Whiplash-Associated Vertigo: If you’ve been in a car accident, taken a hard fall, suffered a sports collision, or experienced any other event that snapped your head and neck violently — and now you’re dealing with dizziness, imbalance, brain fog, and a sense of being “off” that won’t go away — there’s a strong chance you’re experiencing whiplash-associated vertigo.
This condition is alarmingly common and almost universally undertreated. Research shows that 20 to 58 percent of patients who experience whiplash injuries develop late-onset dizziness, vertigo, or disequilibrium — sometimes immediately, but often weeks or months after the original event. Many of these patients have already had their imaging come back “normal,” been told their neck looks fine, and been left wondering why they still feel so wrong.
Here in Sarasota, Florida, where car accidents on I-75, US-41, and the busy seasonal traffic patterns produce a steady stream of whiplash injuries, we see this condition often. At Lavender Family Chiropractic, located at 5899 Whitfield Avenue, Suite 107 at the corner of University and Whitfield, Dr. Rusty Lavender and Dr. Jacob Temple specialize in helping whiplash patients address one of the most overlooked but most clinically significant drivers of their lingering symptoms: dysfunction in the upper cervical spine. This blog will walk you through exactly what whiplash-associated vertigo is, why standard imaging usually misses it, what current research shows, and how upper cervical chiropractic care fits into a complete recovery plan.
This article is part of our broader vertigo resource hub. For the full picture of how we approach dizziness as a whole, we recommend starting with our main page on vertigo care in Sarasota with Dr. Jacob Temple.
What Is Whiplash-Associated Vertigo?
Whiplash-associated vertigo is dizziness, imbalance, or vestibular dysfunction that develops as a result of a whiplash injury — the rapid, forceful back-and-forth motion of the neck that occurs in car accidents (especially rear-end collisions), falls, sports impacts, physical assaults, and other sudden-force events. The condition is part of a broader category clinicians call Whiplash-Associated Disorders (WAD), which includes neck pain, headaches, cognitive symptoms, sleep disturbance, and yes — dizziness.
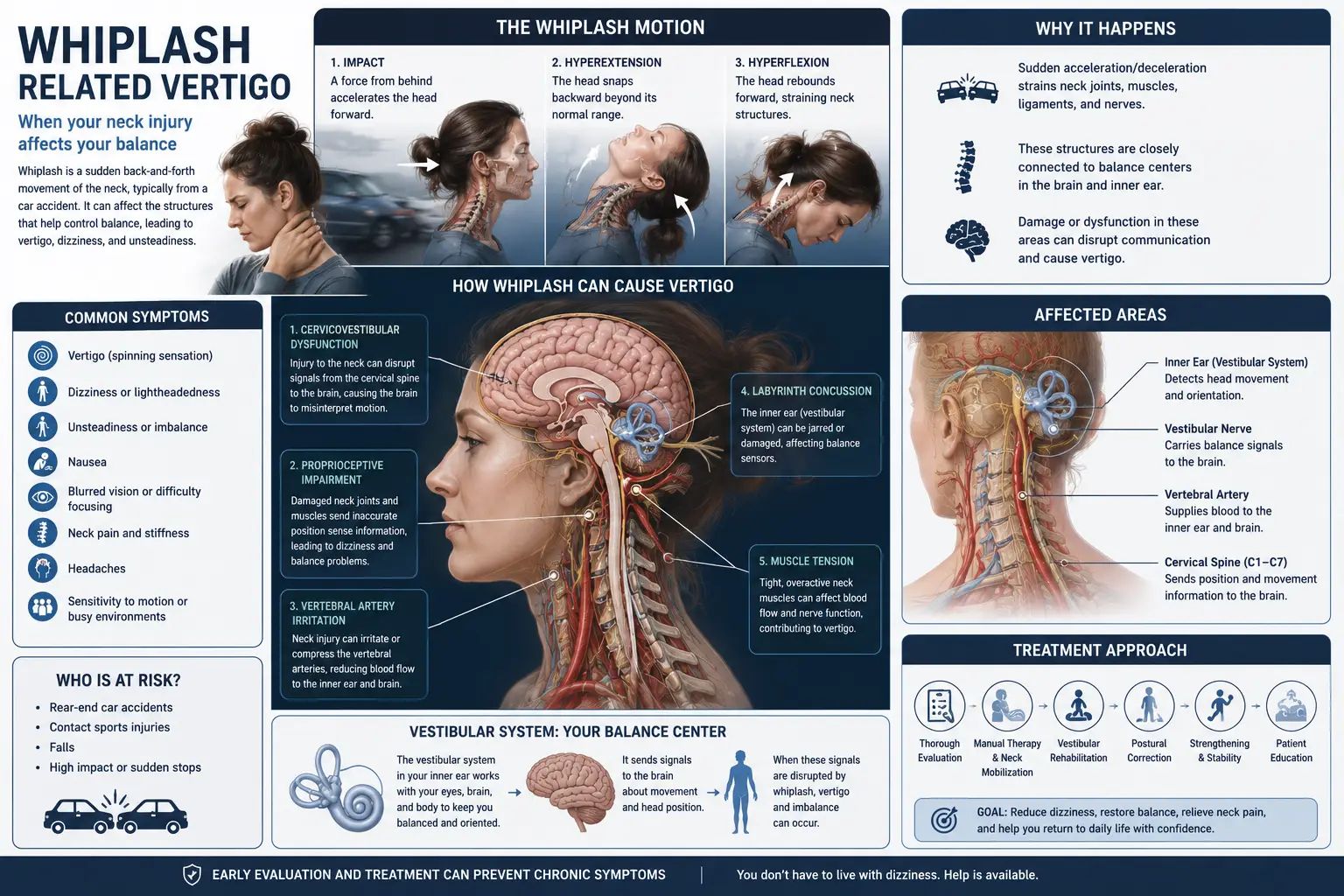
Whiplash injuries can produce dizziness through several mechanisms:
Cervical proprioceptive dysfunction. This is the most common and most overlooked driver. The upper cervical spine (C1–C3) contains roughly 50 percent of all the proprioceptive receptors in the cervical spine — sensors that tell your brain where your head is in space. Whiplash damages these sensors, producing faulty positional signals that the brain interprets as dizziness, imbalance, and disorientation.
Direct vestibular injury. The same forces that injure the neck can transmit through the skull to the inner ear, dislodging calcium crystals (causing post-traumatic BPPV), damaging vestibular hair cells, or disrupting vestibular nerve function.
Concomitant concussion. Many whiplash injuries also produce a concussion — even in cases where the head never struck anything. The rapid acceleration-deceleration is enough to shake the brain inside the skull. When concussion and whiplash occur together, dizziness becomes particularly persistent.
Autonomic dysregulation. Whiplash injuries can affect the vagus nerve and sympathetic chain in the upper neck, producing dizziness on standing, exercise intolerance, and the foggy, dysregulated feeling many WAD patients describe.
Vertebrobasilar involvement. In some cases, whiplash can affect the vertebral arteries that pass through the upper cervical spine, producing positional dizziness when the head is moved or held in certain positions.
Common symptoms of whiplash-associated vertigo include:
- Dizziness, lightheadedness, or a sense of floating
- Imbalance or unsteadiness, especially when walking or turning
- Disorientation in busy visual environments
- Headaches, especially at the base of the skull
- Neck pain and stiffness
- Brain fog and difficulty concentrating
- Fatigue and sleep disruption
- Sensitivity to light and sound
- Motion sensitivity (cars, scrolling, screens)
- Ringing in the ears (tinnitus)
- Visual disturbances or trouble focusing
- Anxiety or mood changes
- Difficulty returning to driving or normal activities
One of the most frustrating features of whiplash-associated vertigo is that standard imaging usually shows nothing. X-rays, CT scans, and MRIs are designed to identify fractures, disc herniations, and structural abnormalities — not the proprioceptive dysfunction, ligament strain, and joint instability that drive most WAD-related dizziness. This is why so many patients are told there’s “nothing wrong” even when something is clearly very wrong.
How a Whiplash Injury Affects Your Nervous System, Cervical Spine, and Balance System
To understand why whiplash produces such persistent dizziness — and why the upper cervical spine plays such a central role — you have to look at exactly what happens during a whiplash event.
When a force suddenly accelerates or decelerates your head, the neck whips through a violent range of motion in a fraction of a second. According to research from the National Institute of Neurological Disorders and Stroke (NINDS), this motion injures multiple structures simultaneously:
1. The Upper Cervical Ligaments. The ligaments that stabilize your atlas and axis — including the alar ligaments and transverse ligament — can be stretched or partially torn. These ligaments don’t always heal perfectly, leading to subtle long-term instability.
2. The Cervical Facet Joints. The small joints between vertebrae, particularly in the upper cervical spine, can sustain injury that doesn’t show on standard imaging but produces persistent dysfunction and faulty signaling.
3. The Deep Cervical Muscles. The suboccipital muscles and deep cervical flexors — small but critical muscles for posture, head control, and proprioception — are often damaged in whiplash and develop chronic dysfunction.
4. The Cervical Proprioceptors. This is the key. The upper cervical spine houses an extraordinary density of position-sensing mechanoreceptors, and whiplash damages them in ways that produce long-term dizziness. A landmark 1997 study by Loudon et al. in the journal Spine demonstrated that whiplash patients have measurably impaired ability to reproduce head position accurately — a direct sign of proprioceptive dysfunction.
5. The Vestibular System. The forces of whiplash can also dislodge inner ear crystals and damage the vestibular apparatus directly, producing classic BPPV or other vestibular dysfunction alongside the cervical injury.
6. The Autonomic Nervous System. Research by Sterling et al. published in the journal Pain in 2003 showed that whiplash produces measurable motor system dysfunction and autonomic disturbance that persists long after the acute injury, contributing to the chronic, multisystem nature of WAD.
Here’s why all of this matters so much for dizziness: your balance depends on the brain integrating three sensory inputs — vestibular (inner ear), visual (eyes), and proprioceptive (especially from the neck). Whiplash often damages two of those three simultaneously: the vestibular input and the proprioceptive input. Your brain is now trying to maintain balance with two unreliable inputs at once, and the result is exactly what whiplash patients describe — persistent dizziness, imbalance, fog, and a sense of being “not yourself.”
The longer this dysfunction persists, the more entrenched it becomes in the nervous system. This is why early evaluation and care matter so much — and why whiplash injuries should never be dismissed, even if you “feel okay” in the first few days.
Why the Upper Cervical Spine Is the Epicenter of Whiplash-Associated Vertigo
The research on this is striking, and it has shifted dramatically over the past two decades. Here’s the bottom line: post-traumatic dizziness following whiplash is primarily a cervical spine problem, not a vestibular problem — even when the inner ear has been affected.
A landmark 2025 review published in Frontiers in Neurology analyzed the connection between cervicogenic dizziness and whiplash-associated disorders. The authors concluded that in cases of dizziness following whiplash, “post-traumatic dizziness seems to be primarily related to the cervical spine rather than a concussion affecting the vestibular system.” They further confirmed that lack of improvement in cervical spine parameters correlates with persistent dizziness in chronic WAD patients.
The 2025 review also confirmed the work of Treleaven et al., who demonstrated that the cervical spine is the primary driver of chronic WAD-related dizziness — meaning that addressing the neck is not just helpful, but essential, for resolving the dizziness.
A 2025 systematic review and meta-analysis published in BMC Musculoskeletal Disorders and indexed in PubMed examined the effectiveness of manual therapy for cervical dizziness across multiple randomized controlled trials. The authors found that manual therapy produced significant reductions in dizziness intensity and improvements in quality of life compared to control groups.
Why is the upper cervical spine specifically so important?
Density of proprioceptors. As noted, the C1–C3 region contains roughly 50 percent of all cervical proprioceptive receptors. Damage here produces disproportionately large effects on balance signaling.
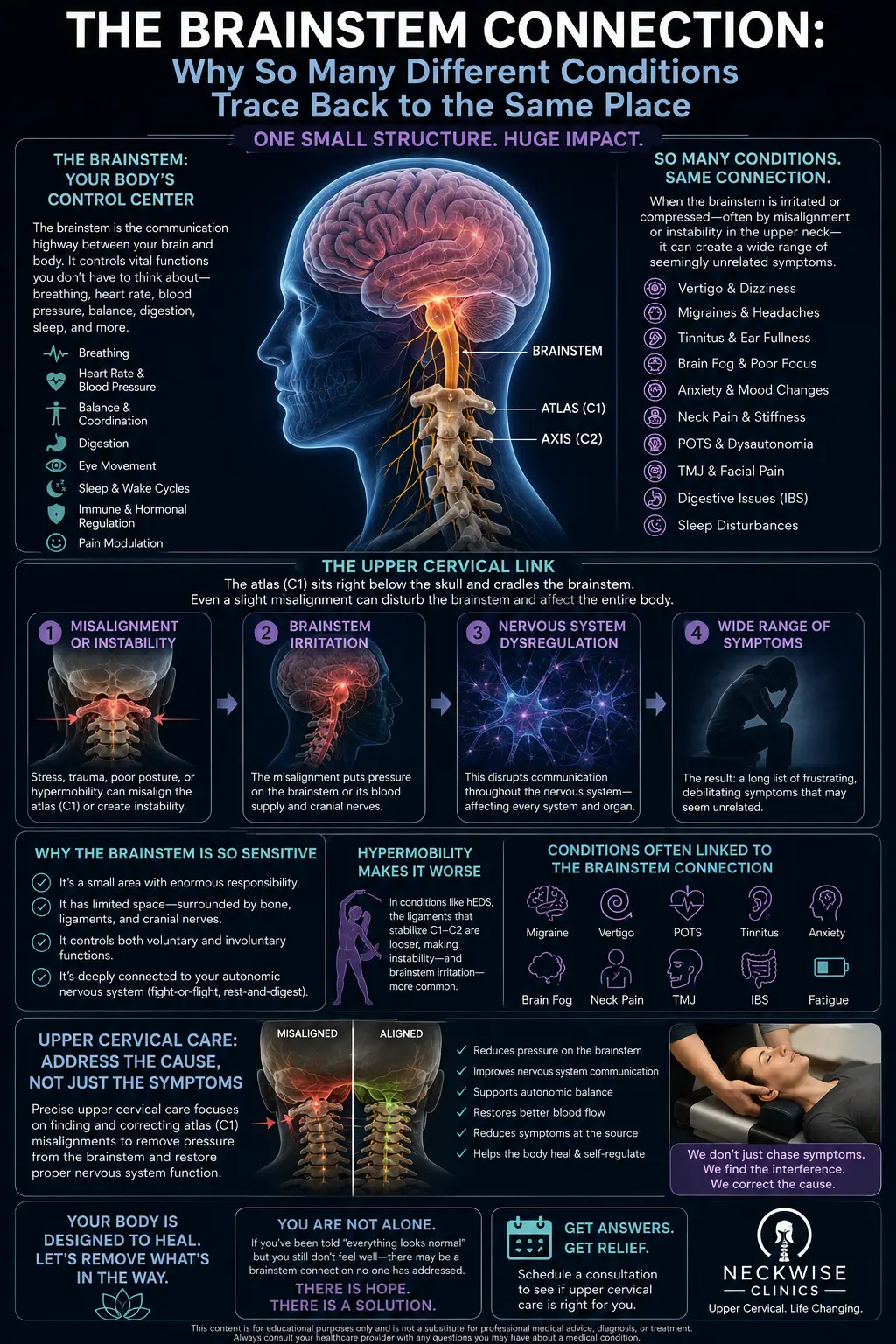
Direct connection to the brainstem. The upper cervical spine sits adjacent to the brainstem, the cerebellum, and the vestibular nuclei — the very structures that integrate balance information. Faulty signals from C1 and C2 directly disrupt these centers.
Mechanical vulnerability. The upper cervical region absorbs the brunt of whiplash forces because the head, balancing on top of the long lever of the neck, generates extreme torque at the skull-neck junction.
Ligamentous involvement. The alar and transverse ligaments at the upper cervical spine are critical for stabilizing the head, and whiplash often strains them in ways that don’t heal completely without targeted intervention.
This is also where the importance of gentle, precise upper cervical correction becomes clear. Forceful manipulation of an already-injured upper cervical spine can worsen ligamentous instability and produce setbacks. The upper cervical chiropractic approach — calculated from imaging, delivered with light pressure, with no twisting or popping — is fundamentally different from general chiropractic and far better suited to whiplash recovery.
Upper Cervical Chiropractic Care for Whiplash-Associated Vertigo: What to Expect
At Lavender Family Chiropractic, we approach whiplash recovery in a careful, deliberate, and gentle way. Many of our whiplash patients have been struggling for months or years and have already seen multiple providers — chiropractors, physical therapists, ENTs, neurologists, primary care doctors. We treat that history with the seriousness it deserves and collaborate with your other care providers whenever appropriate.
Here’s what your journey looks like at our Sarasota office.
Step One: Comprehensive Consultation
Your first visit starts with a real conversation. Dr. Lavender or Dr. Temple will sit down with you and learn the full story — when and how the whiplash happened, the exact mechanism of injury, what symptoms you experienced initially, what symptoms remain, what care you’ve received, and what’s helped versus what hasn’t. We pay particular attention to mechanism of injury (rear-end collision, side-impact crash, sports impact, fall, etc.) because this often reveals exactly how the upper cervical spine was likely injured.
Step Two: 3D CBCT Imaging and Neurological Scanning
Next, we use 3D CBCT X-ray technology to take precise three-dimensional images of your upper cervical spine. This advanced imaging shows us — down to the millimeter — exactly how your atlas (C1) and axis (C2) are positioned. For whiplash patients especially, this precision matters. Standard X-rays and MRIs typically miss the subtle misalignments that drive whiplash-associated vertigo. CBCT is far more sensitive for the upper cervical region.
We pair this with paraspinal infrared thermography, which assesses nervous system function along your spine. For whiplash patients, thermography is particularly useful because it reveals patterns of autonomic stress and nervous system dysfunction that correspond to the persistent symptoms — fatigue, brain fog, dizziness, light sensitivity.
Step Three: A Gentle, Specific Correction — No Twisting or Cracking
When you receive your upper cervical correction, you’ll likely be surprised at how gentle it is. There is no twisting, popping, cracking, or high-velocity thrust. We use the Advanced HIO Knee Chest Upper Cervical Technique (AHKC), one of the gentlest and most precise methods of upper cervical correction available.
This matters enormously for whiplash patients. The upper cervical ligaments may be partially strained from the injury, and aggressive manipulation can make things worse. Our gentle, imaging-guided approach respects the injured tissue while still producing the precise correction needed for recovery.
Step Four: Monitoring and Stabilizing Your Recovery
The goal of upper cervical care isn’t to adjust you repeatedly forever. The goal is to help your spine hold its corrected position so your nervous system can finally complete the recovery work that’s been stalled since the injury. We track your progress visit by visit and adjust your care plan as you stabilize.
Most whiplash patients begin noticing meaningful changes within the first few weeks: clearer thinking, less dizziness, fewer headaches, better neck mobility, improved sleep, reduced motion sensitivity, and the gradual return of confidence in everyday activities. Recovery from chronic WAD is often gradual — research suggests 6 to 12 weeks of consistent care for significant improvement — but the trajectory is almost always positive when the upper cervical piece is addressed.
Have you been dealing with dizziness, brain fog, or imbalance since your whiplash injury? Call us at (941) 243-3729 or book a complimentary consultation online. We’ll help you figure out whether upper cervical care is the missing piece in your recovery.
What the Research Says About Whiplash-Associated Vertigo
The medical literature on whiplash-associated dizziness has expanded significantly in recent years. Here are the most relevant findings.
A 2025 review published in Frontiers in Neurology concluded that post-traumatic dizziness following whiplash is primarily related to the cervical spine rather than vestibular dysfunction, and that lack of improvement in cervical spine parameters correlates with persistent dizziness in chronic whiplash-associated disorder patients. The authors emphasized that addressing the cervical component is essential for resolution.
A 2025 systematic review and meta-analysis published in BMC Musculoskeletal Disorders and indexed in PubMed examined the effectiveness of manual therapy for cervical dizziness across multiple randomized controlled trials. The review concluded that manual therapy produces clinically significant improvements in dizziness intensity, frequency, and quality of life.
A landmark 1997 study by Loudon et al. published in Spine and indexed in PubMeddemonstrated that whiplash patients have measurably impaired ability to reproduce head position accurately — providing concrete evidence that proprioceptive dysfunction is a real, measurable consequence of whiplash injury.
A 2003 study by Sterling et al. published in the journal Pain documented the development of motor system dysfunction following whiplash injury, confirming that WAD produces measurable changes in how the body controls movement and balance long after the initial event.
A 2022 narrative review on proprioceptive cervicogenic dizziness published in the Journal of Clinical Medicine confirmed that whiplash is one of the most common triggers for chronic cervicogenic dizziness, and that the upper cervical region (C1–C3) is the primary source of dizziness-relevant proprioceptive input.
According to the Cleveland Clinic, cervical vertigo can develop following cervical spine injuries including whiplash, and manual therapy is one of the most common treatments — improving balance, easing neck pain, and reducing dizziness.
Research published in clinical trials databases confirms that an estimated 20 to 58 percent of patients who sustain whiplash injuries experience late-onset dizziness, vertigo, or disequilibrium — meaning that millions of people every year develop WAD-related dizziness that goes undertreated.
The takeaway from current research is consistent: whiplash-associated vertigo is primarily a cervical spine problem, it is real and measurable, and it responds well to targeted manual care of the upper cervical spine. Upper cervical chiropractic care, done with precision and gentleness, is uniquely well-suited to filling this clinical need.
Lifestyle Habits That Support Recovery from Whiplash-Associated Vertigo
Beyond upper cervical care, daily habits play a major role in WAD recovery. Here’s what we recommend most often to our whiplash patients.
Move regularly — but gentle and graded. Old advice suggested wearing a soft collar and resting for weeks. Current evidence supports active recovery: gentle, daily neck movement and walking actually speed healing compared to prolonged immobilization. Push to the edge of comfort but not into pain.
Sleep well. Quality sleep is when the brain and nervous system do most of their repair work. Aim for 8–9 hours per night during recovery. Use a supportive pillow that maintains proper upper cervical alignment. Stomach sleeping forces sustained neck rotation and should be avoided.
Stay hydrated. Soft tissue healing, vascular regulation, and nervous system function all depend on hydration. Florida’s heat makes daily hydration especially important — aim for at least half your body weight in ounces of water per day.
Watch your posture during phone and computer use. Forward head posture puts continuous strain on the already-injured upper cervical spine. Keep screens at eye level. Take posture breaks every 30 minutes. Your neck cannot heal if you’re loading it improperly all day.
Manage stress. Stress increases sympathetic nervous system activity, tightens neck muscles, and amplifies dizziness. Whiplash often triggers anxiety related to driving and the accident itself, which compounds the physical symptoms. Breathing exercises, walks outside, and gentle daily routines all help.
Drive cautiously during recovery. Returning to driving can trigger anxiety, motion sensitivity, and physical neck tension — all of which can flare WAD symptoms. Don’t push yourself back to driving long distances before you’re ready. Gradual exposure is key.
Limit aggressive cervical care. This is important — avoid forceful neck manipulation, deep tissue massage directed at the upper neck, aggressive cervical traction, and any treatment that produces sharp pain or significant flare-ups during recovery. Gentle care is appropriate. Aggressive care often makes things worse.
Document your case if a car accident was involved. If your whiplash came from a car accident, keep records of all symptoms, treatments, and provider visits. This matters for insurance, legal proceedings, and long-term care planning. Sarasota and Manatee County car accidents often involve complex insurance considerations, and proper documentation supports your recovery and your case.
Address related conditions. WAD patients often have overlapping issues — cervicogenic dizziness, post-traumatic BPPV, post-concussion symptoms, headaches, and TMJ involvement. For more on the deep connection between neck dysfunction and dizziness, our blog on the connection between neck pain and vertigo is an excellent companion read.
Be patient. Whiplash recovery is rarely linear. Good weeks are followed by setbacks. The trajectory matters more than any single week. With the right combination of care, time, and lifestyle support, most patients see meaningful and lasting improvement.
Serving Sarasota and Surrounding Areas
Lavender Family Chiropractic is located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — right at the corner of University and Whitfield. We are easy to reach from anywhere in the greater Sarasota region.
We proudly serve patients dealing with whiplash injuries, post-accident vertigo, and other dizziness conditions from across the area, including:
- Sarasota, FL
- Bradenton, FL
- Lakewood Ranch, FL
- Venice, FL
- Osprey, FL
- Parrish, FL
- Ellenton, FL
- Siesta Key, FL
- Longboat Key, FL
- St. Pete, FL
- Tampa, FL
To learn more about the full region we serve, visit our areas we service page. Wherever you’re driving from, we’re set up to help.
Top 15 FAQs About Whiplash-Associated Vertigo
What is whiplash-associated vertigo?
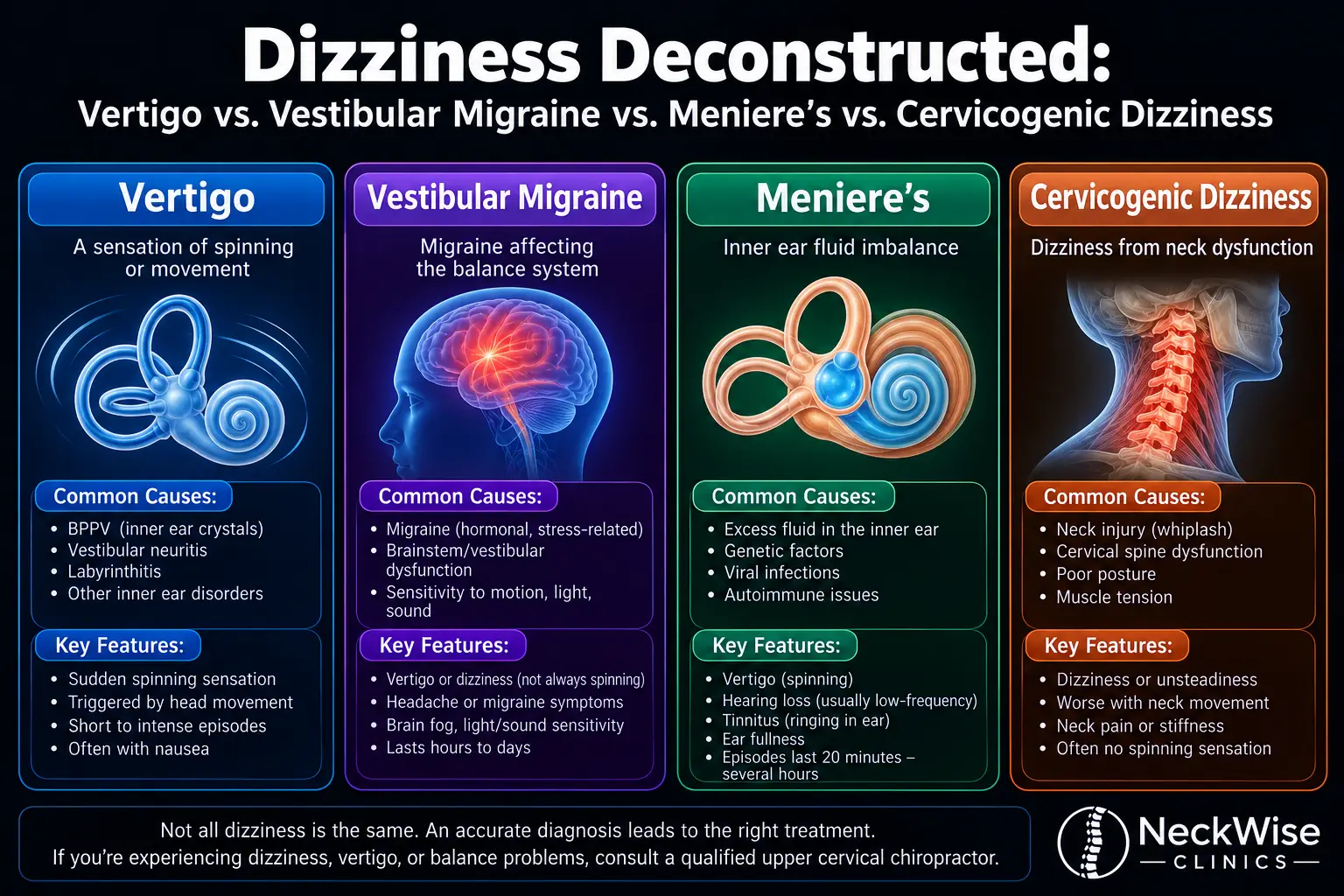
Whiplash-associated vertigo is dizziness, imbalance, or motion sensitivity that develops as a result of a whiplash injury. It can come from cervical proprioceptive dysfunction (the most common cause), direct vestibular injury, concomitant concussion, autonomic dysregulation, or vertebrobasilar involvement — and sometimes all of these at once.
How common is dizziness after whiplash?
Research shows that 20 to 58 percent of whiplash patients develop late-onset dizziness, vertigo, or disequilibrium. This is not a rare or unusual outcome — it’s one of the most common consequences of whiplash injury, especially when the upper cervical spine is not addressed.
Why didn’t my doctor mention my neck as a source of dizziness?
Most general medical training focuses on inner ear and brain causes of dizziness. The cervical spine — especially the upper cervical spine — is often overlooked as a source of vertigo, even though it’s one of the most common contributors. Current research is changing this gradually, but the clinical gap is still wide.
How long does whiplash-associated vertigo last?
Without targeted care, whiplash-associated vertigo can last months to years. With appropriate upper cervical care, most patients begin noticing improvement within the first few weeks and see significant resolution within 6 to 12 weeks of consistent care.
Can a whiplash from years ago still be causing my dizziness today?
Absolutely. Many of our patients trace their persistent dizziness back to a car accident, fall, or sports injury years before their symptoms became severe. Upper cervical misalignment from old whiplash injuries often doesn’t fully resolve on its own and can drive symptoms for decades until properly addressed.
My MRI showed nothing — does that mean my whiplash is fine?
Not necessarily. Standard MRI is designed to detect structural damage like disc herniations and fractures. It often misses the proprioceptive dysfunction, ligamentous strain, and subtle misalignment that drive whiplash-associated vertigo. “Normal” imaging doesn’t mean “normal” function.
Is upper cervical chiropractic care safe after whiplash?
Yes, when done correctly. Forceful chiropractic adjustments are NOT appropriate for whiplash patients, especially in the early phase. Gentle, precise, imaging-guided upper cervical correction (with no twisting, popping, or cracking) is fundamentally different and is one of the most appropriate manual therapy approaches available for whiplash patients.
How soon after a car accident can I receive upper cervical care?
Once acute medical evaluation has ruled out fractures and other emergencies, you can typically begin gentle upper cervical evaluation within days to a couple of weeks. Earlier intervention generally produces better outcomes and helps prevent chronic symptoms from developing.
What’s the difference between whiplash-associated vertigo and post-concussion vertigo?
There’s significant overlap. Many whiplash injuries also produce concussions, and many concussions also produce cervical injury. The distinction is largely academic — what matters clinically is that both conditions usually involve significant upper cervical dysfunction, and both respond well to gentle upper cervical care.
Why does my dizziness flare when I turn my head?
This is a hallmark of cervicogenic dizziness. When the upper cervical proprioceptors are damaged, head movement produces faulty positional signals that the brain interprets as dizziness. Restoring proper cervical function typically resolves this symptom over time.
Will I need other care besides upper cervical correction?
Possibly. Some whiplash patients benefit from a combination of approaches — upper cervical care, vestibular rehabilitation for any inner ear involvement, vision therapy if concussion is also present, and gradual return-to-activity protocols. We work alongside your other providers to give you the best outcome.
Can stress make whiplash symptoms worse?
Yes. Stress increases sympathetic nervous system activity, tightens neck muscles, and amplifies all WAD-related symptoms including dizziness, headaches, and fatigue. Stress management is an important part of WAD recovery.
Should I file a personal injury claim if my whiplash came from a car accident?
That’s a legal question best discussed with a personal injury attorney, but document everything. Keep records of all symptoms, all provider visits, and all treatments. Proper documentation supports both your medical care and any claims process. Our Sarasota office is familiar with the documentation needs of accident-related cases.
Can children and teens get whiplash-associated vertigo?
Yes. Sports injuries, car accidents, and falls all produce whiplash in younger patients. The gentle nature of upper cervical care makes it appropriate for younger patients, and early intervention can prevent chronic patterns from developing.
How do I know if Lavender Family Chiropractic is right for me?
If you’ve experienced a whiplash injury — recent or years ago — and you’re still dealing with dizziness, brain fog, headaches, neck symptoms, or imbalance, you’re an excellent candidate for an evaluation. Call (941) 243-3729 to schedule a complimentary consultation.
You Don’t Have to Live with Whiplash-Associated Vertigo Forever
A car accident is a moment. A fall is a moment. A sports injury is a moment. But for too many patients, the dizziness, fog, and imbalance that follow become a life sentence — not because recovery isn’t possible, but because the right piece of the recovery puzzle was never addressed.
Current research is clear: whiplash-associated vertigo is primarily a cervical spine problem, and it responds well to targeted upper cervical care. The longer it’s left unaddressed, the more entrenched it becomes — but it’s never too late to begin recovery.
At Lavender Family Chiropractic, Dr. Rusty Lavender and Dr. Jacob Temple have helped many whiplash patients across Sarasota and beyond finally find the progress they thought was no longer possible. If you’ve been told to wait it out, learn to live with it, or accept that this is just how things are now — please get a second opinion. The upper cervical piece may be exactly what your recovery has been missing.
📞 Call us today at (941) 243-3729 📅 Or book your complimentary consultation online
Real recovery is still possible — no matter when the injury happened.