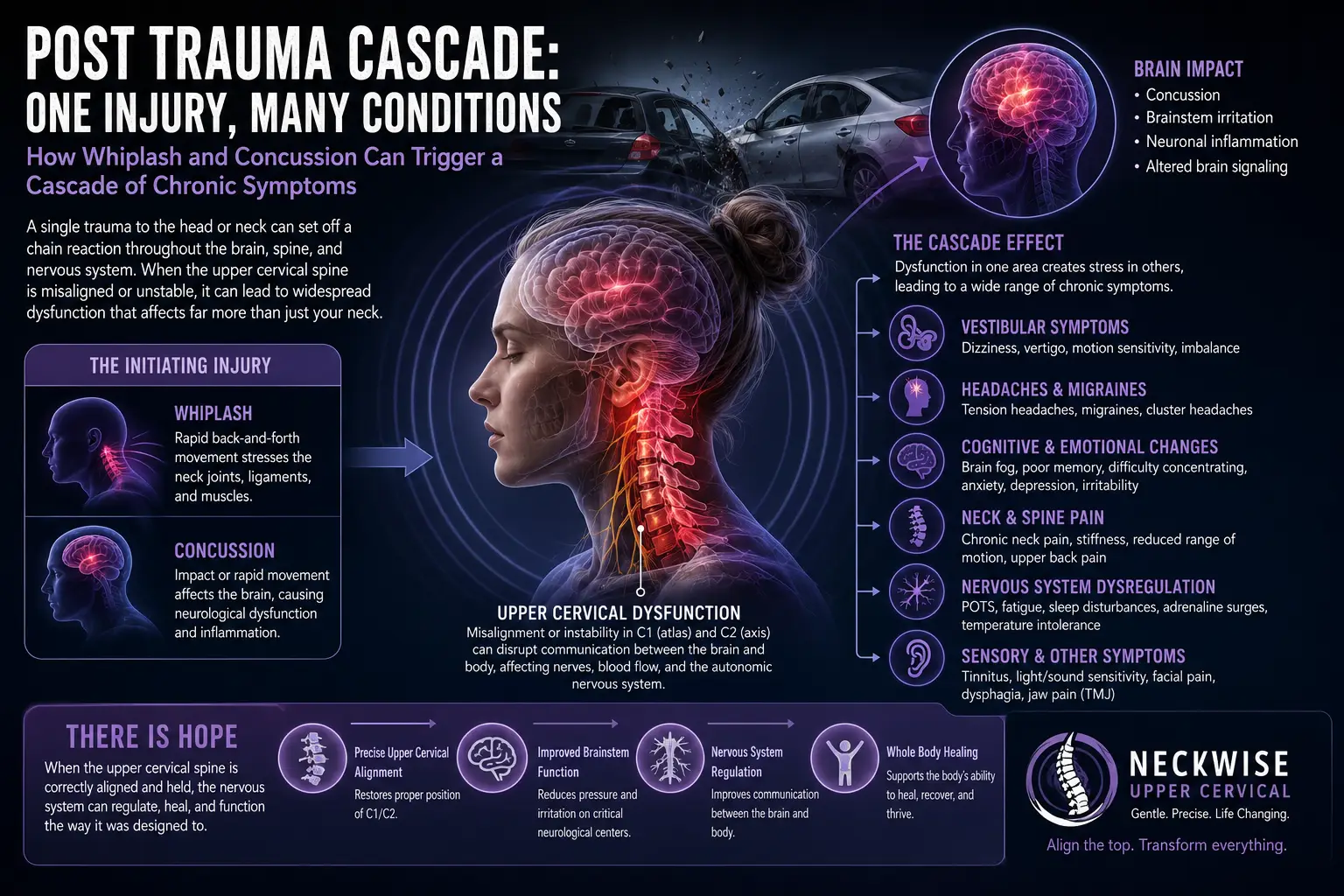
But the connection is not only structural. It is also functional. Direct experimental evidence has established that input from the upper cervical region influences brainstem autonomic control. According to a research study published in PMC, stimulating the second cervical nerve (C2) in a working heart brainstem preparation altered central respiratory drive and increased perfusion pressure, with sensory afferents from the upper cervical region projecting to the intermedius nucleus of the medulla and from there to brain regions involved in respiratory, cardiovascular, postural, and oro-facial behaviors — providing evidence of pathways linking upper cervical sensory afferents with central nervous system areas involved in autonomic control. The same study explicitly proposed that disruption of these pathways could explain the cardiorespiratory abnormalities that accompany whiplash and cervical dystonia.
This is direct, experimental evidence that upper cervical sensory input is wired into the brainstem autonomic control centers — and that disruption of this input has measurable effects on autonomic function. It is one of the strongest pieces of mechanistic evidence for the cervical contribution to autonomic dysfunction in the entire research literature.
What this means clinically: when the upper cervical spine is misaligned — from a fall, a car accident, sports injury, chronic postural strain, or other causes — the chronic abnormal sensory input from the upper cervical region can influence the brainstem autonomic control centers that govern heart rate, blood pressure, respiration, and autonomic balance. For patients whose dysautonomia involves brainstem and vagal dysfunction (which is much of the post-infectious and post-traumatic dysautonomia spectrum, and the autonomic component of conditions like ME/CFS, long COVID, and POTS), addressing the upper cervical contribution is targeting a real, biologically documented mechanism.
This is also why so many of our dysautonomia patients also have one of the conditions we have addressed in depth — POTS, ME/CFS, long COVID, MCAS, craniocervical instability. The shared mechanism — brainstem and vagal dysfunction in the upper cervical region — is the common thread.
Why Upper Cervical Care Matters for Selected Dysautonomia Patients
At Lavender Family Chiropractic, we use the Knee Chest Upper Cervical technique — a precise, gentle method of correcting atlas and axis misalignments without any twisting, popping, or forceful manipulation. For dysautonomia patients with a cervical or upper cervical component, this approach may help in several specific ways.
First, by correcting upper cervical misalignment, we reduce abnormal sensory input to the brainstem autonomic control centers — the very pathways the research has shown influence cardiovascular and respiratory regulation. Second, restoring proper upper cervical alignment supports vagal tone and parasympathetic function, helping shift the autonomic balance from the sympathetic-dominant state characteristic of so much chronic illness toward the “rest and digest” recovery state that supports healing. Third, for patients whose dysautonomia followed neck trauma, infection, or postural strain, addressing the upper cervical contribution targets a plausible mechanical contributor to the autonomic dysregulation.
The gentleness of the Knee Chest technique matters especially here. Dysautonomia patients often have nervous systems that are hypersensitive to physical input, with sympathetic-dominant states that can flare with aggressive manipulation. Our technique avoids forceful manipulation entirely, which makes it appropriate for the sensitive nervous systems characteristic of this patient population. We also pace care carefully, recognizing that many dysautonomia patients (especially those with concurrent ME/CFS or long COVID) tolerate slower, more spaced visits better than aggressive initial loading.
We need to be honest about candidacy and expectations. Upper cervical care is not a treatment for the degenerative or systemic forms of dysautonomia — MSA, PAF, diabetic autonomic neuropathy, genetic dysautonomias. We will tell you so directly if your situation falls into one of those categories. Where upper cervical care may meaningfully contribute is in the forms of dysautonomia involving brainstem and vagal dysfunction with cervical and postural components — and even there, dysautonomia is typically a multi-factor condition, and upper cervical care is best understood as one piece of a multidisciplinary approach rather than a stand-alone solution.
For most dysautonomia patients, the broader care team includes a cardiologist (often the primary specialist for POTS and orthostatic intolerance), a neurologist, possibly an autonomic specialist, and providers managing any underlying conditions (diabetes, autoimmune disease, etc.). We coordinate with these providers and see ourselves as a specialist piece of a broader strategy, never a substitute for proper medical management.
This is precisely the patient population our complex neurological conditions approach is designed for — patients whose symptoms cross multiple systems and whose diagnoses do not fit neatly into a single specialty’s framework.
What Care Looks Like at Lavender Family Chiropractic
If you come to our Sarasota office for evaluation related to dysautonomia, here is what to expect.
Your first visit begins with a thorough consultation. Dr. Lavender or Dr. Temple will sit down with you and carefully review your history — onset story (gradual, post-infectious, post-traumatic, other), symptom profile across the autonomic spectrum (cardiovascular, gastrointestinal, temperature, sweating, bladder, sleep, etc.), any specific dysautonomia diagnosis you carry, comorbid conditions (POTS, ME/CFS, MCAS, EDS, long COVID, fibromyalgia, others), your medications, what other providers have told you, and your activity tolerance. We pay particular attention to whether your dysautonomia onset suggests a cervical or upper cervical contribution — post-traumatic patterns, post-infectious patterns following neck-region inflammation, or postural strain histories.
The examination is adapted for this patient population. We use advanced 3D imaging to visualize your upper cervical alignment with sub-millimeter precision, autonomic function testing to objectively measure your nervous system state, postural and gait analysis, and a careful neurological examination. For patients with concurrent POTS or orthostatic intolerance, we incorporate orthostatic assessment. For patients with severe post-exertional malaise from concurrent ME/CFS, we structure visits to avoid triggering crashes.
If the examination reveals upper cervical findings consistent with someone whose dysautonomia may benefit from care, we will explain our recommendations openly. We will also be honest about cases where your dysautonomia is unlikely to respond to upper cervical care — and we will direct you toward more appropriate care when that is what your situation calls for.
Care is delivered through the gentle Knee Chest Upper Cervical technique. We offer customized treatment plans tailored to your specific situation, with transparent timelines and honest expectations.
📞 Call (941) 243-3729 to schedule your complimentary consultation 📅 Book your consultation online 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
What the Research Says About Dysautonomia and the Upper Cervical Connection
The research on dysautonomia is broad and growing, and the autonomic neuroscience connecting it to the upper cervical region is well established.
The scope of dysautonomia is well documented. Epidemiological analyses estimate that approximately 70 million people worldwide are affected by disorders of the autonomic nervous system, with the actual figure likely far larger because dysautonomia frequently presents as a secondary component of high-prevalence neurological or autoimmune disorders where the autonomic symptoms are commonly unrecognized or misattributed — establishing dysautonomia as a major and substantially undiagnosed public health condition.
The diagnostic challenge is documented in patient-reported research. A study of 672 adults with various forms of dysautonomia found that the average time from symptom onset to diagnosis was 7.7 years, with diagnosis typically made by cardiologists, neurologists, and primary care physicians, and that common comorbid conditions included Ehlers-Danlos syndrome, mast cell disorders, vitamin deficiencies, fibromyalgia, and myalgic encephalomyelitis — confirming both the severity of diagnostic delays and the cluster pattern of comorbid conditions familiar to so many dysautonomia patients.
The central neuroscience of autonomic control is well established. According to clinical references on autonomic regulation, the medulla oblongata is the primary site in the brain for regulating sympathetic and parasympathetic outflow, with the hypothalamus and higher centers modifying medullary activity, and parasympathetic control of the heart primarily mediated by the vagus nerve, which originates in the brainstem at the medulla — placing the brainstem at the structural and functional center of autonomic function.
The direct experimental evidence connecting upper cervical input to brainstem autonomic control is striking. A research study published in PMC documented that stimulating the second cervical nerve in a working heart brainstem preparation altered central respiratory drive and increased perfusion pressure, with sensory afferents from the upper cervical region projecting to the intermedius nucleus of the medulla and to brain regions involved in respiratory, cardiovascular, postural, and oro-facial behaviors, and explicitly proposed that disruption of these pathways could explain the cardiorespiratory abnormalities that accompany whiplash and cervical dystonia. This is direct experimental confirmation that upper cervical input is wired into the brainstem autonomic control system.
The post-infectious connection has been particularly well documented for the COVID-19 era. Estimates suggest that dysautonomia is present in approximately 70% of patients with persistent long COVID symptoms, with the autonomic, vagal, and brainstem mechanisms thoroughly documented in the research we reviewed in detail on our long COVID blog.
This body of research establishes that dysautonomia is enormous in scope, frequently undiagnosed, multi-factorial in cause, brainstem-coordinated in function, and — for the subset of patients with cervical input contributing — directly influenced by upper cervical sensory pathways to the brainstem autonomic centers. The cervical contribution is biologically real, experimentally documented, and clinically meaningful for selected patients.
Lifestyle Factors That Support Dysautonomia Management
Because dysautonomia is so multi-factorial and because the autonomic nervous system is so responsive to daily inputs, lifestyle factors are central to management for most patients.
Hydration and salt. For most forms of dysautonomia involving orthostatic intolerance or blood volume issues, increased water and salt intake is a foundational intervention. Many specialists recommend significant daily water intake and added salt under appropriate medical guidance. The Florida climate makes hydration especially important.
Pacing and activity management. Many dysautonomia patients, especially those with concurrent ME/CFS or long COVID, do best with carefully paced activity that stays within their energy envelope. Aggressive exercise programs frequently backfire; gentle, gradually progressed activity tends to work better.
Compression garments. Waist-high compression garments are one of the most effective non-medication interventions for POTS and other orthostatic dysautonomia, reducing blood pooling in the lower body when upright.
Vagal tone work. Practices that support parasympathetic function — slow diaphragmatic breathing with longer exhales, humming, gargling, gentle cold exposure to the face, meditation, time in nature — are genuinely supportive for dysautonomia involving vagal dysfunction.
Sleep regulation. The autonomic nervous system depends on consistent, restorative sleep. Regular sleep and wake times, dark and cool environment, and good sleep hygiene support autonomic regulation directly.
Stress management. Chronic stress drives sympathetic dominance, which worsens nearly every form of dysautonomia. Practices that down-regulate stress responses — therapy, meditation, supportive relationships — are not optional add-ons; they are core management.
Anti-inflammatory nutrition. Because inflammation contributes to autonomic dysregulation, an anti-inflammatory eating pattern (whole foods, omega-3-rich fish, minimizing processed foods and refined sugars) supports overall autonomic function.
Avoid prolonged standing during flares. For patients with orthostatic intolerance, prolonged still standing is one of the worst provocateurs. Frequent movement, leg crossing, calf pumping, or sitting when possible can prevent symptoms.
Manage underlying conditions. For secondary dysautonomia from diabetes, autoimmune disease, or other systemic conditions, managing the underlying condition is essential. Continue working with the specialists who manage these.
Connect with the community. Patient organizations like Dysautonomia International provide resources, community, and advocacy that genuinely help patients navigate this complex diagnostic territory.
If you found this guide useful, you may also want to read our blogs on ME/CFS, long COVID, and MCAS — all conditions that involve significant autonomic dysfunction and share many of the brainstem and vagal mechanisms we work with here.
Serving Sarasota and the Surrounding Communities
Lavender Family Chiropractic is located in Sarasota, Florida, at 5899 Whitfield Avenue, Suite 107 — at the corner of University and Whitfield. From this central location, we serve patients throughout the region, including Bradenton, Lakewood Ranch, Palmetto, Parrish, Venice, Osprey, Nokomis, Ellenton, Ruskin, Myakka City, North Port, and the greater Tampa Bay area. Patients also travel from St. Pete, Riverview, and Manatee County to receive specialized upper cervical care here.
Dysautonomia is the diagnostic territory where many of our most complex patients land — patients with multiple overlapping diagnoses, long histories of being dismissed or misdiagnosed, and a deep need for a provider who understands the integrated picture. We recognize that travel can be difficult for dysautonomia patients, and we structure care schedules to accommodate energy and orthostatic limitations. If you have been searching for a provider who understands the autonomic and upper cervical mechanisms and will work within your real-world limits, we encourage you to reach out.
Top 15 FAQs About Dysautonomia and Upper Cervical Chiropractic Care
1. What is dysautonomia? Dysautonomia is an umbrella term for disorders involving dysfunction of the autonomic nervous system — the system that controls heart rate, blood pressure, digestion, temperature, sweating, breathing rate, and other involuntary functions. It includes many specific conditions and affects an estimated 70 million people worldwide.
2. How is dysautonomia diagnosed? Diagnosis typically involves a combination of clinical history, physical examination, and specialized testing such as tilt-table testing, autonomic function testing, heart rate variability assessment, and tests specific to the suspected subtype. The average time from symptom onset to diagnosis is reported to be approximately 7.7 years, reflecting how often the condition is missed or misattributed.
3. Can upper cervical chiropractic cure dysautonomia? No. Dysautonomia is a multifactorial condition with many causes, and no single treatment cures it. What upper cervical care can do is address the cervical input to brainstem autonomic control centers — a documented contributor to autonomic dysfunction in selected patients — as one part of a multidisciplinary approach.
4. Which forms of dysautonomia might upper cervical care help? The forms involving brainstem and vagal dysfunction with cervical or postural contributions, such as POTS, post-infectious autonomic dysfunction (including long COVID), dysautonomia following neck trauma, and the autonomic components of ME/CFS, MCAS, and craniocervical instability. We are honest that genetic, neurodegenerative, and systemic forms (like MSA, PAF, diabetic autonomic neuropathy) are not addressed by upper cervical care.
5. Why is the upper cervical spine connected to autonomic function? Because the brainstem — the primary central regulator of autonomic function — sits directly behind and below the atlas and axis. Direct experimental research has shown that upper cervical sensory input projects to brainstem autonomic centers and alters cardiovascular and respiratory regulation. The vagus nerve, the major parasympathetic nerve, also exits the skull immediately adjacent to the atlas.
6. Is upper cervical care safe for dysautonomia patients? The Knee Chest Upper Cervical technique is exceptionally gentle, with no twisting or forceful manipulation. It is generally well tolerated by the sensitive nervous systems of dysautonomia patients. We pace care carefully and screen for red flags.
7. Do I still need a cardiologist or neurologist? Yes. Dysautonomia is a complex multidisciplinary condition, and most patients benefit from involvement of a cardiologist, neurologist, or autonomic specialist as the primary medical manager. Upper cervical care is best understood as a specialist adjunctive piece of a broader strategy.
8. What is the connection between dysautonomia and conditions like POTS, ME/CFS, MCAS, and long COVID?These conditions all involve significant autonomic dysfunction as a core feature. They overlap substantially in patient populations, share many mechanisms (brainstem dysregulation, vagal dysfunction, central sensitization), and often coexist in the same patients. They are different presentations of overlapping autonomic and neuroinflammatory mechanisms.
9. Why did it take so long to get my diagnosis? Because dysautonomia symptoms affect multiple organ systems, standard testing often appears normal, and few clinicians are trained specifically in autonomic medicine. The 7.7-year average delay is a real and frustrating feature of this diagnostic territory. You are not imagining it, and you were not exaggerating.
10. How long does it take to see results from upper cervical care? This varies by patient and by how much of the dysautonomia is driven by cervical and upper cervical factors. Some patients notice subtle changes in orthostatic tolerance, heart rate variability, or sleep within weeks. Others experience more gradual improvement over months. We give honest timelines based on your examination findings.
11. Can a car accident cause dysautonomia? Yes. Cervical trauma, including whiplash, can disrupt the upper cervical pathways that input to brainstem autonomic centers, and post-traumatic dysautonomia is a recognized clinical pattern. The 2015 research on upper cervical afferent input to autonomic centers explicitly proposed this mechanism for the cardiorespiratory abnormalities seen after whiplash.
12. Will I need to stop my medications? No. Continue all medications as prescribed by your treating physicians. Upper cervical care is complementary, not a replacement. If your medical team eventually adjusts your regimen based on clinical improvement, that is a discussion for you and them.
13. Can stress make dysautonomia worse? Yes, significantly. Chronic stress drives sympathetic dominance, which is one of the core problems in most forms of dysautonomia. Stress management is genuinely central to overall management, not an afterthought.
14. How will I know if upper cervical care is right for me? The only way to know is a thorough evaluation. We will assess whether your dysautonomia has a cervical and upper cervical component, screen for red flags, and give you an honest assessment of whether upper cervical care is likely to help — and what else you may need.
15. How do I get started? Call our Sarasota office at (941) 243-3729 or book your consultation online. We will review your full history, perform a thorough examination, coordinate with your medical team, and give you an honest assessment of how upper cervical care fits into your overall management.
Take the Next Step
Dysautonomia is one of the most under-recognized and most clinically important diagnostic territories in modern medicine — an umbrella that covers tens of millions of people worldwide, the vast majority of whom never receive accurate recognition. Whether your specific diagnosis is POTS, neurocardiogenic syncope, post-COVID autonomic dysfunction, the autonomic component of ME/CFS or MCAS, or something else in this complex family, you deserve providers who take the integrated picture seriously and who understand the mechanisms — including the upper cervical and brainstem mechanisms — that connect so many of these conditions.
If you are in Sarasota, Bradenton, Lakewood Ranch, or anywhere in the surrounding region and you are living with dysautonomia — diagnosed or suspected — Dr. Rusty Lavender and Dr. Jacob Temple at Lavender Family Chiropractic are here to give you an honest evaluation of whether the upper cervical piece is part of your picture, and to coordinate with the broader medical team that should be part of managing this condition.
📞 Call (941) 243-3729 today to schedule your complimentary consultation 📅 Book online here 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield