By Dr. Rusty Lavender
Thoracic Outlet Syndrome: It often starts as something easy to dismiss. An ache in the shoulder. Numbness or tingling in the hand, especially the ring and little fingers. An arm that fatigues and feels heavy when you raise it overhead — to wash your hair, to reach a high shelf, to hang a picture. Maybe your hand goes cold or pale. Maybe you wake up with your arm “asleep.” You may have been told it is carpal tunnel, or a pinched nerve, or stress, or that you simply slept wrong. You may have had wrist surgery that did not fix it, or a workup that came back inconclusive. And the symptoms persist, because the real source of the problem was never where everyone was looking.
At Lavender Family Chiropractic in Sarasota, Florida, we see patients with thoracic outlet syndrome — and many more who have it but have never received the diagnosis. Thoracic outlet syndrome is one of the most frequently misdiagnosed and underdiagnosed conditions in musculoskeletal medicine, in large part because its symptoms overlap with carpal tunnel syndrome, cervical radiculopathy, rotator cuff problems, and a dozen other conditions. What gets missed in nearly every conventional workup is the role that posture and the alignment of the neck and upper spine play in creating the compression in the first place — and that is precisely where upper cervical chiropractic care becomes relevant.
This guide is for anyone in Sarasota, Bradenton, Lakewood Ranch, or the surrounding areas who has been dealing with arm, shoulder, or hand symptoms that have not been adequately explained or resolved — and who wants to understand what thoracic outlet syndrome really is, why posture and the cervical spine matter so much, and how the precise, gentle Knee Chest Upper Cervical technique used by Dr. Rusty Lavender and Dr. Jacob Temple fits into a comprehensive recovery plan.
What Is Thoracic Outlet Syndrome?
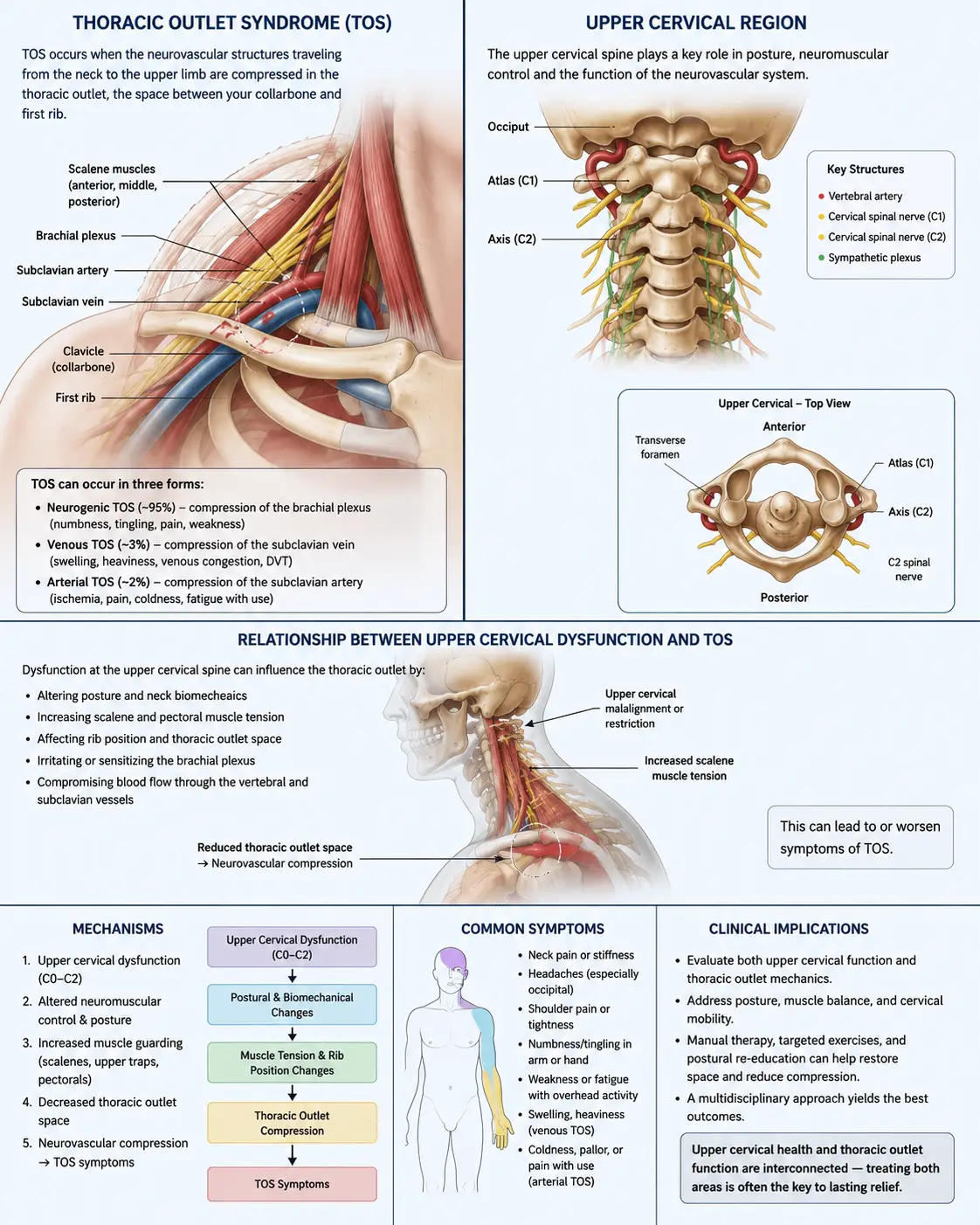
Thoracic outlet syndrome (TOS) is a group of disorders that result from compression of the nerves, arteries, or veins as they pass through the thoracic outlet — the anatomical passageway between your lower neck and your armpit. This passageway is bounded by the first rib, the collarbone (clavicle), and the scalene muscles of the neck. Through this narrow space travel the brachial plexus (the bundle of nerves that supplies the arm and hand), the subclavian artery, and the subclavian vein. When any of these structures gets compressed in this region, the result is thoracic outlet syndrome.
TOS is classified into three types based on which structure is compressed. Neurogenic TOS, which involves compression of the brachial plexus nerves, is by far the most common — accounting for over 90% of all cases according to current estimates. Venous TOS, involving compression of the subclavian vein, accounts for roughly 3 to 5% of cases. Arterial TOS, involving the subclavian artery, is the rarest at around 1%. The vast majority of patients seeking help for TOS have the neurogenic form, and that is the form most relevant to the postural and cervical mechanisms we will discuss.
The symptom picture depends on which structures are compressed. Neurogenic TOS typically produces pain, numbness, tingling, and weakness in the neck, shoulder, arm, and hand — often most pronounced in the ring and little fingers and the inner forearm, following the distribution of the lower brachial plexus. Symptoms classically worsen with overhead activities and with sustained arm positions. Patients may notice their arm fatiguing quickly, a weakening grip, dropping objects, or clumsiness of the hand. Venous TOS tends to produce arm swelling, a bluish discoloration, and a feeling of heaviness. Arterial TOS can produce coldness, pallor, and pain with activity. Some patients experience a mix.
How common is TOS? This is genuinely difficult to pin down, because the diagnosis is contested and the symptoms are nonspecific. Estimates of incidence range widely — from 3 to 80 cases per 1,000 people, depending on the source and the diagnostic criteria used. What is more consistent across the literature is that TOS is more common in women than men, more common in people with poor posture or poor muscle development, and most likely to first appear between the ages of 20 and 50. It is also a condition that disproportionately affects people whose work or sport involves repetitive overhead activity or sustained forward-head, rounded-shoulder postures.
One of the defining features of TOS is how often it is misdiagnosed. Because its symptoms overlap so heavily with carpal tunnel syndrome, cervical radiculopathy, ulnar neuropathy, rotator cuff pathology, and even fibromyalgia, many patients spend months or years — and sometimes undergo unnecessary procedures — before the real source of their symptoms is identified. The famous debate in the medical literature, captured in two 1999 papers with the pointed titles “Thoracic outlet syndrome is underdiagnosed” and “Thoracic outlet syndrome is overdiagnosed,” reflects just how contested and slippery this condition is. The truth is probably that it is both — overdiagnosed in some settings and badly underdiagnosed in others — and that careful, thorough evaluation is essential.
The Postural and Cervical Connection: Why Your Neck Drives Your Arm Symptoms
Here is where the thoracic outlet syndrome story connects directly to posture and the cervical spine — and where the upper cervical angle becomes genuinely defensible rather than a stretch.
The thoracic outlet is bounded and defined in large part by structures that are directly controlled by neck posture and cervical alignment. The scalene muscles — anterior, middle, and posterior — attach to the cervical vertebrae and to the first and second ribs, and they form one wall of the most common compression site, the scalene triangle. The first rib forms the floor of the outlet. The position of the head, neck, and shoulders determines the tension in the scalenes, the position of the first rib, and the amount of space available in the outlet for the nerves and vessels to pass through.
This is why posture is so central to TOS. When the head sits forward of the shoulders — the forward head posture that has become epidemic in the smartphone and computer era — the scalene muscles are placed under chronic tension and the entire geometry of the thoracic outlet changes. The shoulders round forward, the chest collapses, the first rib elevates, and the space available in the outlet narrows. Over time, this postural pattern is one of the most common drivers of neurogenic TOS. The connection is so well established that conservative TOS treatment universally begins with postural correction.
The medical literature is explicit about this. According to a treatment review, physical therapy that addresses postural abnormalities and muscle imbalance relieves symptoms in most patients with thoracic outlet syndrome by relieving pressure on the thoracic outlet, and the review explains that abnormal static or repetitive postures create chronic nerve compression, maintain muscles in shortened positions, and produce the muscle imbalances that perpetuate the problem. In other words, posture is not a minor footnote in TOS — it is one of the primary drivers, and correcting it is one of the primary treatments.
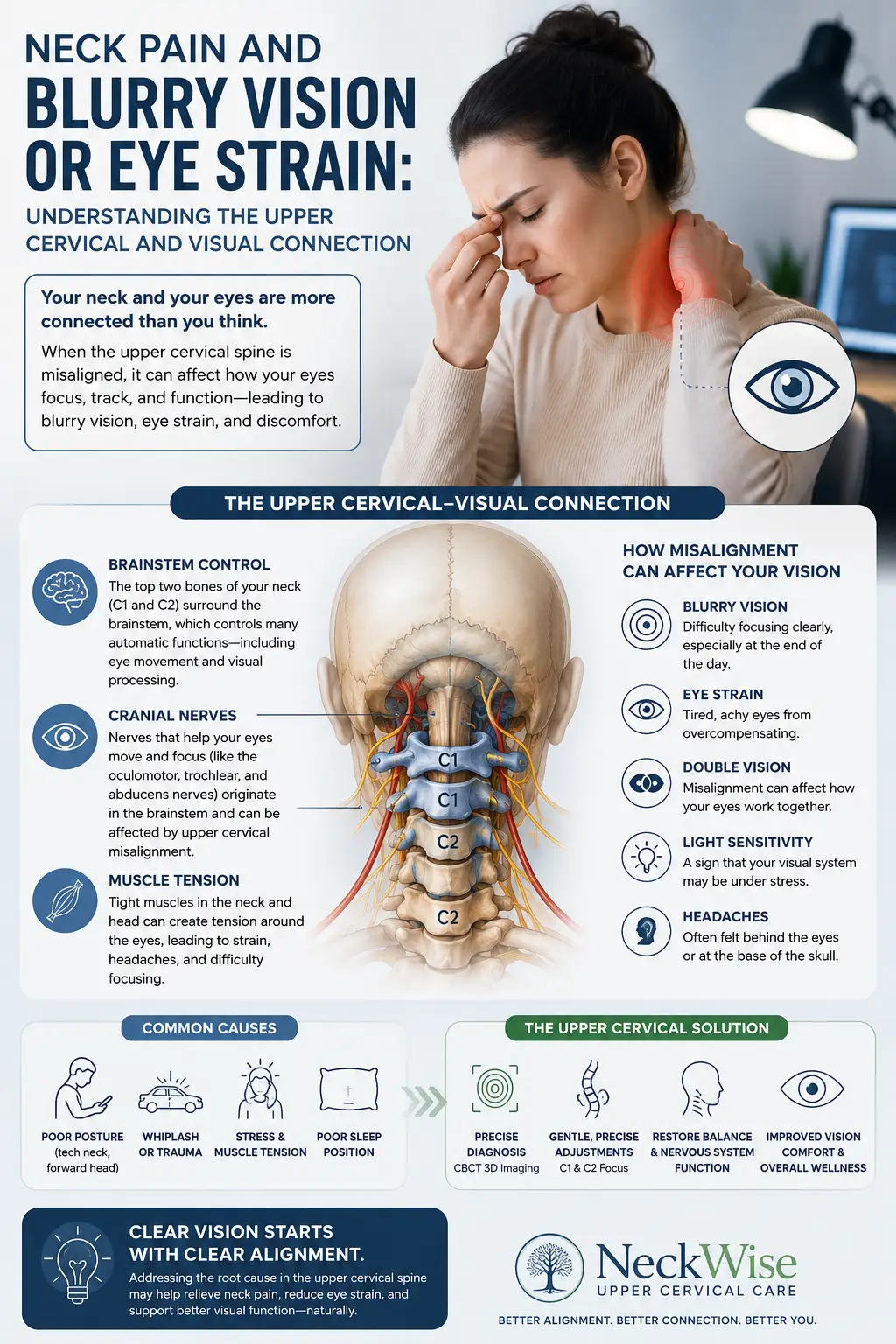
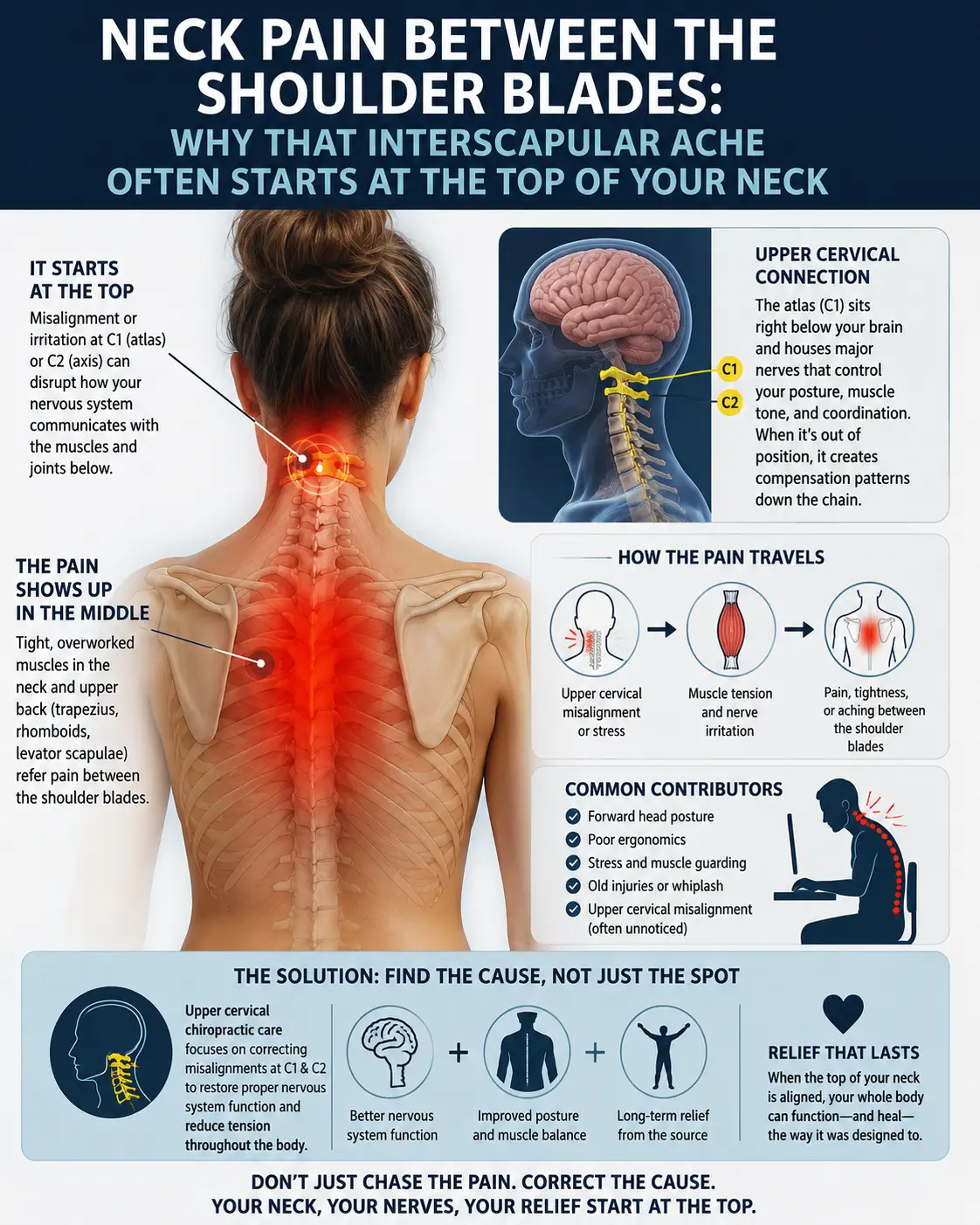
Now connect this to the upper cervical spine. The atlas (C1) and axis (C2) at the top of the neck are the foundation of cervical posture and head position. When the upper cervical spine is misaligned, the body compensates with a cascade of postural changes down the entire spine — including the forward head posture and rounded-shoulder pattern that directly narrows the thoracic outlet. The scalene muscles attach to the cervical vertebrae, so their tension is influenced by cervical alignment. Correcting the upper cervical foundation can help restore the head-over-shoulders posture that takes tension off the scalenes, lowers the first rib, and opens the thoracic outlet.
There is a second, deeper connection worth understanding: the double crush phenomenon. In 1973, Upton and McComas introduced the concept of “double crush” — the observation that a nerve compressed at one point along its course becomes more vulnerable to symptoms from compression at a second point. A nerve root that is already irritated where it exits the cervical spine is more likely to become symptomatic when the same nerve is compressed downstream at the thoracic outlet, and vice versa. This means that cervical spine dysfunction and thoracic outlet compression can compound one another — and that addressing the cervical contribution can meaningfully reduce the overall nerve irritation, even when the thoracic outlet compression itself is also being addressed. This is the same double-crush principle that connects TOS to conditions like cervical radiculopathy and carpal tunnel syndrome.
We want to be honest and precise here, because TOS care is full of overselling. Upper cervical correction does not remove a cervical rib, does not directly decompress the subclavian vein, and is not a stand-alone cure for every case of TOS. What it does is address the postural foundation and the cervical contribution to the double-crush picture — both of which are legitimate, well-documented parts of neurogenic TOS. For the right patients, this is a meaningful piece of a comprehensive recovery strategy.
Why Upper Cervical Care Matters for Thoracic Outlet Syndrome
At Lavender Family Chiropractic, we use the Knee Chest Upper Cervical technique — a precise, gentle approach to correcting atlas and axis misalignments without any twisting, popping, or forceful manipulation. For TOS patients, this matters in several specific ways.
First, by correcting the upper cervical misalignment that drives forward head posture and rounded shoulders, we help restore the head-over-shoulders alignment that takes chronic tension off the scalene muscles and helps open the thoracic outlet. This addresses one of the primary postural drivers of neurogenic TOS rather than just treating the symptoms.
Second, by addressing the cervical contribution to the double-crush phenomenon, upper cervical care reduces the overall load of nerve irritation. When the brachial plexus nerves are no longer being irritated at the cervical level, the same nerves are better able to tolerate any residual compression at the thoracic outlet, and symptoms often improve.
Third, upper cervical correction restores proper proprioceptive input and supports the postural control system that governs how the head, neck, and shoulders are held in space. Posture is not just a mechanical phenomenon — it is a neurological one, governed by the brainstem and the postural reflexes that depend on accurate upper cervical input. Correcting the upper cervical spine helps the postural control system do its job, which supports lasting postural improvement rather than the temporary correction that comes from consciously “sitting up straight.”
It is worth understanding what the broader literature says about conservative care for TOS, because it strongly supports a non-surgical first approach. According to multiple reviews, conservative management — including postural correction, physical therapy, and lifestyle modification — is the recommended first-line treatment for TOS and is successful in most patients, with surgery generally reserved for patients who fail conservative care or who have severe vascular involvement. Our upper cervical work fits within this conservative-first model, addressing the postural and cervical foundation that conservative care universally targets.
We want to be clear about our role. Upper cervical care is one part of a comprehensive approach to TOS. Most TOS patients also benefit from targeted physical therapy — scalene and pectoralis stretching, first-rib mobilization, postural strengthening, and nerve gliding exercises — and we are happy to coordinate with physical therapists and other providers. For patients with a cervical rib, significant vascular involvement, or symptoms that fail conservative care, surgical evaluation may be appropriate, and we will tell you that honestly.
What Care Looks Like at Lavender Family Chiropractic
If you come to our Sarasota office for evaluation related to thoracic outlet syndrome, here is what to expect.
Your first visit begins with a thorough consultation. Dr. Lavender or Dr. Temple will sit down with you and review your full history — when symptoms started, the exact pattern of your arm, shoulder, and hand symptoms, what makes them better or worse, what work or activities you do, what imaging and testing you have had, and what other providers have told you. Because TOS is so frequently confused with other conditions, we pay close attention to the specific pattern of your symptoms to help distinguish TOS from carpal tunnel syndrome, cervical radiculopathy, and other look-alikes.
The examination includes a detailed neurological evaluation, TOS-specific provocative testing (maneuvers that reproduce symptoms by narrowing the thoracic outlet), postural and gait analysis, and advanced 3D imaging to assess your upper cervical alignment and overall spinal posture. We also screen carefully for red flags. If you have signs of significant vascular involvement (arm swelling, discoloration, signs of blood clot) or progressive neurological deficit, we will direct you to appropriate medical or vascular evaluation immediately — vascular TOS in particular can be serious and requires prompt medical care.
If the examination reveals an upper cervical and postural component contributing to your TOS, we will explain honestly how upper cervical care fits into your overall recovery — and where it does not. We are direct about the fact that most TOS patients also benefit from targeted physical therapy and other interventions, and we coordinate with those providers. We see ourselves as one part of your care team.
Care is delivered through the gentle Knee Chest Upper Cervical technique. We offer customized treatment plans tailored to your specific situation, with transparent timelines and honest expectations.
📞 Call (941) 243-3729 to schedule your complimentary consultation 📅 Book your consultation online 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
What the Research Says About Thoracic Outlet Syndrome and Conservative Care
The research on TOS reflects both the difficulty of diagnosing it and the strong consensus that conservative care should come first.
The epidemiological foundation is well documented. The StatPearls review established that neurogenic TOS accounts for over 90% of all cases, that TOS is more prevalent in females and in those with poor posture or poor muscle development, and that estimated incidence ranges from 3 to 80 cases per 1,000 population — with the wide range reflecting the genuine difficulty of diagnosing this contested condition.
A 2021 epidemiological review in Thoracic Surgery Clinics confirmed that the incidence of neurogenic TOS is approximately 95% of known cases, with venous and arterial TOS representing roughly 3% and 1% respectively, and documented the postural, traumatic, and repetitive-strain etiologies that drive the neurogenic form.
The consensus on treatment is clear and consistent. The StatPearls review states plainly that conservative management, consisting of lifestyle modifications and physical therapy, is the recommended first-line treatment for TOS, with postural correction being a common adjustment that relieves symptoms, and that surgery is reserved for severe or refractory cases. A treatment review reinforced that physical therapy addressing postural abnormalities and muscle imbalance relieves symptoms in most TOS patients by relieving pressure on the thoracic outlet, explicitly identifying abnormal posture as a primary mechanism of nerve compression.
A 2021 narrative review in PMC summarized the management landscape, confirming that general first-line therapy for thoracic outlet syndrome is conservative treatment, including physical therapy and lifestyle modifications, with surgical decompression reserved for patients who have failed conservative therapy — reinforcing the conservative-first model that upper cervical care fits within.
The double-crush concept, introduced by Upton and McComas in their 1973 Lancet paper, remains a foundational principle for understanding why cervical spine dysfunction and distal nerve compression syndromes like TOS so often coexist and compound one another — providing the mechanistic basis for addressing the cervical contribution in TOS patients.
This body of research does not establish that upper cervical chiropractic cures TOS. What it establishes is that posture is a primary, well-documented driver of neurogenic TOS, that conservative care addressing posture is the recommended first-line treatment, and that the cervical spine’s relationship to the thoracic outlet (both postural and through the double-crush phenomenon) is legitimate and meaningful.
Lifestyle Factors That Support Thoracic Outlet Syndrome Recovery
Whether or not upper cervical care is part of your strategy, the daily inputs you control are central to TOS recovery. Because posture is such a primary driver, lifestyle factors matter even more in TOS than in many other conditions.
Posture correction. This is the single most important factor. Bring screens to eye level, keep the head stacked over the shoulders rather than jutting forward, and avoid the rounded-shoulder, collapsed-chest posture that narrows the thoracic outlet. Postural awareness throughout the day is foundational.
Sleep position. Avoid sleeping with your arms in an overhead or abducted position, which compresses the thoracic outlet for hours at a time. Sleep on your back or on your uninvolved side, and keep your arms down. Many TOS patients find their worst symptoms occur in the morning specifically because of overhead sleeping postures.
Avoid heavy bags on the shoulder. Carrying a heavy purse, backpack, or bag on the affected shoulder depresses the shoulder girdle and compresses the thoracic outlet. Switch to a backpack worn properly, a rolling bag, or carry less.
Scalene and pectoral stretching. Gentle stretching of the scalene muscles in the neck and the pectoralis muscles in the chest helps relieve the muscle tightness that contributes to outlet compression. A physical therapist can teach you the right techniques.
Strengthen the postural muscles. The muscles that pull the shoulders back and down — the middle and lower trapezius, the rhomboids, the serratus anterior — counteract the forward, rounded posture that drives TOS. Rows, scapular retraction exercises, and postural strengthening are valuable, but progress carefully to avoid aggravating symptoms.
Diaphragmatic breathing. Many TOS patients are chronic chest breathers, which overuses the scalene muscles (which act as accessory breathing muscles) and keeps them tight. Learning to breathe with the diaphragm rather than the upper chest reduces chronic scalene tension.
Activity modification. Reduce or modify repetitive overhead activities and sustained arm positions that provoke symptoms. This may mean adjusting how you work, how you exercise, or how you perform daily tasks.
Stress management. Stress increases muscle tension throughout the neck and shoulders, including the scalenes, which can worsen outlet compression. Whatever practices help you down-regulate are worth incorporating.
If you found this guide useful, you may also want to read our blog on forward head posture and tech neck, the postural pattern that is one of the most common drivers of thoracic outlet syndrome.
Serving Sarasota and the Surrounding Communities
Lavender Family Chiropractic is located in Sarasota, Florida, at 5899 Whitfield Avenue, Suite 107 — at the corner of University and Whitfield. From this central location, we serve patients throughout the region, including Bradenton, Lakewood Ranch, Palmetto, Parrish, Venice, Osprey, Nokomis, Ellenton, Ruskin, Myakka City, North Port, and the greater Tampa Bay area. Patients also travel from St. Pete, Riverview, and Manatee County to receive specialized upper cervical care here.
Thoracic outlet syndrome is one of the most frequently misdiagnosed conditions there is, and many patients have been searching for years for someone who understands the postural and cervical mechanisms behind their symptoms. If that describes you, we encourage you to reach out for an honest evaluation.
Top 15 FAQs About Thoracic Outlet Syndrome and Upper Cervical Chiropractic Care
1. What is thoracic outlet syndrome in simple terms? TOS is compression of the nerves, arteries, or veins as they pass through the narrow space between your lower neck and your armpit — the thoracic outlet. This compression causes pain, numbness, tingling, and weakness in the neck, shoulder, arm, and hand. The most common form, neurogenic TOS, involves compression of the brachial plexus nerves.
2. Why is TOS so often misdiagnosed? Because its symptoms overlap heavily with carpal tunnel syndrome, cervical radiculopathy, ulnar neuropathy, rotator cuff problems, and other conditions — and because there is no single universally accepted diagnostic test. Many patients spend months or years, and sometimes undergo unnecessary procedures, before TOS is identified.
3. Can upper cervical chiropractic cure thoracic outlet syndrome? We want to be honest: upper cervical care does not remove a cervical rib or directly decompress a blood vessel. What it can do is address the postural foundation and the cervical contribution to the double-crush phenomenon, both of which are legitimate, well-documented parts of neurogenic TOS. For the right patients, it is a meaningful piece of a comprehensive strategy.
4. Why would my neck affect symptoms in my hand? Because the thoracic outlet is bounded by the scalene muscles (which attach to the cervical vertebrae) and the first rib, and because head and neck posture directly determines the space available in the outlet. Forward head posture, often driven by upper cervical misalignment, is one of the most common causes of neurogenic TOS.
5. What is the double crush phenomenon? It is the principle, introduced in 1973, that a nerve compressed at one point becomes more vulnerable to symptoms from compression at a second point. Cervical spine irritation and thoracic outlet compression can compound one another, which is why addressing the cervical contribution can reduce the overall nerve irritation in TOS.
6. Is TOS the same as carpal tunnel syndrome? No, though they are frequently confused. Carpal tunnel involves compression of the median nerve at the wrist. TOS involves compression of the brachial plexus or vessels at the thoracic outlet, higher up. They can also coexist via the double-crush phenomenon, which is one reason carpal tunnel surgery sometimes fails to resolve symptoms.
7. Do I need surgery for TOS? Most people do not. Conservative care — postural correction, physical therapy, lifestyle modification — is the recommended first-line treatment and is successful in most patients. Surgery is generally reserved for those who fail conservative care or who have significant vascular involvement.
8. Is upper cervical care safe for TOS? The Knee Chest Upper Cervical technique is exceptionally gentle, with no twisting or forceful manipulation. It is generally very safe. We screen carefully for vascular red flags and will direct you to appropriate medical care if signs of significant vascular involvement are present.
9. How long does conservative care take to work for TOS? Many patients see improvement within weeks to a few months of consistent conservative care addressing posture and the cervical contribution. Chronic or longstanding cases may take longer. We provide honest timelines based on your specific findings.
10. Can poor posture really cause TOS? Yes — it is one of the primary drivers of neurogenic TOS. Forward head posture and rounded shoulders narrow the thoracic outlet, place the scalene muscles under chronic tension, and elevate the first rib. This is why postural correction is universally part of TOS treatment.
11. Can a car accident cause TOS? Yes. Whiplash and other trauma can cause or contribute to TOS by injuring the soft tissues, altering posture, and creating cervical dysfunction. Our car accident chiropractic care addresses the whole-spine consequences of collisions, including the cervical and postural factors relevant to TOS.
12. What kind of doctor diagnoses TOS? TOS may be evaluated by vascular surgeons, neurologists, physiatrists, physical therapists, and chiropractors, among others. Because it is so easily confused with other conditions, a thorough clinical evaluation combining history, provocative testing, and appropriate imaging is essential. We perform this evaluation and coordinate with other specialists as needed.
13. Should I see a physical therapist too? Often, yes. Most TOS patients benefit from targeted physical therapy — scalene and pectoral stretching, first-rib mobilization, postural strengthening, and nerve gliding. We view upper cervical care and physical therapy as complementary and are happy to coordinate care.
14. How will I know if upper cervical care is right for me? The only way to know is a thorough evaluation. We will assess whether your upper cervical alignment and posture are contributing to your TOS, screen for red flags, and give you an honest assessment of whether upper cervical care is likely to help — and what else you may need.
15. How do I get started? Call our Sarasota office at (941) 243-3729 or book your consultation online. We will review your history, perform a thorough examination, screen for red flags, and give you a straight answer about how upper cervical care fits into your recovery.
Take the Next Step Toward Relief
Thoracic outlet syndrome is one of the most misunderstood and misdiagnosed conditions in musculoskeletal medicine — and for many patients, the postural and cervical mechanisms that drive it are never properly addressed. The good news is that most TOS responds to conservative care, that surgery is needed for only a minority of cases, and that addressing the postural foundation and the cervical contribution can make a meaningful difference for the right patients.
If you are in Sarasota, Bradenton, Lakewood Ranch, or anywhere in the surrounding region and you are dealing with unexplained arm, shoulder, or hand symptoms — or you have been diagnosed with TOS and want to address the postural and cervical components — Dr. Rusty Lavender and Dr. Jacob Temple at Lavender Family Chiropractic are here to give you an honest evaluation of where upper cervical care fits into your recovery.
📞 Call (941) 243-3729 today to schedule your complimentary consultation 📅 Book online here 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield