
By Dr. Rusty Lavender and Dr. Jacob Temple
Cervical Spondylosis Relief in Sarasota: Maybe your doctor showed you an X-ray and used the words “wear and tear,” “degeneration,” or “arthritis in your neck.” Maybe you have been told you have bone spurs, narrowed disc spaces, or “a neck older than your years.” For many people, that conversation lands hard. It sounds permanent, like the structure of your neck is simply breaking down and there is nothing to do but manage the pain. The stiffness that greets you in the morning, the deep ache after a long day, the grinding sensation when you turn your head, the occasional pain that radiates into your shoulder, all of it suddenly has a name that sounds like a slow, one-way decline.
If you are in Sarasota, Bradenton, Lakewood Ranch, or anywhere along the Gulf Coast and you have been told you have cervical spondylosis, here is the most important thing to understand from the start: the presence of degenerative changes on your imaging is extraordinarily common, it is a normal part of aging, and it correlates surprisingly poorly with how much pain a person actually has. Many people with significant degeneration on their scans have no symptoms at all, and many people with painful, stiff necks have only modest changes on imaging. The degeneration is real, but it is rarely the whole story, and the parts of the story you can actually influence, how your cervical spine is loaded and aligned, are often the parts that matter most for how you feel.
At Lavender Family Chiropractic in Sarasota, our entire focus is the upper cervical spine, the atlas (C1) and axis (C2) at the very top of the neck. We use 3D CBCT imaging and paraspinal infrared thermography to find the subtle misalignments that change how the joints and discs below them are loaded, and we correct them with the gentle, precise Knee Chest Upper Cervical technique, with no twisting, popping, or forceful cranking on a degenerating, sensitive spine. This guide will explain what cervical spondylosis actually is, why it develops, why the upper cervical spine plays such an important role in how fast it progresses and how much it hurts, what the research honestly says about conservative care, and what you can do to both calm your symptoms and protect your neck for the years ahead.
What Is Cervical Spondylosis?
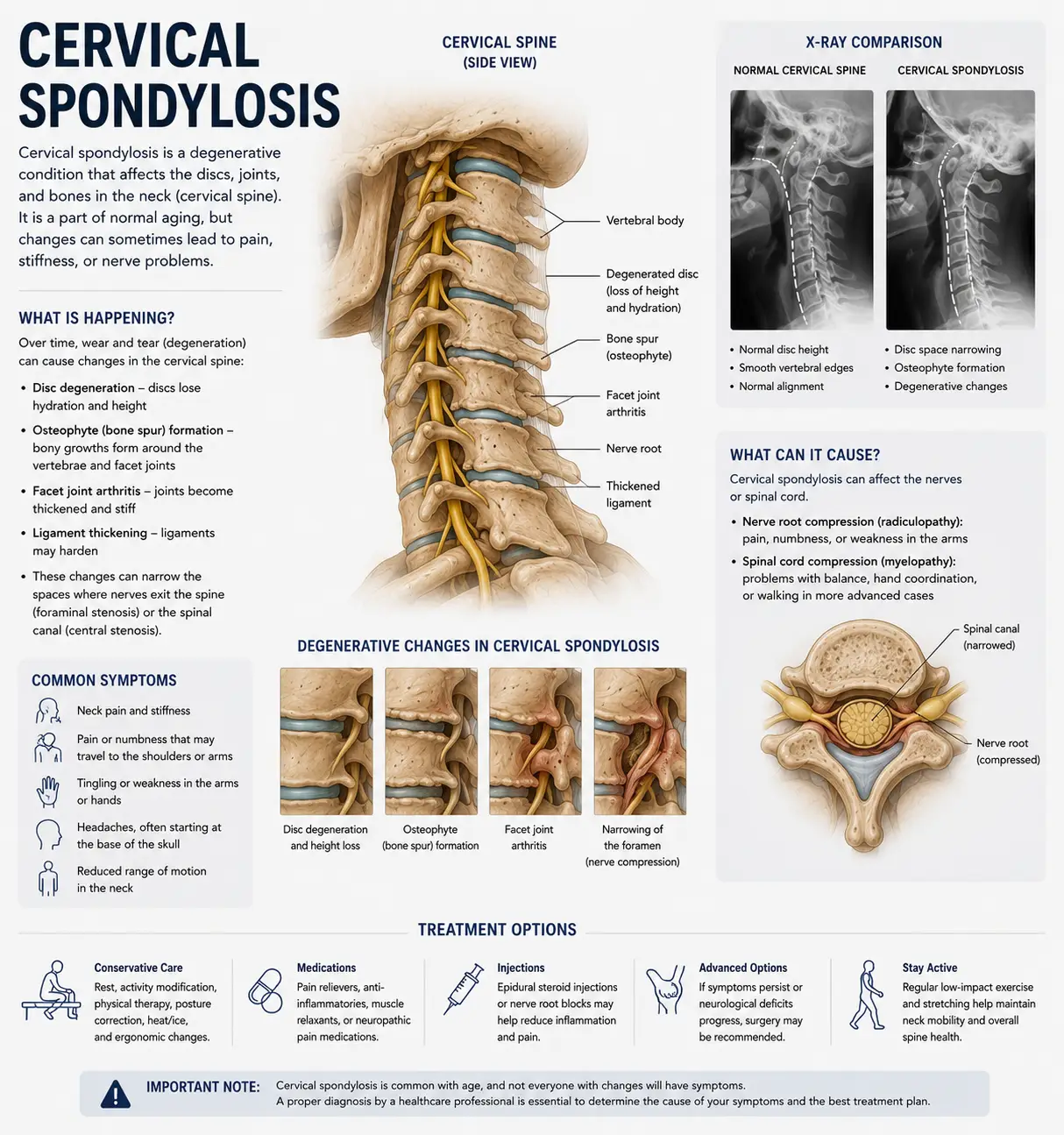
Cervical spondylosis is the medical term for age-related degeneration of the cervical spine. It is not a single injury or a discrete disease but a gradual, cumulative process that affects all the structures of the neck over time: the intervertebral discs, the facet joints, the uncovertebral joints, the ligaments, and the vertebral bodies themselves. It is often used interchangeably with terms like cervical osteoarthritis, neck arthritis, or degenerative disc disease of the neck.
According to Physiopedia, the clinical reference resource used widely by physical therapists, spondylosis describes a generalized natural aging process involving a sequence of degenerative changes in spinal structure, affecting the intervertebral discs and facet joints, and potentially progressing to disc herniation, osteophyte (bone spur) formation, vertebral body degeneration, and in some cases compression of the spinal cord. The same resource notes that while aging is the primary cause, the location, rate, and symptomatic impact of the degeneration vary enormously from one person to the next.
The cascade usually begins with the discs. The intervertebral discs are the cushions between your vertebrae, and they are roughly 80% water. As we age, they gradually lose water content and height. As a disc loses height, the space between two vertebrae narrows, which transfers more load to the facet joints at the back of the spine, changes the way the joints track, and can prompt the body to lay down bone spurs around the joint margins in an attempt to stabilize the segment. Those bone spurs, along with the narrowed spaces, can encroach on the openings where nerve roots exit, which is how spondylosis sometimes produces radiating arm symptoms. Cervical spondylosis is therefore best understood not as a single problem but as an interconnected chain of changes, each one influencing the next.
Clinically, the symptoms of cervical spondylosis sort into three broad patterns. A review published in PMC on the natural history and clinical syndromes of degenerative cervical spondylosis describes how symptoms can be categorized broadly into three clinical syndromes: axial neck pain, cervical radiculopathy, and cervical myelopathy, with patients commonly having a combination of these, and the majority of symptomatic patients presenting between the ages of 40 and 60. Axial neck pain is the most common, the deep, aching, stiff neck pain felt locally. Radiculopathy is nerve-root irritation producing arm symptoms. Myelopathy, the least common but most serious, involves the spinal cord itself and requires careful medical evaluation. Most people with cervical spondylosis have the first pattern, axial neck pain and stiffness, without nerve or cord involvement.
How Common Is It, Really?
This is where the picture becomes genuinely reassuring, because the prevalence numbers reframe the entire conversation. Degenerative change in the cervical spine is not a sign that something has gone uniquely wrong with you. It is close to universal with age.
According to StatPearls, the peer-reviewed clinical reference, radiographic studies frequently demonstrate spondylotic changes in the cervical spine, yet the majority of affected individuals remain asymptomatic, with these changes present in approximately 25% of individuals younger than 40, 50% of those older than 40, and up to 85% of individuals beyond a certain age. Read that again: up to 85% of older adults show these changes, and most of them have no symptoms. A large radiographic study of 1,581 patients aged 18 to 97, published in the European Spine Journal, found that 53.9% of individuals had radiographic disc degeneration, with the C5/C6 level the most commonly affected.
The clinical significance of this is enormous, and it is something we want every patient to understand. Because degenerative changes are so common in people without any pain, the changes on your X-ray or MRI cannot, by themselves, explain your pain. Imaging findings and symptoms correlate poorly. This is liberating news, because it means your pain is not simply a direct readout of how “worn out” your neck looks on a scan. There are other factors, how your spine is loaded, how it is aligned, how the surrounding muscles are functioning, how inflamed the tissues are, that determine whether a degenerating neck hurts or not. And many of those factors can be influenced.
What Causes Cervical Spondylosis to Progress and Become Painful?
If degeneration is a normal aging process, why do some people develop painful, rapidly progressing spondylosis while others age into their seventies with comfortable, mobile necks? The answer comes down to load. The rate at which a cervical spine degenerates, and whether it becomes painful, is heavily influenced by how it is mechanically stressed over the years.
The primary driver is cumulative mechanical load, particularly uneven or excessive load. Discs and joints that are loaded evenly and within their healthy range tend to age slowly and gracefully. Discs and joints that are chronically overloaded, or loaded asymmetrically, wear faster. This is why occupational factors matter: jobs involving prolonged neck flexion, frequent overhead work, or heavy loading of the upper body are associated with higher rates of significant cervical spondylosis.
In the modern world, the single most pervasive source of excess cervical load is sustained forward head posture, the pattern so common from phones, tablets, and laptops that it has earned the nickname tech neck. Every inch the head drifts forward of its balanced position over the shoulders dramatically multiplies the leverage and load on the lower cervical discs and joints. Hours per day in that position, year after year, is precisely the kind of sustained overload that accelerates the degenerative cascade.
Other contributors include prior trauma, especially whiplash, which can initiate or accelerate degeneration at the injured segments; genetics, since the tendency toward disc degeneration runs in families and follows similar patterns even in twins; smoking, which impairs disc nutrition and accelerates degeneration; and chronic dehydration, which the discs are especially vulnerable to. But underlying nearly all of these is the common theme of how the cervical spine is loaded and aligned over time, and that is where the upper cervical connection becomes central.
The Upper Cervical Connection: Why Alignment Determines How Your Neck Ages
Here is a question worth sitting with: why does spondylosis so often develop more on one side than the other, and why does it concentrate at particular levels like C5/C6? If aging alone were the cause, you might expect symmetric, even wear. Instead, degeneration is usually lopsided, and that asymmetry is a clue.
The answer lies in how the cervical spine functions as a single, integrated system, and in how the alignment of the atlas and axis sets the mechanical baseline for every level below them.
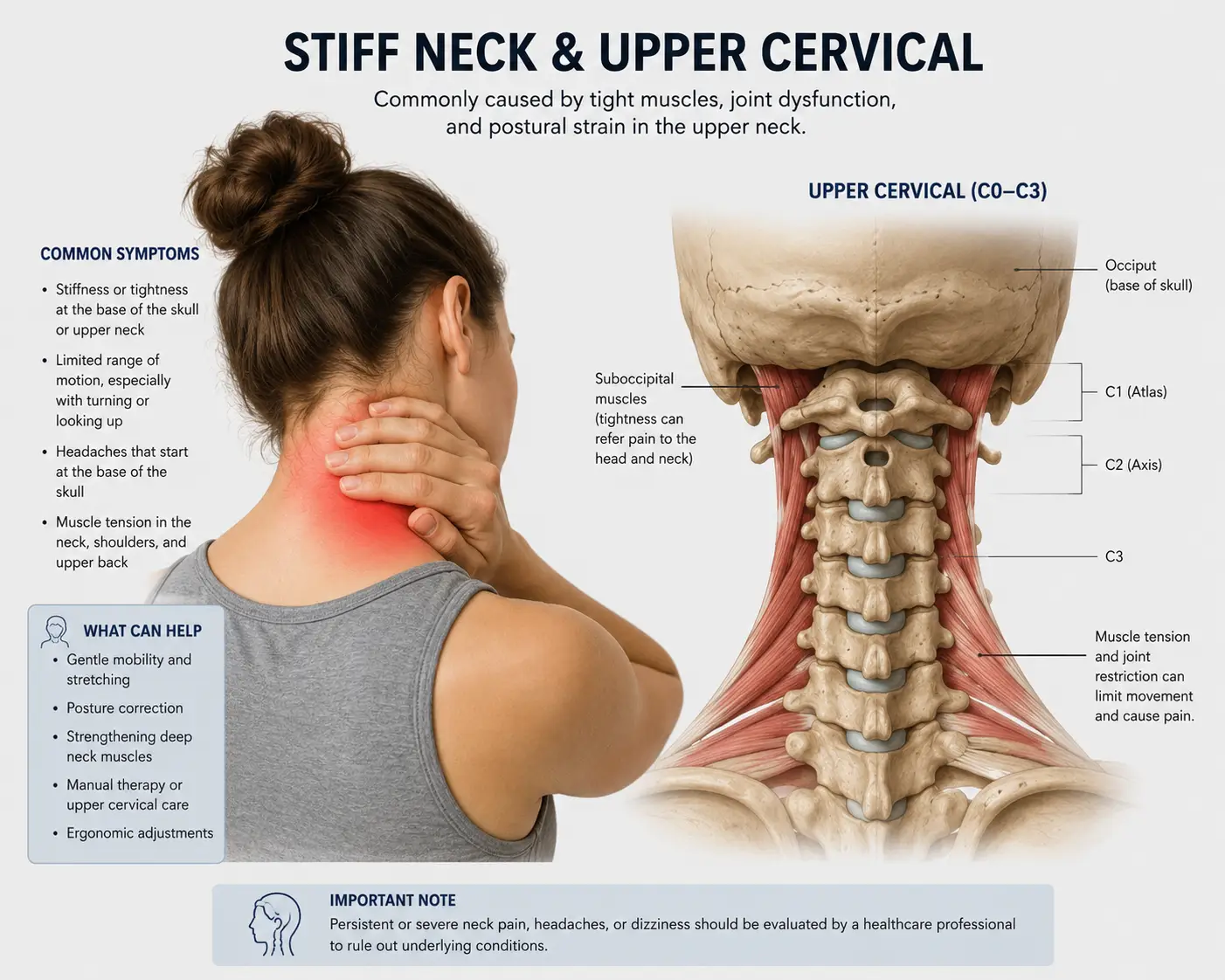
The atlas and axis form the craniocervical junction at the top of the neck, the region responsible for keeping your head level and your eyes oriented to the horizon. When the atlas sits even slightly out of position, your body cannot tolerate a tilted head, because your visual and vestibular systems demand a level gaze. So the body compensates, side-bending and rotating the vertebrae below the misalignment to bring the head back toward horizontal. Those compensations propagate downward through the lower cervical spine, the very region, especially C5/C6 and C6/C7, where spondylosis concentrates.
The consequence over time is that a chronic upper cervical misalignment forces the lower cervical discs and joints into asymmetric positions and uneven loading patterns that they were never designed to hold for decades. One side of a segment gets compressed and overworked while the other is unloaded. The overloaded discs lose height faster. The overloaded facet joints wear faster and form bone spurs preferentially. The neural openings narrow asymmetrically. This is exactly the lopsided pattern of degeneration seen so often on imaging, and it is the mechanical fingerprint of asymmetric loading driven from above.
In other words, while you cannot change your age or your genetics, the alignment of your upper cervical spine is one of the inputs that determines how quickly your lower cervical spine degenerates and whether it becomes painful. Correcting that alignment does not reverse degeneration that has already occurred, and we are careful never to claim it does. But it can change the loading pattern going forward, taking chronic, uneven stress off the segments that have been bearing more than their share, which can reduce pain, reduce the protective muscle guarding that accompanies it, and slow the rate at which further degeneration accumulates.
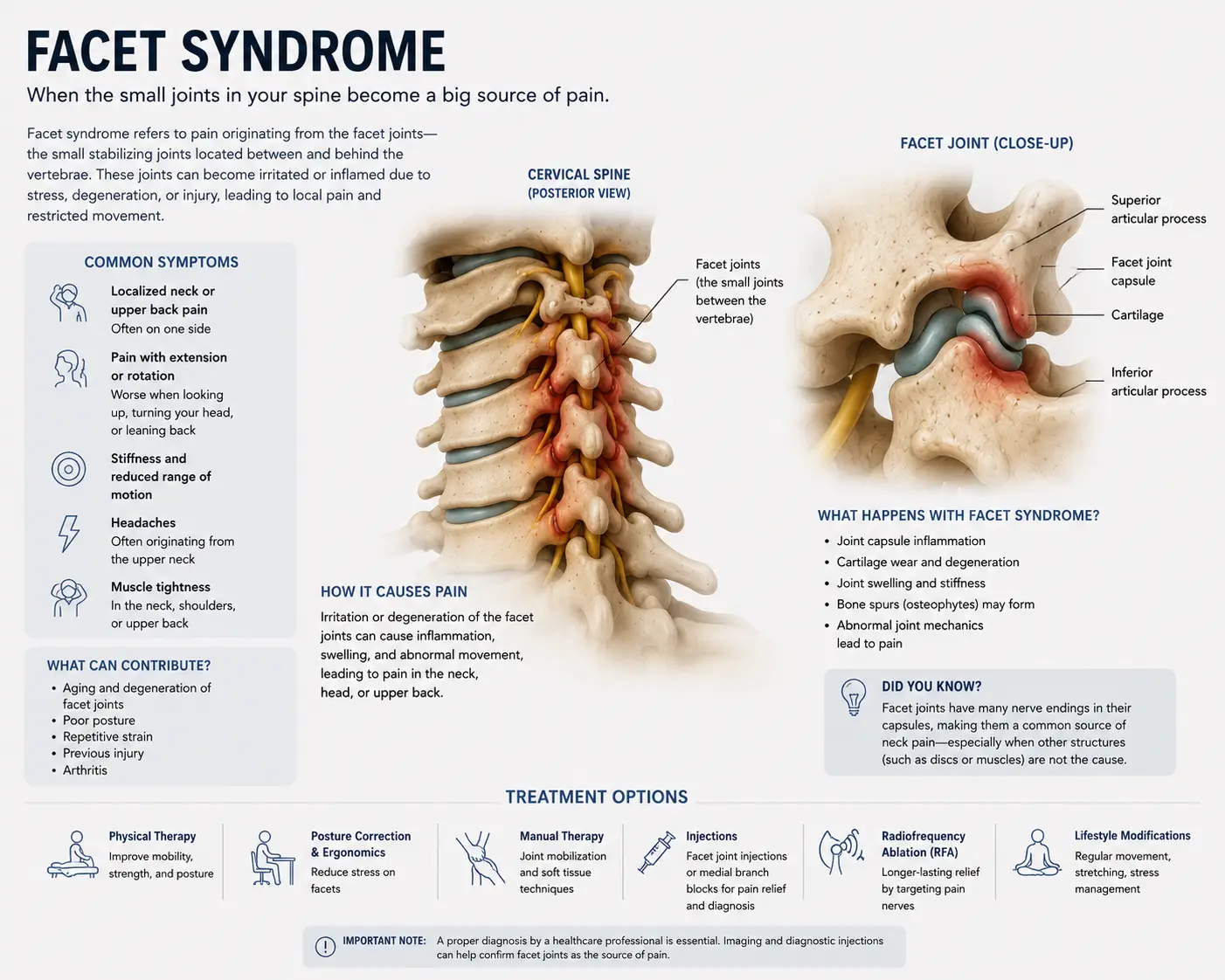
There is a second mechanism worth understanding. The atlas and axis surround the brainstem and are densely packed with the proprioceptors that tell the brain where the head and neck are in space. When upper cervical alignment is compromised, the quality of that position information degrades, muscle tone regulation becomes less precise, and the muscles around a degenerating, stiff segment guard more persistently. That guarding is itself a significant source of the pain and stiffness people attribute purely to “arthritis.” If you also find yourself with a constant urge to crack or pop your neck to relieve the stiffness, that urge is often the body trying to mobilize a stiff, guarded, degenerating segment, and it is another sign the same upper cervical pattern is in play.
Why Upper Cervical Care Matters for Cervical Spondylosis
At Lavender Family Chiropractic in Sarasota, we approach cervical spondylosis by being honest about what can and cannot change, and by focusing on the factors that genuinely move the needle. We cannot reverse degeneration that has already happened. What we can do is address the upper cervical alignment and loading pattern that influences how your neck is stressed from here forward. Through the Knee Chest Upper Cervical technique, we correct atlas and axis misalignment with a precise, gentle, sub-millimeter adjustment that requires no twisting, no cracking, and no forceful rotation of the neck. This gentleness matters greatly for spondylosis patients, because a degenerating cervical spine with bone spurs and narrowed spaces is exactly the kind of neck where aggressive, high-velocity rotational manipulation can be uncomfortable or inadvisable.
For someone with cervical spondylosis, restoring proper upper cervical alignment helps in several ways. First, it reduces the asymmetric loading that has been accelerating degeneration on the overworked side, allowing the chronically compressed segments to be loaded more evenly going forward. Second, it improves the proprioceptive input from the upper neck, which helps the nervous system dial down the protective muscle guarding that produces so much of the stiffness and aching. Third, by restoring symmetry and motion at the top of the cervical spine, it supports the deep stabilizing muscles in doing their job of controlling segmental motion, which reduces the repetitive micro-stress on already degenerating discs and joints during everyday movement.
What separates upper cervical care from a generic adjustment is the precision of the diagnosis and the specificity of the correction. We are not forcefully manipulating the degenerated, arthritic segments. We are correcting the structural foundation above them that has been shaping how they are loaded for years. This is a fundamentally different and gentler model, and it is well suited to the realities of a spondylotic spine.
The broader research on conservative care for degenerative neck conditions is encouraging. A case series published in the Journal of Orthopaedic & Sports Physical Therapy on the treatment of degenerative cervical radiculopathy in a geriatric population found that multimodal conservative approaches combining manual therapy, exercise, and traction are commonly used and supported for cervical spondylosis and cervical radicular symptoms, reflecting a broad consensus that conservative care should generally come first for degenerative neck conditions. A systematic review in PMC on manual physical therapy for cervical radiculopathy similarly concluded that manual therapy combined with therapeutic exercise is effective for increasing function and range of motion while decreasing pain and disability, with recent evidence favoring conservative treatment over surgical options for many patients.
What Care Looks Like at Lavender Family Chiropractic
If you come into our Sarasota office for evaluation related to cervical spondylosis, here is what to expect.
Your first visit begins with a thorough consultation. Dr. Lavender or Dr. Temple will sit down with you and review your full history: when your neck pain and stiffness started, how it has progressed, what makes it better or worse, whether you have arm symptoms or any neurological changes, what imaging you have had, and what you have been told. We pay particular attention to red flags. If you have signs of cervical myelopathy, the spinal-cord-involvement pattern of spondylosis, such as changes in hand coordination, balance problems, gait changes, or widespread weakness or numbness, we will tell you directly and ensure you get the appropriate medical evaluation. Myelopathy is the one pattern of spondylosis that genuinely requires careful medical and sometimes surgical attention, and screening for it is part of our responsibility. Patient safety comes before everything else.
For appropriate patients, the examination includes a careful assessment of your range of motion, a neurological screen, postural analysis, and advanced 3D CBCT imaging of your cervical spine. This level of imaging is particularly valuable for spondylosis because it lets us see the degenerative changes, disc spacing, bone spurs, foraminal narrowing, and atlas-axis alignment in three dimensions, detail far beyond what flat films provide. We also perform functional nervous system scans to objectively measure how your nervous system is operating before care begins.
If the examination reveals an upper cervical misalignment contributing to your loading pattern, we will explain our findings and recommendations honestly, including a frank conversation about what upper cervical care can realistically do for a spine with established degeneration and what it cannot. If your situation involves advanced degeneration, myelopathy, or findings that call for medical or surgical co-management, we will tell you plainly and help coordinate that care. We see ourselves as one part of your team.
For patients who are appropriate candidates, care is delivered through the gentle Knee Chest Upper Cervical technique, with no popping, twisting, or rotational force, which is particularly important for a degenerating spine. We offer customized treatment plans tailored to the severity and chronicity of your spondylosis, and we are transparent about realistic timelines and what success looks like for your particular case. With degenerative conditions, the goal is usually meaningful reduction in pain and stiffness, improved function, and a slower trajectory of further wear, rather than a cure for the degeneration itself.
📞 Call (941) 243-3729 to schedule your complimentary consultation 📅 Book your consultation online 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
What the Research Says About Cervical Spondylosis and Conservative Care
The research on cervical spondylosis carries two clear and honest messages: degenerative change is nearly universal with age and correlates poorly with symptoms, and conservative care should generally be the first line of management for the great majority of symptomatic cases.
On prevalence and the imaging-symptom disconnect, the evidence is striking. StatPearls documents that spondylotic changes are present in roughly 25% of people under 40, 50% over 40, and up to 85% of older individuals, with the majority remaining asymptomatic. The European Spine Journal radiographic study of nearly 1,600 patients found disc degeneration in 53.9%, concentrated at C5/C6. Physiopedia underscores that most features of degenerative disease are found in asymptomatic people and correlate poorly with clinical symptoms. The practical takeaway for patients is that a scary-looking scan does not doom you to pain, and treating the modifiable factors matters more than the static picture of degeneration.
On management, the consensus favors conservative care first. The PMC review on the natural history of degenerative cervical spondylosis describes the three clinical syndromes and notes that most axial neck pain and radiculopathy are managed non-surgically, with surgery reserved primarily for myelopathy or refractory, progressive cases. The JOSPT case series on geriatric degenerative cervical radiculopathy supports multimodal conservative care combining manual therapy, exercise, and traction, and the PMC systematic review on manual physical therapy concludes that manual therapy plus exercise effectively improves function and range of motion while reducing pain and disability.
It is worth being honest about the limits of this evidence as it applies to upper cervical care specifically. Much of the high-quality research studies general manual therapy, exercise, and physical therapy for degenerative neck conditions rather than upper cervical correction in particular. We think it reads as more credible, not less, to state plainly that the prevalence and imaging-disconnect data are very well established, while the treatment evidence for conservative manual care is solid for the general approach and still developing for upper cervical correction specifically. What the literature clearly supports is acting conservatively first, addressing the modifiable mechanical and lifestyle factors, and reserving surgery for the minority of cases that genuinely require it.
Lifestyle Factors That Protect Your Neck and Slow Degeneration
Whether or not upper cervical care is part of your plan, the daily inputs you control have an outsized effect on how your spondylosis feels and how fast it progresses. With a degenerative condition, these habits are not optional extras, they are central to protecting your neck for the long run.
Screen ergonomics. This is the most important modifiable factor for most people. Sustained forward head posture from devices dramatically increases the load on the lower cervical discs and joints, accelerating degeneration. Bring screens to eye level, and break up long stretches of looking down with frequent movement.
Stay gently active. Degenerating joints depend on movement for their health, and total inactivity stiffens them and worsens pain. Regular, gentle, pain-respecting movement, walking, mobility work, and appropriate strengthening, supports circulation, maintains range of motion, and helps the supporting muscles protect the degenerating segments. Stay active within your comfortable range.
Build supporting strength. Once you are past acute flares, gradually strengthening the deep neck flexors and the muscles of the upper back and shoulder girdle helps support the cervical spine and reduce the load on the degenerating structures. Work with a qualified physical therapist or trainer who understands spinal conditions.
Sleep position and pillow. A pillow that holds your neck in neutral alignment, supporting the natural curve without pushing the head forward or letting it drop, protects the degenerating discs and joints during the many hours you spend in bed. Back and side sleeping with proper support are kinder than stomach sleeping.
Hydration. The discs are roughly 80% water, and chronic dehydration accelerates the disc height loss that drives the whole degenerative cascade. In the Florida heat this matters even more. Aim for at least half your body weight in ounces of water daily.
Anti-inflammatory eating. Whether a degenerating segment hurts depends heavily on inflammation, and chronic systemic inflammation makes everything worse. Minimizing processed foods, refined sugars, and seed oils while emphasizing whole foods, healthy fats, omega-3-rich fish, and adequate protein supports joint and tissue health.
Smoking cessation. If you smoke, this is one of the most important things you can do for your neck. Smoking is a well-documented accelerator of disc degeneration because it impairs the already-limited blood supply that nourishes the discs.
Manage stress. Chronic stress raises muscle tension throughout the neck, increasing load on degenerating segments and lowering the threshold for painful flare-ups and guarding. Stress management is a genuine part of managing spondylosis.
If you found this guide useful, you may also want to read our blog on pinched nerve in the neck (cervical radiculopathy), which explores what happens when spondylotic changes begin to irritate a cervical nerve root and produce arm symptoms.
Serving Sarasota and the Surrounding Communities
Lavender Family Chiropractic is located in Sarasota, Florida, at 5899 Whitfield Avenue, Suite 107, at the corner of University and Whitfield. From this central location, we serve patients throughout the region, including Bradenton, Lakewood Ranch, Palmetto, Parrish, Venice, Osprey, Nokomis, Ellenton, Ruskin, Myakka City, North Port, and the greater Tampa Bay area. Patients also travel from St. Pete, Riverview, and Manatee County to receive specialized upper cervical care here.
Cervical spondylosis is the kind of diagnosis that can make people feel resigned, as though their neck is simply wearing out and there is nothing to be done. We see it differently. The degeneration may be permanent, but how your neck is loaded, how aligned it is, and how much it hurts are all things that can change. If you want a thorough, honest evaluation of where upper cervical care fits into managing your spondylosis and protecting your neck going forward, we would be glad to help.
Top 15 FAQs About Cervical Spondylosis and Upper Cervical Chiropractic Care
1. What exactly is cervical spondylosis? It is the medical term for age-related degeneration of the cervical spine, affecting the discs, facet joints, ligaments, and vertebrae. It is often called neck arthritis, cervical osteoarthritis, or degenerative disc disease of the neck, and it is a normal part of aging rather than a discrete disease.
2. Does spondylosis on my X-ray mean that is what is causing my pain? Not necessarily. Degenerative changes are extremely common and are found in many people with no symptoms at all, so imaging findings correlate poorly with pain. Your degeneration is real, but other factors, loading, alignment, muscle function, and inflammation, largely determine whether it hurts.
3. How common is it? Very. Spondylotic changes are present in roughly 25% of people under 40, 50% over 40, and up to 85% of older adults, and most of those people are asymptomatic. If you have it, you are in the large majority of people your age.
4. Can chiropractic reverse my spondylosis? No, and we will never claim it can. Degeneration that has already occurred does not reverse. What can change is how your neck is loaded and aligned from here forward, which can reduce pain and stiffness, ease muscle guarding, and slow the rate of further wear.
5. Why would adjusting the top of my neck help degeneration in the lower neck? Because the atlas and axis set the alignment for the entire cervical spine. When they are misaligned, the lower segments are loaded asymmetrically, which accelerates degeneration on the overworked side. Correcting the upper cervical foundation reduces that uneven loading going forward.
6. Is upper cervical chiropractic safe for a degenerated, arthritic neck? Yes, this is one of its advantages. The Knee Chest Upper Cervical technique is gentle and precise, with no twisting, popping, or rotational force, which makes it well suited to a spine with bone spurs and narrowed spaces, where aggressive manipulation could be inadvisable. We always examine thoroughly first.
7. What is the difference between spondylosis, a pinched nerve, and myelopathy? Spondylosis is the broad degenerative process. When it irritates a nerve root and causes arm symptoms, that is cervical radiculopathy (a pinched nerve). When it compresses the spinal cord itself, that is cervical myelopathy, the most serious form, which requires careful medical evaluation. Many people have axial neck pain from spondylosis without either nerve or cord involvement.
8. When should I be worried that it is something more serious? Seek medical evaluation if you notice changes in hand coordination or fine motor skills, balance or gait problems, or progressive weakness or numbness. These can indicate myelopathy. We screen carefully for these signs and will direct you to appropriate care if needed.
9. Will I need surgery? Most people with cervical spondylosis do not. Surgery is generally reserved for myelopathy or for radiculopathy that is progressive or has failed conservative care. Axial neck pain from spondylosis is almost always managed conservatively.
10. Does posture really affect how fast my neck degenerates? Yes, significantly. Sustained forward head posture from devices dramatically increases the load on the lower cervical discs and joints, accelerating degeneration. Addressing posture and the alignment that drives it is one of the most impactful things you can do.
11. Can a past car accident have contributed to my spondylosis? Yes. Whiplash and other neck trauma can initiate or accelerate degeneration at the injured segments, sometimes showing up as spondylosis years later. Trauma is a well-recognized contributor to earlier or more pronounced cervical degeneration.
12. Why is my degeneration worse on one side or at one level? Because degeneration follows load, and load is rarely symmetric. Asymmetric loading, often driven by upper cervical misalignment and postural compensation, concentrates wear on particular sides and levels, which is why C5/C6 is so commonly the most affected level.
13. Can stress make my spondylosis pain worse? Yes. Chronic stress raises muscle tension throughout the neck, increasing load on degenerating segments and lowering the threshold for painful flare-ups. Stress management is a genuine part of managing the condition.
14. How will I know if upper cervical care is right for me? The only way to know for certain is a thorough evaluation. Our examination, including 3D imaging and functional scans, will show whether an upper cervical misalignment is contributing to your loading pattern, and we will give you an honest assessment of what upper cervical care can and cannot do for your specific situation.
15. How do I get started? Call our Sarasota office at (941) 243-3729 or book your consultation online. We will review your history, perform a thorough examination, screen for any red flags including myelopathy, and give you a straight answer about how upper cervical care fits into managing your spondylosis.
Take the Next Step Toward Natural Neck Pain Relief
Cervical spondylosis is not a sentence, and it is not a sign that you have done something wrong. It is one of the most common features of an aging spine, found in most people your age, and the degeneration on your imaging is only one piece of why your neck feels the way it does. The pieces that matter most for how you feel, how your neck is loaded, how it is aligned, how the supporting muscles function, and how you care for it day to day, are largely within your power to influence. The people who do best with spondylosis are the ones who stop fixating on the unchangeable picture on the scan and start addressing the modifiable factors that actually drive their pain.
If you are in Sarasota, Bradenton, Lakewood Ranch, or anywhere in the surrounding region and you have been told you have neck arthritis, degeneration, or cervical spondylosis, Dr. Rusty Lavender and Dr. Jacob Temple at Lavender Family Chiropractic are here to give you an honest evaluation of where upper cervical care fits into managing your symptoms and protecting your neck for the years ahead, natural neck pain treatment focused on the causes you can actually change.
📞 Call (941) 243-3729 today to schedule your complimentary consultation 📅 Book online here 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
Related Articles
Related Posts
Popular Posts