By Dr. Rusty Lavender
Carpal Tunnel Syndrome: The symptoms are familiar to millions of people. Numbness and tingling in the thumb, index, and middle fingers. Hands that fall asleep at night and wake you up needing to shake them out. A weakening grip, dropped coffee mugs, fumbled keys. Pain that radiates from the wrist up into the forearm. For most people with these symptoms, the diagnosis is carpal tunnel syndrome, and the standard path is well worn: wrist splints, anti-inflammatories, a cortisone injection, and — if those fail — carpal tunnel release surgery.
But here is something that surprises many patients: a substantial number of people who undergo carpal tunnel surgery do not get full relief. And one of the most important reasons, supported by decades of research, is that the median nerve may be compressed not only at the wrist, but also higher up — at the level of the cervical spine. When a nerve is compressed at two points along its course, the condition is called double crush syndrome, and it is one of the most overlooked reasons carpal tunnel treatment fails.
At Lavender Family Chiropractic in Sarasota, Florida, we want to be honest with you from the start, because honesty is the foundation of good care: carpal tunnel syndrome is fundamentally a wrist problem. The median nerve is compressed within the carpal tunnel at the wrist, and we do not claim that adjusting your neck repairs that wrist compression. We are an upper cervical practice, not hand surgeons. What we can tell you, and what this guide explains in detail, is that for many carpal tunnel patients, the cervical spine is part of the picture — through the double-crush phenomenon — and that addressing the cervical contribution can be a meaningful part of a comprehensive approach. This guide is for anyone in Sarasota, Bradenton, Lakewood Ranch, or the surrounding areas who wants to understand what carpal tunnel syndrome really is, why the neck matters more than most providers acknowledge, and where upper cervical care fits — and does not fit — into recovery.
What Is Carpal Tunnel Syndrome?
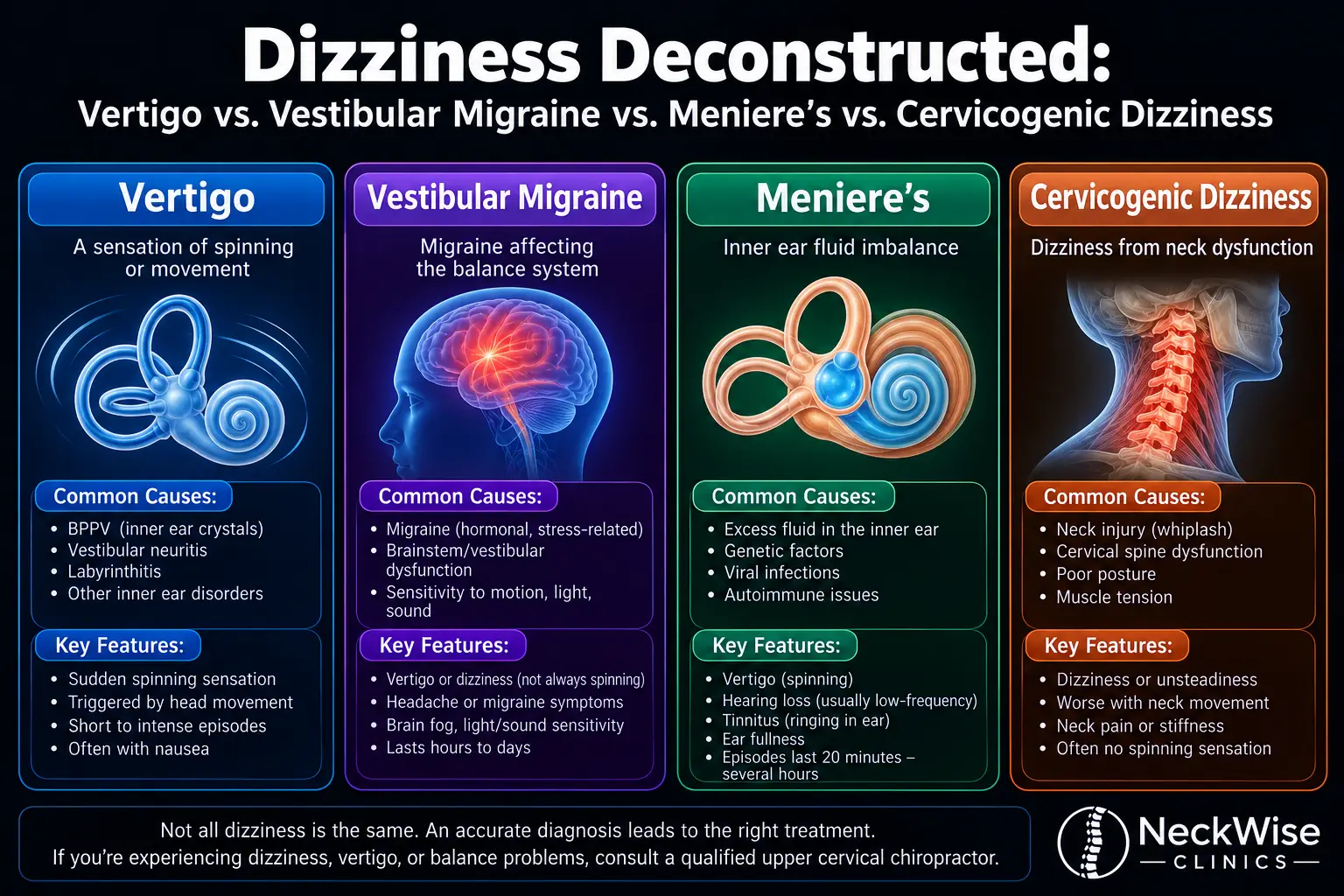
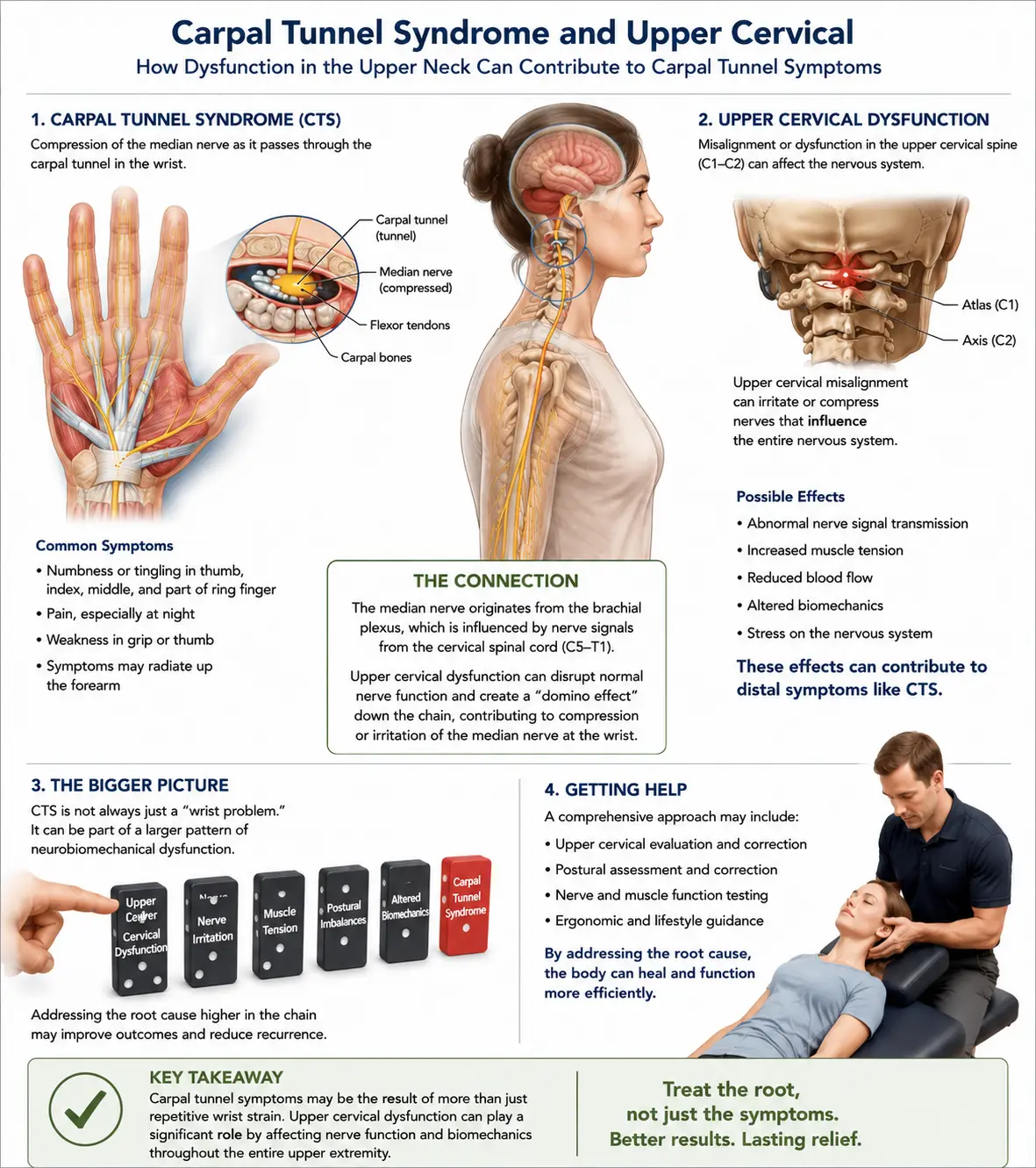
Carpal tunnel syndrome (CTS) is the most common peripheral compression neuropathy, caused by compression of the median nerve as it passes through the carpal tunnel — a narrow passageway on the palm side of the wrist, bounded by the carpal bones below and the transverse carpal ligament above. Through this tight space pass the median nerve and nine flexor tendons. When the pressure within the tunnel rises — from swelling, inflammation, repetitive strain, or anatomical factors — the median nerve gets compressed, and the result is the characteristic symptoms of carpal tunnel syndrome.
The median nerve supplies sensation to the thumb, index finger, middle finger, and half of the ring finger, and it controls some of the muscles at the base of the thumb. This is why the classic symptoms of CTS appear in this specific distribution. Patients typically experience numbness, tingling, and pain in the thumb and first two or three fingers — but notably not the little finger, which is supplied by the ulnar nerve. Symptoms are often worst at night and frequently wake patients from sleep, prompting the characteristic “flick sign” of shaking the hand to relieve symptoms. As the condition progresses, patients may develop weakness of grip, difficulty with fine motor tasks like buttoning a shirt, and, in severe cases, wasting of the thenar muscles at the base of the thumb.
How common is carpal tunnel syndrome? It is extraordinarily common. According to epidemiological data, the prevalence of carpal tunnel syndrome in the general population is approximately 9.2% in women and 6% in men, making it the most frequent compressive neuropathy. A landmark population study published in Neurology documented a mean annual incidence of 329 cases per 100,000 person-years, with rates substantially higher in women (506 per 100,000) than in men (139 per 100,000). Among active workers in certain occupations, prevalence can reach 10% or higher. Carpal tunnel syndrome is also the most expensive upper-extremity musculoskeletal disorder, with U.S. medical costs exceeding $2 billion annually, primarily due to surgical releases.
The risk factors are well established and include repetitive hand and wrist use, sustained awkward wrist positions, vibration exposure, obesity, diabetes, hypothyroidism, pregnancy, rheumatoid arthritis, and female sex. The peak age of onset is generally between 45 and 60. For a region like Sarasota, with a large population of retirees, office workers, manual laborers, and people managing diabetes and other metabolic conditions, carpal tunnel syndrome is one of the most common reasons people seek help for hand symptoms.
The encouraging reality is that carpal tunnel syndrome is highly treatable, and that conservative care helps many patients avoid surgery. But for the patients whose symptoms persist despite wrist-focused treatment — or who have surgery and still do not get full relief — the missing piece is frequently found higher up, in the cervical spine.
The Double-Crush Connection: Why Your Neck May Be Part of Your Wrist Problem
This is the part of the carpal tunnel story that most patients are never told, and it is genuinely important — and, to be intellectually honest, genuinely debated.
In 1973, neurologists Upton and McComas published a now-famous paper in The Lancet introducing the concept of “double crush syndrome.” Their observation was that a peripheral nerve compressed at one point along its course becomes more vulnerable to dysfunction from a second compression at another point along the same nerve. The proposed mechanism is that proximal compression disrupts the normal axoplasmic flow — the transport of nutrients and materials along the nerve fiber — which makes the more distal portion of the nerve more susceptible to injury, even from a compression that might otherwise be tolerated.
For carpal tunnel syndrome, this matters because the median nerve does not begin at the wrist. Its nerve fibers originate from the cervical nerve roots in the neck (primarily C6, C7, and C8), travel through the brachial plexus, pass through the thoracic outlet, course down the arm and forearm, and finally pass through the carpal tunnel at the wrist. A compression or irritation of these nerve fibers at the cervical level — from a misalignment, disc bulge, foraminal narrowing, or the postural strain so common in the modern era — can, according to the double-crush model, predispose the median nerve to becoming symptomatic at the wrist.
How often do carpal tunnel syndrome and cervical nerve compression coexist? The research shows it is common, though the numbers and the interpretation vary considerably across studies. One study found that 95 out of 126 carpal tunnel patients (75.4%) had probable concurrent cervical radiculopathy. Other studies have reported coexistence rates around 18 to 26%. A review documented that double crush between the cervical spine and the median nerve has been well documented, and importantly noted that roughly 30% of median nerve double crush patients considered their carpal tunnel release surgery a failure, which may be related to persistent cervical nerve compression that was never addressed.
We want to be honest about the controversy here, because that honesty is exactly what distinguishes responsible care from overselling. The double-crush hypothesis is debated in the medical literature. Some researchers argue it is invoked far more often than the strict anatomical and physiological evidence warrants. One careful study revisiting 301 cases of median nerve neuropathy found that while about 25% of carpal tunnel patients had some form of double compression, only about 7.3% met the strict criteria necessary to genuinely explain a true double-crush mechanism. The honest summary is this: double crush is a real clinical entity, the median nerve is the most commonly involved nerve, cervical and wrist compression frequently coexist, and the cervical contribution genuinely matters for a meaningful subset of patients — but it is not the explanation for every case, and anyone who claims it is would be overstating the science.
What this means practically is straightforward. For carpal tunnel patients whose cervical spine is also involved, addressing only the wrist leaves part of the problem unaddressed — which is one reason carpal tunnel surgery sometimes fails to deliver full relief. And the cervical spine, particularly the postural and alignment factors that influence the cervical nerve roots, is exactly where upper cervical care can contribute.
Why Upper Cervical Care Matters for Carpal Tunnel Syndrome
Let us be clear about our role, because it would be easy to overstate it. At Lavender Family Chiropractic, we use the Knee Chest Upper Cervical technique — a precise, gentle method of correcting atlas and axis misalignments without twisting, popping, or forceful manipulation. We do not perform carpal tunnel release, and upper cervical correction does not open the carpal tunnel at the wrist. What upper cervical care addresses is the cervical and postural contribution to the double-crush picture.
For the right carpal tunnel patients, upper cervical care can contribute in several ways. First, by correcting upper cervical misalignment and improving overall cervical posture, we help reduce irritation of the cervical nerve roots from which the median nerve fibers originate. According to the double-crush model, reducing this proximal irritation can make the median nerve less susceptible to symptoms at the wrist. Second, upper cervical correction addresses the forward head posture and rounded-shoulder pattern that increase tension throughout the entire course of the median nerve, from the neck through the thoracic outlet and down the arm. Third, by supporting the overall function of the cervical spine and the postural control system, upper cervical care can be part of reducing the total load of nerve irritation that the median nerve is experiencing along its full path.
This is also why carpal tunnel syndrome connects so closely to two other conditions we address. Cervical radiculopathy— a pinched nerve in the neck — is the classic proximal half of the median nerve double crush. And thoracic outlet syndrome represents compression at the thoracic outlet, a third potential crush point along the same nerve pathway. For patients with symptoms that do not fit neatly into a single diagnosis, evaluating the whole nerve pathway — not just the wrist — is essential, and this is a perspective that wrist-focused care often misses.
We want to be honest about candidacy. If your carpal tunnel syndrome is purely a wrist-level problem with no cervical or postural contribution, upper cervical care is unlikely to resolve it, and we will tell you that. Many carpal tunnel patients benefit most from wrist-focused conservative care — splinting, activity modification, ergonomic changes, and addressing underlying metabolic factors like diabetes or thyroid dysfunction — and some need surgical release. Our role is to evaluate whether the cervical spine is part of your picture and to address that component when it is relevant, as part of a comprehensive approach.
What Care Looks Like at Lavender Family Chiropractic
If you come to our Sarasota office for evaluation related to carpal tunnel syndrome, here is what to expect.
Your first visit begins with a thorough consultation. Dr. Lavender or Dr. Temple will sit down with you and review your full history — when symptoms started, the exact pattern and distribution of your numbness and tingling, what makes symptoms better or worse, your work and activities, any underlying conditions like diabetes or thyroid problems, what testing you have had, and what treatments you have tried. We pay particular attention to whether your symptoms suggest pure wrist-level carpal tunnel or whether there are signs pointing to a cervical or double-crush component — neck pain, symptoms extending above the wrist, involvement of the ring and little fingers, or a history of neck problems.
The examination includes a detailed neurological evaluation, carpal tunnel provocative testing (such as Phalen’s and Tinel’s tests), cervical and postural assessment, and advanced 3D imaging to evaluate your upper cervical alignment and overall posture. We screen for red flags and for signs that warrant referral — significant thenar muscle wasting or severe nerve damage, for example, may require prompt surgical evaluation, and we will tell you that directly.
If the examination reveals a cervical and postural component contributing to your carpal tunnel symptoms, we will explain honestly how upper cervical care fits into your overall recovery — and where it does not. We are direct about the fact that many carpal tunnel patients also need wrist-focused care, ergonomic changes, or medical management of underlying conditions, and we coordinate with other providers. We see ourselves as one part of your care team.
Care is delivered through the gentle Knee Chest Upper Cervical technique. We offer customized treatment plans tailored to your specific situation, with transparent timelines and honest expectations about what upper cervical care can and cannot accomplish for your particular case.
📞 Call (941) 243-3729 to schedule your complimentary consultation 📅 Book your consultation online 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
What the Research Says About Carpal Tunnel Syndrome and the Double-Crush Phenomenon
The research on carpal tunnel syndrome is extensive, and the literature on the double-crush phenomenon is substantial, if genuinely debated.
The epidemiological foundation is well established. A study of hospital workers documented that carpal tunnel syndrome has a general population prevalence of approximately 9.2% in women and 6% in men, making it the most frequent compressive neuropathy. The landmark Neurology population study reported a mean annual incidence of 329 cases per 100,000 person-years, with women affected far more often than men — establishing carpal tunnel syndrome as one of the most common neurological conditions in the general population.
The double-crush research provides the basis for the cervical connection. A study of 126 carpal tunnel patients found that 95 (75.4%) had probable concurrent cervical radiculopathy, suggesting a high rate of coexistence. A 2020 review documented that double crush between the cervical spine and median nerve is well documented at a rate around 18%, with C5 and C6 most commonly affected, and that approximately 30% of median nerve double-crush patients considered their carpal tunnel release a failure — directly linking unaddressed cervical compression to surgical failure.
A 2021 cadaveric study published in PMC examined the median nerve histologically and concluded that the structural differences along the nerve help explain the high concomitant occurrence of carpal tunnel syndrome and cervical radiculopathy, and recommended cautious evaluation of patients with upper limb symptoms because these conditions require different management approaches — providing anatomical support for the double-crush concept.
In the interest of honesty, the literature also includes important skepticism. A study revisiting 301 cases of median nerve neuropathy found that while about 25% of carpal tunnel patients had some double compression, only about 7.3% met the strict anatomical and physiological criteria needed to genuinely qualify as a true double-crush syndrome, concluding that the hypothesis is invoked far more often than warranted. This is an important corrective, and we present it because intellectual honesty matters: double crush is real and clinically meaningful for a subset of patients, but it is not the universal explanation that some providers claim.
Taken together, this body of research establishes that carpal tunnel syndrome is extremely common, that it frequently coexists with cervical nerve compression, that the double-crush phenomenon is a real (if sometimes overinvoked) entity, and that unaddressed cervical contribution is a documented reason carpal tunnel surgery sometimes fails. This is the legitimate, evidence-based basis for evaluating the cervical spine in carpal tunnel patients.
Lifestyle Factors That Support Carpal Tunnel Syndrome Recovery
Whether or not upper cervical care is part of your strategy, the daily inputs you control matter enormously for carpal tunnel recovery. Conservative care helps many patients avoid surgery, and lifestyle factors are central to it.
Wrist splinting. A neutral-position wrist splint, particularly worn at night, is one of the most effective conservative treatments for carpal tunnel syndrome. It keeps the wrist from flexing during sleep, which is when many patients’ symptoms are worst.
Ergonomics. Adjust your workstation so your wrists stay in a neutral position rather than bent up or down. Keep your keyboard and mouse at the right height, use wrist supports appropriately, and take frequent breaks from repetitive hand activities.
Activity modification. Identify and modify the repetitive hand and wrist activities that provoke your symptoms. This may mean changing technique, taking more frequent breaks, or using ergonomic tools.
Posture correction. Because the median nerve travels from the neck to the wrist, forward head posture and rounded shoulders increase tension along its entire course. Bringing the head over the shoulders and opening the chest reduces this whole-pathway tension — addressing the cervical and thoracic outlet contributions to the double-crush picture.
Manage underlying conditions. Diabetes, hypothyroidism, and obesity are significant risk factors for carpal tunnel syndrome. Managing blood sugar, thyroid function, and weight can meaningfully reduce symptoms and prevent progression. Work with your medical provider on these.
Anti-inflammatory measures. Because swelling and inflammation raise pressure within the carpal tunnel, an anti-inflammatory approach — minimizing processed foods, refined sugars, and seed oils while emphasizing whole foods and omega-3-rich fish — can be supportive. Adequate hydration matters too.
Nerve gliding exercises. Gentle median nerve gliding (or “flossing”) exercises can help the nerve move freely along its pathway and may reduce symptoms. A physical therapist or hand therapist can teach you the proper technique.
Address the whole nerve pathway. If your symptoms persist despite wrist-focused care, consider whether the cervical spine and thoracic outlet are part of the picture. Treating only the wrist when the problem is a double crush leaves part of the problem unaddressed.
If you found this guide useful, you may also want to read our blog on thoracic outlet syndrome, another nerve-compression condition along the same pathway that frequently coexists with carpal tunnel syndrome through the double-crush phenomenon.
Serving Sarasota and the Surrounding Communities
Lavender Family Chiropractic is located in Sarasota, Florida, at 5899 Whitfield Avenue, Suite 107 — at the corner of University and Whitfield. From this central location, we serve patients throughout the region, including Bradenton, Lakewood Ranch, Palmetto, Parrish, Venice, Osprey, Nokomis, Ellenton, Ruskin, Myakka City, North Port, and the greater Tampa Bay area. Patients also travel from St. Pete, Riverview, and Manatee County to receive specialized upper cervical care here.
Carpal tunnel syndrome is one of the most common reasons people seek help for hand and arm symptoms, and many patients have been treated only at the wrist without anyone considering whether the neck is part of the picture. If you have had carpal tunnel treatment that did not fully resolve your symptoms, or you want a comprehensive evaluation that considers the whole nerve pathway, we encourage you to reach out for an honest assessment.
Top 15 FAQs About Carpal Tunnel Syndrome and Upper Cervical Chiropractic Care
1. Can upper cervical chiropractic cure carpal tunnel syndrome? We want to be honest: upper cervical care does not open the carpal tunnel at the wrist, and for purely wrist-level carpal tunnel it is unlikely to be the answer. What it can do is address the cervical and postural contribution to the double-crush picture, which is a meaningful part of the problem for a substantial subset of patients. For many patients, wrist-focused care is also needed.
2. What is the double-crush phenomenon? It is the principle, introduced by Upton and McComas in 1973, that a nerve compressed at one point becomes more vulnerable to symptoms from compression at a second point. For carpal tunnel, the median nerve can be compressed both at the cervical spine and at the wrist, and the two compressions can compound one another.
3. Why would my neck affect symptoms in my hand? Because the median nerve fibers originate from the cervical nerve roots (mainly C6, C7, C8) before traveling down to the wrist. Irritation of these nerve roots in the neck can, per the double-crush model, make the median nerve more susceptible to becoming symptomatic at the wrist.
4. Is the double-crush theory actually proven? It is a real and clinically meaningful phenomenon, but it is genuinely debated. Some studies show high coexistence rates of cervical and wrist compression; others argue the strict criteria for a true double crush are met far less often than the diagnosis is invoked. We present it honestly: it matters for a subset of patients, but it is not the explanation for every case.
5. Why did my carpal tunnel surgery not fully work? One documented reason is unaddressed cervical compression — roughly 30% of median nerve double-crush patients consider their carpal tunnel release a failure, often related to persistent cervical nerve compression that was never evaluated or treated. If your surgery did not fully resolve symptoms, the cervical contribution is worth evaluating.
6. How do I know if my neck is involved? Signs that suggest a cervical or double-crush component include neck pain, symptoms extending above the wrist into the forearm or arm, a history of neck problems, or carpal tunnel symptoms that have not responded to wrist-focused care. A thorough evaluation can help determine this.
7. Is upper cervical care safe for carpal tunnel patients? The Knee Chest Upper Cervical technique is exceptionally gentle, with no twisting or forceful manipulation. It is generally very safe. We perform a thorough evaluation and coordinate with other providers for the wrist-level and medical components of your care.
8. Should I still wear my wrist splint? Yes. Wrist splinting, especially at night, is one of the most effective conservative treatments for carpal tunnel syndrome and addresses the wrist-level compression directly. Upper cervical care addresses the cervical contribution — the two are complementary.
9. Do I need surgery for carpal tunnel syndrome? Many patients do not. Conservative care — splinting, activity modification, ergonomics, addressing underlying conditions, and where relevant the cervical contribution — helps many patients avoid surgery. Surgery is generally reserved for severe cases, significant nerve damage, or failure of conservative care.
10. Can diabetes cause carpal tunnel syndrome? Diabetes is a significant risk factor, as are hypothyroidism, obesity, pregnancy, and rheumatoid arthritis. Managing these underlying conditions is an important part of treating and preventing carpal tunnel syndrome.
11. Can a car accident contribute to carpal tunnel symptoms? Trauma like whiplash can injure the cervical spine and contribute to the cervical half of a double-crush picture, potentially making median nerve symptoms at the wrist worse. The whole-pathway evaluation is especially relevant for patients with a history of neck trauma.
12. Why are my symptoms worse at night? Many people sleep with their wrists flexed, which increases pressure in the carpal tunnel. This is why night splinting is so effective and why symptoms often wake patients from sleep. Sleeping posture and arm position can also play a role.
13. What is the difference between carpal tunnel and a pinched nerve in the neck? Carpal tunnel is compression of the median nerve at the wrist, producing symptoms in the thumb and first fingers. A pinched nerve in the neck (cervical radiculopathy) is compression of a nerve root in the cervical spine. They can occur separately or together — and when they occur together along the median nerve, that is the double-crush phenomenon.
14. How will I know if upper cervical care is right for me? The only way to know is a thorough evaluation. We will assess whether your cervical spine and posture are contributing to your carpal tunnel symptoms, screen for red flags, and give you an honest assessment of whether upper cervical care is likely to help — and what else you may need.
15. How do I get started? Call our Sarasota office at (941) 243-3729 or book your consultation online. We will review your history, perform a thorough examination, and give you a straight answer about how upper cervical care fits into your recovery.
Take the Next Step Toward Relief
Carpal tunnel syndrome is one of the most common conditions there is — and for many patients, conservative care helps them avoid surgery entirely. But for the substantial subset of patients whose median nerve is being compressed not only at the wrist but also at the cervical spine, treating only the wrist leaves part of the problem unaddressed. The double-crush phenomenon is real, it is documented, and it is one of the most overlooked reasons carpal tunnel treatment fails.
If you are in Sarasota, Bradenton, Lakewood Ranch, or anywhere in the surrounding region and you are dealing with carpal tunnel symptoms — especially if wrist-focused treatment has not fully resolved them — Dr. Rusty Lavender and Dr. Jacob Temple at Lavender Family Chiropractic are here to give you an honest evaluation of whether the cervical and double-crush component is part of your picture, and where upper cervical care fits into your recovery.
📞 Call (941) 243-3729 today to schedule your complimentary consultation 📅 Book online here 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield