

Ehlers-Danlos Syndrome: If you live with Ehlers-Danlos Syndrome (EDS), you already know how exhausting it can be to explain your symptoms to people who have never heard the word “zebra.” You know what it’s like to dislocate a shoulder reaching for a coffee mug, to feel your heart race the moment you stand up, to wake up feeling like you got hit by a truck even though you barely moved the day before. You’ve probably been bounced between rheumatologists, cardiologists, neurologists, GI specialists, and physical therapists — each one focused on their own slice of the problem, none of them quite able to see the whole picture.
Here in Sarasota, Florida, we meet EDS patients almost every week at Lavender Family Chiropractic. Most of them have been told that chiropractic care is “off the table” because of their tissue fragility and hypermobility — and frankly, when people are picturing the rough, twisting, popping kind of adjustments, that warning makes sense. But upper cervical chiropractic care is a completely different animal. There is no twisting. No yanking. No popping. No cracking. It is one of the gentlest, most precise forms of healthcare available, and for the EDS community, it can be a game changer.
This guide walks you through what EDS is, why the upper neck is so critical for hypermobile patients, what gentle upper cervical care actually looks like in our office, and what the current research says. If you’ve been searching for a thoughtful, evidence-informed approach that respects the realities of living in a hypermobile body, you’re in the right place.
What Is Ehlers-Danlos Syndrome?
Ehlers-Danlos Syndrome is a group of inherited connective tissue disorders. The thread that runs through all of them is the same — the body produces collagen that is structurally different from typical collagen. Since collagen is the building material for skin, ligaments, tendons, blood vessels, joint capsules, and the dura around your spinal cord, you can probably already see why EDS doesn’t stay in one lane. It touches everything.
There are thirteen recognized subtypes of EDS, but the one most patients in our office are working with is hypermobile EDS (hEDS), along with the closely related Hypermobility Spectrum Disorders (HSD). These patients tend to share a recognizable cluster of features:
Joints that move beyond their normal range — fingers that bend backward, elbows and knees that hyperextend, shoulders, jaws, and hips that slip or sublux without warning. Skin that may feel soft, stretchy, or velvety, and that bruises easily or scars poorly. A near-constant background of pain that doesn’t always match what imaging shows. Profound fatigue. And a long list of seemingly unrelated symptoms — headaches, dizziness, racing heart, GI problems, brain fog, anxiety — that other doctors have a hard time tying together.
If you’ve been told you have “loose joints,” “double-jointedness,” or that your symptoms are “in your head,” and yet you know in your bones that something more is going on, EDS or HSD may be part of the story. Getting an accurate diagnosis matters, because it changes everything about how your body should be approached — including what kind of chiropractic care is safe and appropriate.
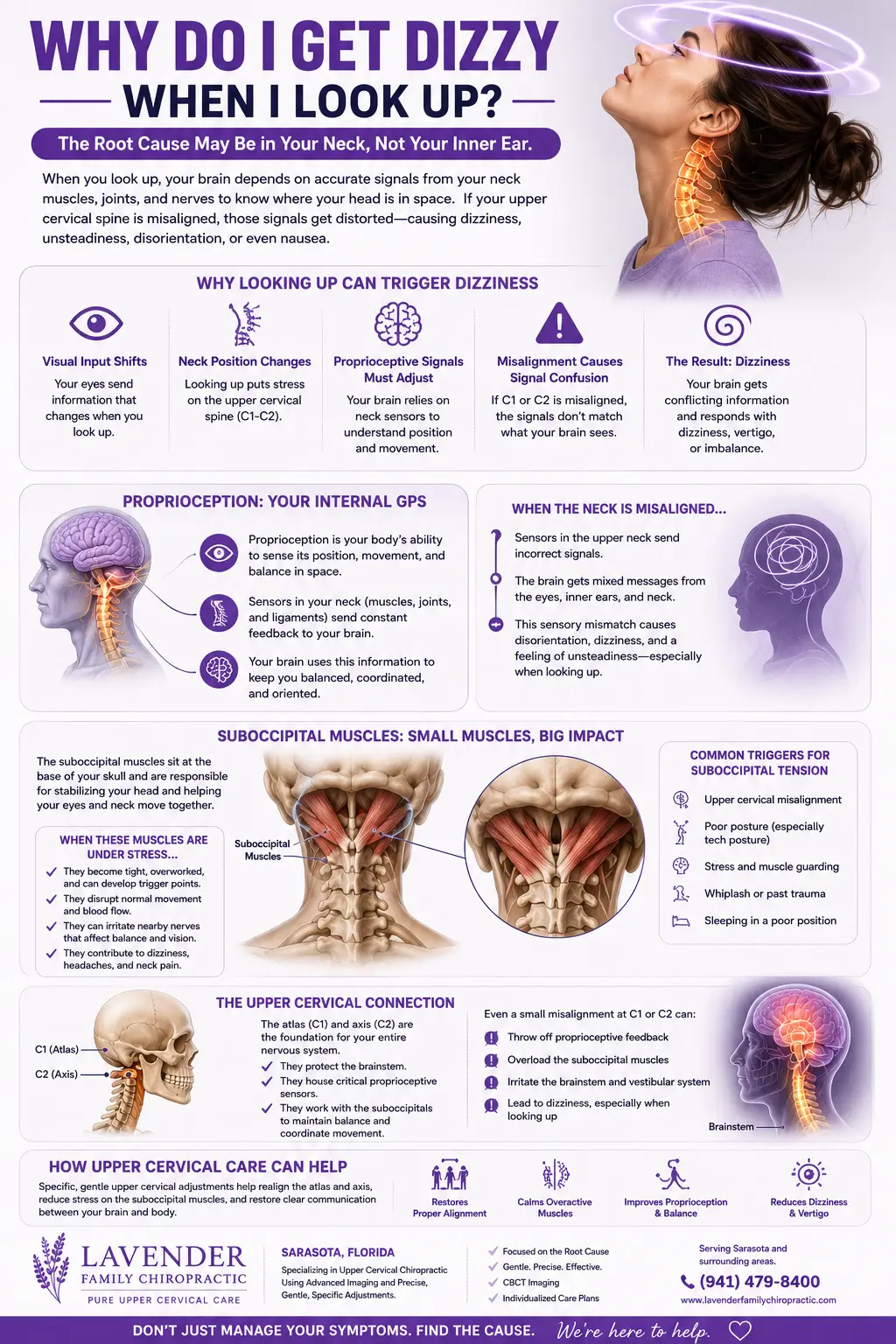
Why the Upper Neck Matters So Much for EDS Patients
To understand why upper cervical chiropractic can have such a powerful impact for EDS, you have to understand the unique real estate at the top of the spine.
The atlas (C1) is the very first vertebra of the neck. It sits directly under the skull and supports the entire weight of the head. The axis (C2) sits right below it. Together, these two bones form the craniocervical junction — the place where your head meets your spine. Unlike the rest of the vertebrae, the atlas has no disc above or below it. It is held in position almost entirely by ligaments.
That is where things get interesting for EDS patients. If the ligaments holding the atlas in place are made of more elastic, more stretchable collagen, those upper neck bones can drift out of position more easily and stay there. Even subtle misalignments at C1 and C2 can have outsized consequences, because of what is housed in that exact area.
A neurological pressure point
Running directly through the atlas and axis is the brainstem — the lower part of the brain that controls breathing, heart rate, blood pressure, digestion, balance, swallowing, sleep regulation, and the body’s stress response. The vagus nerve, which is the master conductor of your parasympathetic (“rest and digest”) nervous system, exits the skull right in this region. The spinal cord, the trigeminal nerve nuclei that influence facial and head pain, and the vestibular pathways that govern balance and spatial orientation all converge here.
When the upper neck is misaligned in someone with EDS, the consequences are rarely limited to neck pain. Patients often report the cascade of symptoms we’ll discuss below — and many of them tie back to one common thread: irritation of the brainstem and the nerves that pass through this small but mighty area.
A vascular highway
The upper cervical spine is also a major vascular highway. The vertebral arteries pass up through the bones of the upper neck before joining at the base of the brain. Cerebrospinal fluid — the clear fluid that bathes your brain and spinal cord — also moves through this region. When the atlas is shifted, blood flow to the brain and CSF dynamics can be subtly disrupted, contributing to migraines, fogginess, fatigue, and pressure sensations many EDS patients describe.
For these reasons, the upper cervical spine is one of the most clinically important regions in the body for someone with hypermobile EDS or HSD. And it’s exactly the area we specialize in at Lavender Family Chiropractic.
Upper Cervical Chiropractic Care: Gentle, Precise, and Built for Fragile Bodies
If you have EDS, you’ve probably had at least one bad chiropractic experience — or you’ve been warned away from chiropractic care entirely. We understand why. Forceful, twisting, popping adjustments can be a poor fit for hypermobile patients. The last thing anyone with stretchy ligaments needs is more stretch.
Upper cervical chiropractic is not that. It is a separate discipline, with its own training, its own diagnostic technology, and its own technique.
Here’s what makes our approach so different — and why it tends to be such a good fit for the EDS community:
No twisting. No yanking. No popping. There is no rotation of the head. There is no thrust to the neck. There is no crack. The adjustment itself is a light, specific contact that most patients describe as feeling like nothing more than a gentle touch.
Precision down to fractions of a millimeter. Before a single correction is made, we use 3D CBCT (Cone Beam Computed Tomography) imaging to map out the exact position of your atlas and axis. This is not a guess. We can measure misalignment down to the hundredth of a millimeter and calculate a correction formula that is specific to your spine.
Low force. Where traditional chiropractic relies on a high-velocity, low-amplitude thrust, our knee-chest upper cervical technique uses a very small, low-force input. For fragile connective tissue, this is enormous. Case reports and clinical literature on EDS consistently recommend low-force adjusting techniques over forceful manipulation specifically because of tissue fragility concerns.
Specific, not generalized. Most chiropractic adjustments target multiple joints at once. Upper cervical care targets one specific misalignment at the top of the spine — the one we’ve verified on imaging — and leaves the rest of the spine to respond and rebalance on its own.
For hypermobile patients especially, this combination of precision, gentleness, and specificity is what makes the difference between a treatment that triggers a flare and a treatment that quiets the nervous system down.
What to Expect at Your First Visit
We know that walking into a new office, especially for an EDS patient who has been burned before, can feel like a leap. So here is exactly what your first visit looks like at Lavender Family Chiropractic.
You’ll begin with a detailed health history. We want to hear the whole story — your diagnoses, your symptoms, your past injuries, your dislocations, your medications, what’s worked, what hasn’t, and what you’re hoping for. We treat EDS patients as the experts on their own bodies.
From there, we move into a functional nervous system assessment. We use paraspinal infrared thermography (the Tytron system) to look for patterns of nerve interference along your spine. This is non-invasive — you just sit still while the scanner reads your skin’s surface temperature pattern. We pair this with postural analysis and orthopedic and neurological exams.
If you are a candidate for care, we’ll take a 3D CBCT scan of your upper cervical spine. This gives us the precise three-dimensional view of your atlas and axis we need to design your correction. We then sit down with you in a Report of Findings visit to walk through exactly what we see, what your nervous system is telling us, and whether (and how) we think we can help. There is no high-pressure sell. If you’re not a fit, we tell you that, too.
When we do begin care, your first correction is gentle, specific, and based directly on your imaging. Many EDS patients are surprised by how subtle the actual adjustment feels — and even more surprised by how the body responds in the hours and days afterward.
How Upper Cervical Care Can Help the Many Faces of EDS
Most EDS patients aren’t dealing with just one thing. They are dealing with eight or ten things at once, all of them feeding each other. Below are the symptoms and comorbidities we see most often in EDS patients in our Sarasota office, and how upper cervical care can support each one.
Headaches and Migraines
Headaches are one of the most common complaints in EDS. They show up as cervicogenic headaches, tension headaches, classic migraines, occipital neuralgia, and pressure-type headaches that feel like a vise around the head. The trigeminal nerve nuclei sit right in the upper cervical area, and irritation there can refer pain into the face, eyes, temples, and forehead. Restoring atlas alignment often reduces both the frequency and intensity of head pain for our patients — sometimes dramatically.
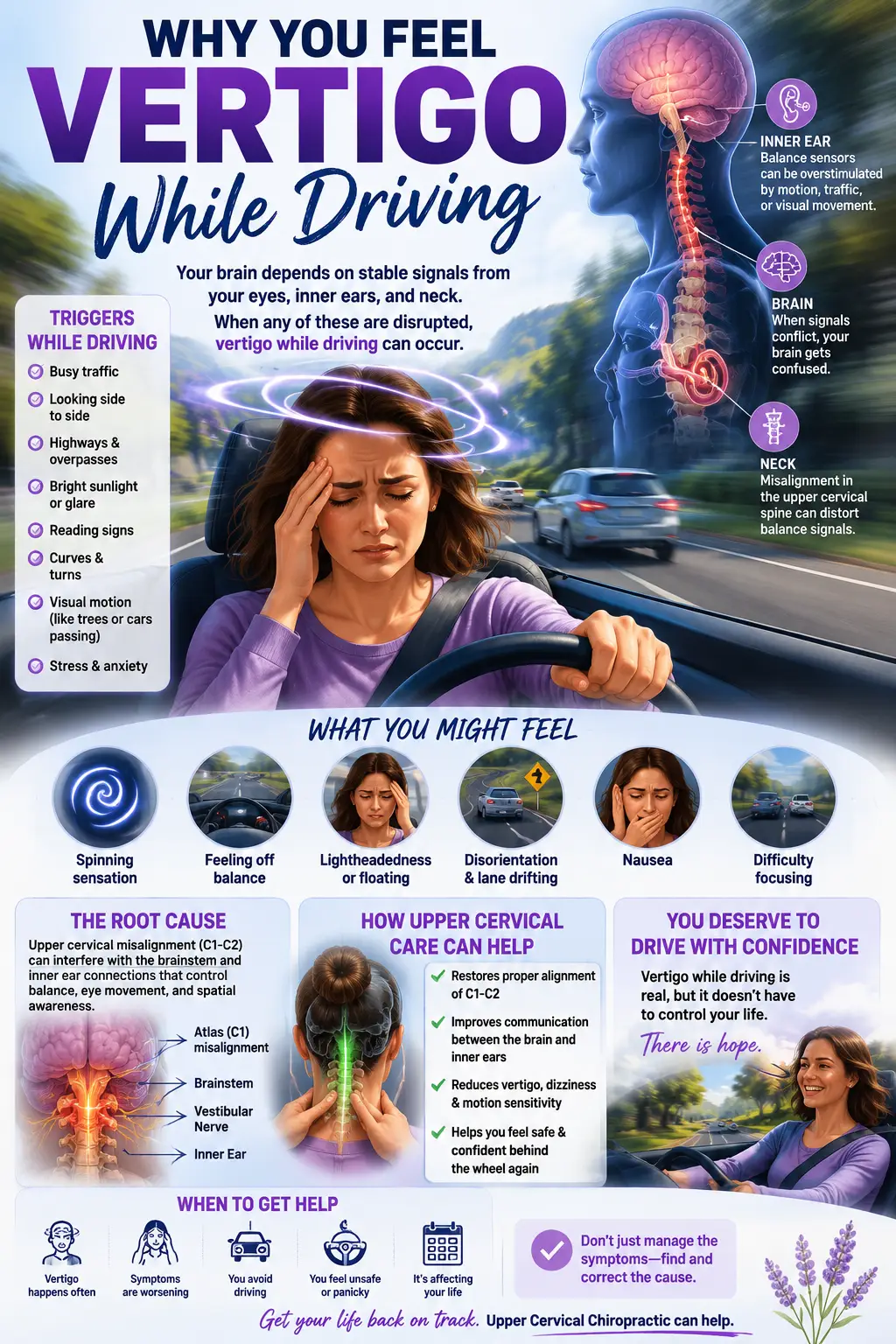
Vertigo, Dizziness, and Imbalance
The vestibular system depends on accurate input from the inner ears, the eyes, and the proprioceptors in the upper neck. When the atlas is shifted, the neck sends scrambled information to the brain, creating a sensory mismatch. The result is dizziness, spinning, fogginess, motion intolerance, and that “rocking on a boat” feeling many EDS patients describe. Correcting the upper cervical misalignment often calms the entire vestibular system down.
POTS and Dysautonomia
Postural Orthostatic Tachycardia Syndrome is one of the most common comorbidities of hypermobile EDS. Stand up, heart races, blood pools in the lower body, lightheadedness sets in, brain fog rolls in like weather. POTS is a disorder of the autonomic nervous system — and the autonomic nervous system is conducted, in large part, through the brainstem. By taking pressure off the brainstem and supporting vagal tone, upper cervical care can help the autonomic system find a steadier rhythm. Many of our POTS patients report being able to stand longer, think more clearly, and tolerate heat better as care progresses.
Fibromyalgia and Widespread Pain
Fibromyalgia and EDS overlap so often that some researchers wonder whether some “fibromyalgia” diagnoses are actually undiagnosed hEDS. Either way, central sensitization — the nervous system turning the volume up on pain signals — is the engine driving the misery. The upper cervical spine plays a major role in modulating that sensitization. When we get the brainstem out of distress, the pain dial often turns down.
Brain Fog and Cognitive Symptoms
EDS patients often describe a heavy, foggy, slow-thinking quality that no amount of sleep seems to fix. This is partly autonomic (POTS reduces blood flow to the brain when upright) and partly inflammatory. Upper cervical correction supports better cerebrospinal fluid flow and cerebral blood flow, and many patients report noticeably clearer thinking within weeks of starting care.
TMJ and Jaw Issues
Hypermobile jaws are common in EDS — clicking, locking, subluxing, popping out of place. The TMJ is intricately linked to the upper cervical spine through shared muscular and neurological connections. When the atlas is misaligned, the jaw compensates. Atlas correction often relieves jaw tension and pain in EDS patients without anyone ever touching the jaw directly.
Anxiety, Panic, and Nervous System Overload
This one isn’t always discussed openly, but it is real. When the brainstem is under chronic stress, the sympathetic nervous system runs hot. Patients live in a low-grade fight-or-flight state — wired, jumpy, easily overwhelmed, struggling to sleep. Restoring upper cervical alignment can support a parasympathetic shift, helping the nervous system finally power down.
Digestive Issues
Bloating, slow motility, reflux, nausea, and the dreaded IBS picture are extremely common in EDS. The vagus nerve, which controls most of digestion, exits right at the base of the skull. Upper cervical care supports vagal tone, and many EDS patients notice digestion calming, motility improving, and reflux easing as their nervous system stabilizes.
Chronic Fatigue
The fatigue of EDS isn’t ordinary tiredness — it’s a heavy, full-body exhaustion. It’s the cumulative cost of running a nervous system in constant overdrive. As the brainstem gets less irritated and autonomic balance improves, energy often follows.
Neck and Back Pain
EDS patients frequently have abnormal spinal curvatures, instability, and tissue strain. While we don’t try to “force” the spine into alignment, supporting the very top of the chain — where the head sits on the neck — often allows the rest of the spine to relax into a better position over time.
Tired of trying everything and feeling like nothing fits a hypermobile body? Upper cervical chiropractic at Lavender Family Chiropractic was built for patients exactly like you. To learn more about our specific technique, see our Upper Cervical Chiropractic Care page, or read Why Upper Cervical to understand what makes this approach so different.
What the Research Says
This is the part where we have to be honest with you: large-scale, randomized controlled trials on upper cervical chiropractic care for EDS specifically do not yet exist. EDS is still a relatively under-researched condition across the board. But the research that does exist — both on EDS and the upper cervical spine, and on low-force chiropractic care for hypermobile patients — points in a consistent and encouraging direction.
The most important paper for our community is the 2023 international expert consensus on upper cervical instability in hypermobile patients, published in Frontiers in Medicine by Russek and colleagues. This consensus statement, available on PubMed, was put together by an international panel of experts in physical therapy, medicine, and rehabilitation.
Their core conclusion is striking: experts in symptomatic generalized joint hypermobility agree that upper cervical instability needs to be better recognized in this population, which commonly presents as hypermobility spectrum disorder and hypermobile Ehlers-Danlos syndrome. They note that while mild upper cervical instability may be common in this group and still impactful, severe cases can be debilitating, and that the field has historically lacked consistent ways to screen, classify, and manage this issue. PubMed
In other words: top international experts are openly acknowledging that the upper neck deserves dramatically more attention in EDS care than it has historically received. You can read the full PubMed citation here: Russek et al., “Presentation and physical therapy management of upper cervical instability in patients with symptomatic generalized joint hypermobility: International expert consensus recommendations,” Frontiers in Medicine, 2023 (PMID 36743665).
Earlier case-based literature in chiropractic supports the same conclusion. A landmark 2003 paper in the Journal of Manipulative and Physiological Therapeutics on chiropractic management of EDS concluded that chiropractic care may be of benefit to some patients with connective tissue disorders, including Ehlers-Danlos syndrome, and that low-force chiropractic adjusting techniques may be a preferred technique of choice in patients with tissue fragility, offering a viable alternative to traditional chiropractic care in attempting to minimize risks and side effects. More recent case reports in the Journal of Contemporary Chiropractic have continued to show favorable outcomes for EDS patients receiving gentle, low-force, instrument-assisted, and drop-style adjustments rather than rotational manipulation. PubMed
The common thread in the literature is the same thread that runs through our office: hypermobile patients do best with gentle, precise, low-force care focused on the upper cervical spine — exactly what upper cervical chiropractic is designed to deliver.
Supporting Your EDS Body Outside the Office
Care at Lavender Family Chiropractic is one piece of a bigger picture. To get the most out of upper cervical work as an EDS patient, we encourage a few lifestyle anchors:
Pace yourself. Push-crash cycles are the enemy of EDS recovery. Build steady, gentle activity rather than swinging between overdoing it and being bedbound.
Hydrate aggressively. POTS and dysautonomia respond strongly to fluid and electrolyte intake. Most EDS patients need more salt and water than the general population, not less.
Strengthen, don’t stretch. Hypermobile bodies do not need more flexibility. They need stability. Low-impact strengthening — isometrics, resistance bands, swimming, gentle Pilates — protects joints far better than aggressive stretching, which can actually destabilize you further.
Protect the upper neck. Avoid forceful manipulation, aggressive head-and-neck stretches, and rough massage in this area. Sleep with appropriate neck support. If you’ve had an atlas correction, follow your post-care guidance carefully so the correction can hold.
Sleep is medicine. EDS recovery happens during sleep. Prioritize it ruthlessly.
If you’d like more on these concepts, our blog How to Resolve Dysautonomia: Real Answers and Proven Results from Upper Cervical Chiropractors in Sarasota goes deep on the lifestyle and nervous-system side of EDS-related autonomic issues.
Serving Sarasota and the Surrounding Communities
Lavender Family Chiropractic is located at 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243, right at the corner of University and Whitfield. We’re easy to find, easy to park at, and easy to get to from across the region.
We’re proud to care for EDS, POTS, and complex chronic condition patients from throughout the area, including Sarasota, Bradenton, Lakewood Ranch, Parrish, Ellenton, Venice, Osprey, Punta Gorda, St. Petersburg, Siesta Key, Longboat Key, Lido Key, Myakka City, and beyond. Many of our patients drive an hour or more each way because they simply cannot find this kind of gentle, specific, upper cervical care closer to home — and they tell us the trip is worth it.
For more on our team, our diagnostics, and our philosophy of care, visit our Home page.
Top 15 Frequently Asked Questions About EDS and Upper Cervical Chiropractic Care
Is chiropractic care safe if I have Ehlers-Danlos Syndrome?
Traditional, forceful, rotational chiropractic adjustments are generally not the best fit for EDS patients because of tissue fragility and joint hypermobility. However, gentle, low-force, upper cervical chiropractic care — which involves no twisting, popping, or yanking — is designed precisely for fragile, hypermobile bodies and is widely considered a safer option. Always work with a chiropractor experienced in upper cervical technique and familiar with hypermobility.
Will the adjustment hurt or pop my neck?
No. There is no cracking, popping, twisting, or thrusting in upper cervical chiropractic. The correction is a light, specific contact based on your imaging. Most patients describe it as gentler than they expected.
How do you know exactly where to adjust?
We use 3D CBCT imaging to measure your atlas and axis position down to the hundredth of a millimeter. From there we calculate a precise correction formula that is unique to you. There is no guessing.
Can upper cervical care help my migraines?
Migraines are one of the most common conditions we see — and one of the most responsive. Many EDS patients with chronic migraines report significant reductions in frequency and intensity once their upper cervical alignment is corrected.
What about my POTS symptoms?
POTS is closely tied to autonomic nervous system function, which is controlled in large part through the brainstem. By taking pressure off the brainstem and supporting vagal tone, upper cervical care often helps POTS patients tolerate standing longer and experience fewer symptom spikes.
Can this help my fibromyalgia?
Yes. Fibromyalgia involves a sensitized nervous system, and the upper cervical spine plays a major role in modulating that sensitization. Many patients with fibromyalgia and EDS notice reduced overall pain, better sleep, and improved energy with care.
Will I feel worse before I feel better?
Some patients have a brief adjustment period where the body recalibrates — mild fatigue, a temporary symptom shift, or a need for extra rest after the first few corrections. This usually settles quickly. We coach you through what to expect.
How often will I need to come in?
EDS patients typically need a structured initial phase of care to allow the correction to hold, followed by less frequent visits as the body stabilizes. We design every plan around your imaging, your symptoms, and how your body responds — not a one-size-fits-all schedule.
Can you cure my EDS?
No. EDS is a genetic condition and has no cure. What we can do is reduce nervous system interference, improve autonomic function, and help your body manage the symptoms of EDS far more effectively. Most patients report a meaningful improvement in quality of life.
Is upper cervical care safe if I have craniocervical instability (CCI)?
This depends on the severity of your CCI and your individual case. We screen carefully for signs of significant instability, review imaging, and refer out when surgical consultation is appropriate. For mild to moderate upper cervical instability, gentle low-force care can often be supportive rather than harmful — but it must be done thoughtfully, by a doctor who understands the condition.
Can I bring my imaging from a previous provider?
Yes. We welcome outside MRI, CT, and X-ray imaging and will review it as part of your evaluation. We may still recommend our own 3D CBCT if a more precise upper cervical view is needed for treatment planning.
Is the office accessible if I have mobility limitations or pain flares?
Yes. Our office is single-story, easy to access, and our team is experienced in working with patients who have significant pain, fatigue, and mobility considerations. We move at your pace.
Do you treat children with EDS?
Yes. Upper cervical care is gentle enough for pediatric patients, and many hypermobile kids benefit significantly. We adapt every aspect of the visit to be child-friendly and trauma-informed.
How long until I notice changes?
Some patients feel changes within the first few visits. For more chronic, complex EDS cases, meaningful improvement often unfolds over several weeks to months. Healing is rarely a straight line — but for most of our patients, the trend is steady, real, and lasting.
Do you take insurance?
We work with patients on a variety of payment options and can talk you through specifics on a complimentary consultation. We never want financial barriers to keep you from finding out whether this care could change your life.
Ready to Take the Next Step?
If you’ve been living with EDS and feel like every door you’ve knocked on has led to another dead end, we want you to know there is another path. A gentle one. A precise one. A patient one. A path that respects your body’s fragility while still moving you forward.
At Lavender Family Chiropractic, our doctors — Dr. Rusty Lavender and Dr. Jacob Temple — have spent thousands of hours mastering specific upper cervical technique because we believe that when the nervous system is finally allowed to function the way it was designed to, healing becomes possible. Even for the most complex, layered, “I’ve-been-to-everyone” cases.
We would be honored to listen to your story.
Call our Sarasota office today at (941) 243-3729 or book your complimentary consultation online. We’ll sit down with you, hear what you’ve been through, and tell you honestly whether we think we can help.
You don’t have to keep doing this alone.
Related Articles
- POTS Doctor Sarasota – Our #1 Proven Approach for POTS at Lavender Family Chiropractic
- Fibromyalgia Doctor Lakewood Ranch – How Lavender Family Chiropractic Helps Restore Quality of Life Through Upper Cervical Care
- How to Resolve Dysautonomia: Real Answers and Proven Results from Upper Cervical Chiropractors in Sarasota
By the team at Lavender Family Chiropractic- Dr. Rusty Lavender and Dr. Jacob Temple — Sarasota, Florida
Related Posts
Popular Posts
