By Dr. Rusty Lavender
Pinched Nerve in the neck: You know the feeling. A sharp, burning pain that starts in your neck and runs down into your shoulder, your arm, sometimes all the way to your fingertips. Maybe it wakes you up at night because you can’t find a position that doesn’t make it worse. Maybe you’ve noticed your grip feels weaker, you’ve dropped a coffee mug or two, or the numbness and tingling in your hand has started to interfere with typing, driving, or holding your phone. You may have already been to your primary care doctor, gotten an MRI, been told it’s a “pinched nerve,” and walked out with a prescription for muscle relaxers, anti-inflammatories, or a referral for steroid injections — and you are still in pain.
At Lavender Family Chiropractic in Sarasota, Florida, we see patients with cervical radiculopathy — the medical term for a pinched nerve in the neck — every single week. Some come in early, hoping to avoid surgery. Others come in years after their original diagnosis, having tried medications, injections, physical therapy, and sometimes failed surgeries, and they are looking for an answer nobody has been able to give them. What most of them have not been told is that the upper cervical spine — the atlas and axis at the very top of the neck — plays a far larger role in cervical nerve root irritation than the standard medical evaluation accounts for, and that addressing the upper cervical component can dramatically change the trajectory of recovery.
This guide is for anyone in Sarasota, Bradenton, Lakewood Ranch, or the surrounding areas who has been told they have a pinched nerve, a herniated disc, cervical spondylosis, or cervical radiculopathy — and who is looking for a deeper understanding of what is actually happening, why some treatments work and others don’t, and how the precise, gentle Knee Chest Upper Cervical technique used by Dr. Rusty Lavender and Dr. Jacob Temple may be the missing piece in your recovery.
What is a Pinched nerve in the neck (Cervical Radiculopathy)?
Cervical radiculopathy is the clinical name for what most people call a “pinched nerve in the neck.” It describes a condition in which a nerve root exiting the cervical spine becomes compressed, irritated, or inflamed — producing pain, numbness, tingling, weakness, or sensory changes that radiate from the neck into the shoulder, arm, hand, and sometimes the fingers.
The cervical spine has seven vertebrae (C1 through C7) and eight pairs of cervical nerve roots that exit between them. Each nerve root supplies a specific area of the upper body — a region of skin called a dermatome and a group of muscles called a myotome. When a particular nerve root is irritated, the symptoms follow a recognizable pattern. A C6 radiculopathy typically produces pain and numbness along the thumb side of the forearm into the thumb and index finger, with weakness in the biceps and wrist extensors. A C7 radiculopathy — the most common type — sends symptoms into the middle finger and produces weakness in the triceps and finger extensors. A C8 radiculopathy affects the pinky side of the hand and the small muscles of the fingers.
The compression itself comes from one of several sources. In younger patients, it is most often a herniated or bulging cervical disc — the soft cushion between two vertebrae has pushed outward into the space where the nerve root travels. In older patients, it is more often cervical spondylosis — age-related degenerative changes in the discs, vertebrae, and facet joints that gradually narrow the neural foramen (the bony opening where the nerve exits). Other causes include bone spurs, thickened ligaments, instability, tumors (rare), or trauma from whiplash and other cervical injuries.
The numbers tell the scope of the problem. The most cited epidemiological study, conducted in Rochester, Minnesota, reported an annual age-adjusted incidence of 83.2 cases per 100,000 population, with rates of 107.3 per 100,000 for men and 63.5 per 100,000 for women, and the highest incidence occurring in the 50–54 age group. A 2020 systematic review published in Musculoskeletal Care refined those estimates, reporting incidence between 0.832 and 1.79 per 1,000 person-years and prevalence values ranging from 1.21 to 5.8 per 1,000 in adults. Translated to a city the size of Sarasota and its surrounding communities, that means thousands of people in our region are dealing with cervical radiculopathy at any given moment — and many of them have been told there is little to be done short of medication or surgery.
The classic presentation includes neck pain that radiates down the arm, sharp or burning quality to the discomfort, symptoms that worsen with certain neck positions (especially looking up or rotating the head toward the painful side), numbness and tingling in a specific dermatomal pattern, and sometimes objective muscle weakness that the patient may not have noticed until tested. Reflexes in the affected arm may be diminished. The pain is often worse at night, partly because nighttime positions place the neck in sustained postures that further compress the irritated nerve root.
Conventional treatment typically progresses through a predictable sequence. Nonsteroidal anti-inflammatory drugs and muscle relaxers come first. Physical therapy is often added. If symptoms persist, cervical epidural steroid injections are commonly offered. If those fail, surgery — most often anterior cervical discectomy and fusion (ACDF) or cervical disc replacement — becomes the next step. According to the Rochester epidemiological data, 26% of cervical radiculopathy patients eventually undergo surgery, and 31.7% experience a recurrence of symptoms even after treatment.
What is missing from this conventional sequence is any meaningful evaluation of the upper cervical spine and how its alignment may be driving — or perpetuating — the symptoms at the lower cervical levels where the nerve compression is occurring. That gap is where upper cervical chiropractic care becomes essential.
The Upper Cervical Connection: Why Your Atlas and Axis Matter for a Lower Cervical Nerve Problem
It seems intuitive, at first glance, that a pinched nerve at C6-C7 or C5-C6 should be addressed at C6-C7 or C5-C6. The compression is there. The disc bulge is there. The bone spur is there. Why would the top of the neck matter for a problem at the bottom?
The answer lies in how the cervical spine functions as a single, integrated unit, and how the alignment of the atlas (C1) and axis (C2) determines the mechanical environment for every vertebra below them.
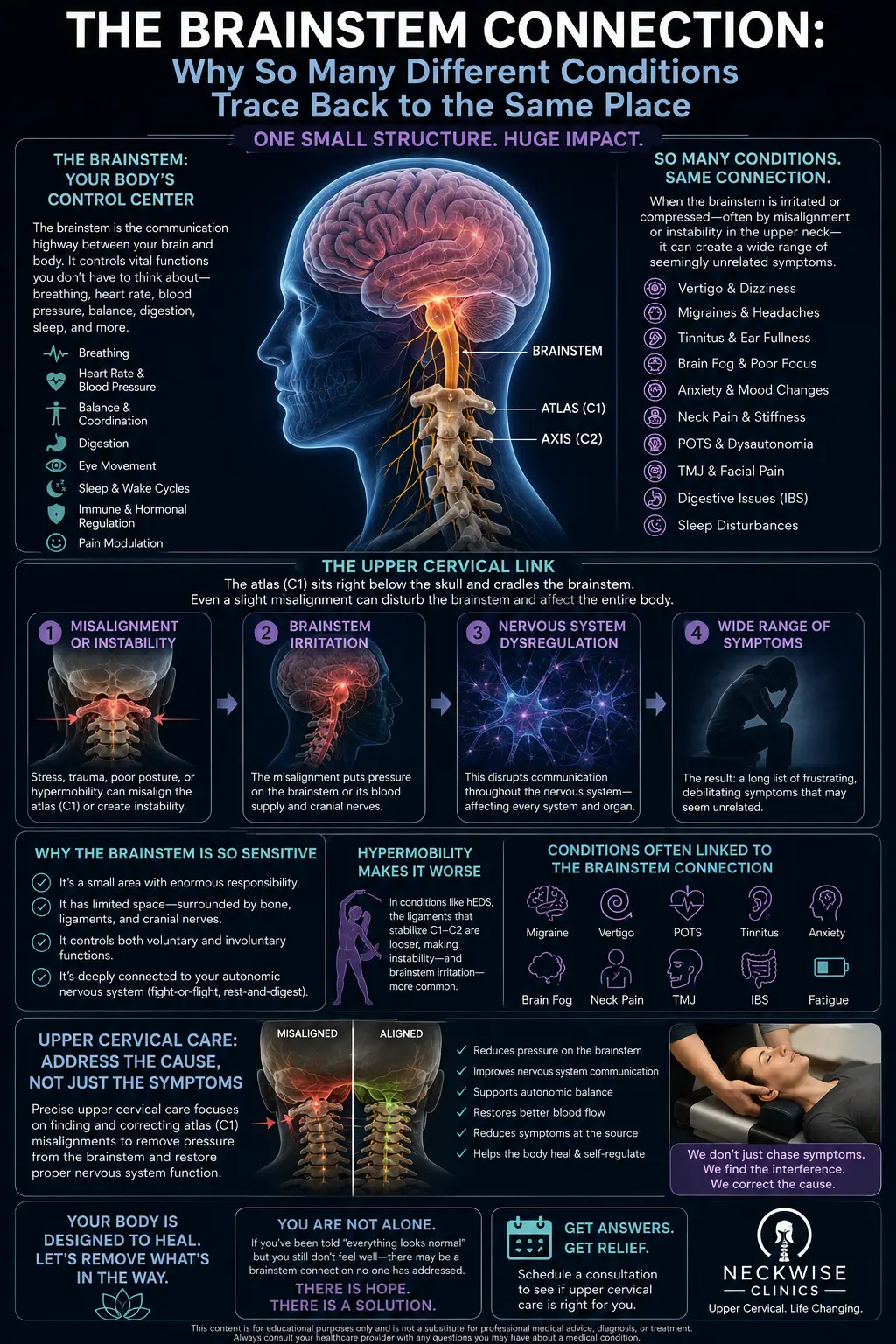
The atlas and axis form the craniocervical junction — the most mobile region of the entire spine, and the region that sets the baseline alignment for the rest of the cervical column. When the atlas is misaligned, the head must compensate to keep the eyes level and the inner ear oriented properly. The body accomplishes this by rotating, side-bending, and shifting the vertebrae below to produce a series of compensations that allow the head to remain in approximate horizontal alignment. These compensations propagate downward through C3, C4, C5, C6, and C7 — the very vertebrae where most cervical radiculopathy occurs.
In other words, a chronic upper cervical misalignment forces the lower cervical spine into asymmetric positions that it was never designed to hold long-term. The discs are loaded unevenly. The facet joints wear at different rates on the left versus the right. The neural foramina — those bony openings through which the nerve roots exit — narrow asymmetrically. Over years and decades, this is precisely how spondylosis, disc degeneration, and foraminal stenosis develop preferentially on one side. And when an acute event finally tips the balance — a sudden movement, a poor night’s sleep, a whiplash injury, a heavy lift — the nerve root on the asymmetrically narrowed side becomes the one that fires up.
There is a second mechanism that is just as important. The upper cervical spine houses the brainstem and the upper portion of the spinal cord, which means it is the gateway through which all motor commands and all sensory information must pass between the brain and the rest of the body. When the upper cervical alignment is compromised, the neurological environment in which the entire cervical nervous system operates is also compromised. Pain processing is heightened, autonomic regulation is destabilized, muscle tone is dysregulated, and the body’s ability to self-correct an irritated nerve root is reduced.
This is why patients with cervical radiculopathy who only have their lower cervical spine treated — through injections, physical therapy, or even surgery — often improve temporarily and then relapse. The driver of the asymmetric loading was never addressed. The atlas and axis are still positioned in a way that forces the lower cervical spine into the same pattern that produced the radiculopathy in the first place. If you are also dealing with daily neck pain on top of the radicular symptoms, this same upper cervical pattern is almost certainly involved.
Why Upper Cervical Care Matters for Cervical Radiculopathy
At Lavender Family Chiropractic in Sarasota, we approach cervical radiculopathy by addressing both the local problem and the upstream driver. Through the Knee Chest Upper Cervical technique, we correct atlas and axis misalignment with a precise, gentle, sub-millimeter adjustment that requires no twisting, no cracking, and no forceful manipulation of the neck. This is critical for radiculopathy patients, because aggressive manipulation of the lower cervical spine in the presence of disc pathology can be uncomfortable at best and contraindicated at worst.
For radiculopathy patients, restoring upper cervical alignment matters for several reasons. First, it reduces the asymmetric loading that has been silently driving disc and facet degeneration in the lower cervical spine for years. Once the head sits more squarely over the cervical column, the discs and joints below can begin to decompress on the side that has been chronically overloaded. Second, it normalizes the neurological environment in which the irritated nerve root is trying to heal. Pain processing centers in the brainstem and upper spinal cord function more efficiently when upper cervical input is symmetric and proprioceptively accurate. Third, it allows the deep stabilizing muscles of the neck — the multifidi, the longus colli, the rotatores — to fire properly again, which restores active stability to the cervical spine and reduces the protective muscle guarding that often perpetuates radicular symptoms.
A 2016 systematic review published in Chiropractic & Manual Therapies by Thoomes evaluated the literature on manual therapy for cervical radiculopathy and concluded that there is evidence supporting cervical manipulation and mobilization as effective interventions for pain and range of motion in cervical radiculopathy patients, particularly when combined with motor control exercises. The review noted that patients with radiculopathy due to confirmed cervical disc herniation can experience substantial improvement in both pain and activity limitations within the first three months of conservative manual therapy.
A 2021 systematic review in PMC analyzed multiple studies of manual therapy for cervical radiculopathy and reached a similar conclusion: manual therapy was effective in treating symptoms related to cervical radiculopathy in all included studies, regardless of the specific technique applied — supporting reductions in chronic cervical pain and decreases in cervical disability index scores in the short term.
What separates upper cervical chiropractic care from general manual therapy is the precision of the diagnostic process and the specificity of the correction. We are not adjusting the symptomatic level — we are adjusting the structural foundation that is forcing the symptomatic level to behave the way it does. This is fundamentally a different model of care, and it explains why patients who have failed conventional treatment often respond to upper cervical care.
What Care Looks Like at Lavender Family Chiropractic
If you come to our Sarasota office for evaluation of a pinched nerve or cervical radiculopathy, here is what to expect.
Your first visit begins with a thorough consultation. Dr. Lavender or Dr. Temple will sit down with you and review your full history — when symptoms began, what triggered them, what makes them better or worse, what treatments you have tried, what imaging has been done, and what conventional providers have told you. We want the complete clinical picture so we can determine whether your situation is one where upper cervical care is likely to help.
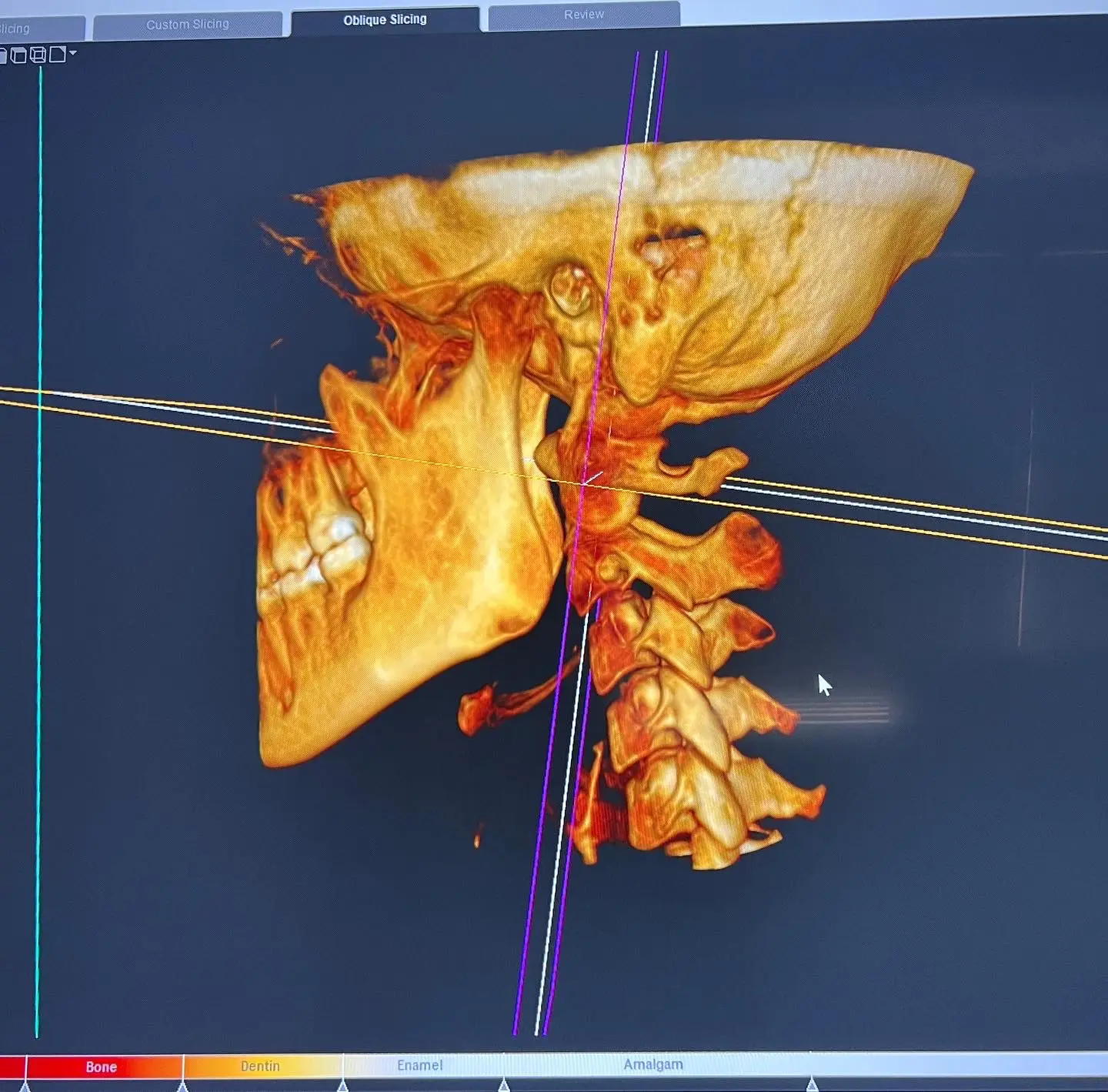
The examination includes a detailed neurological evaluation — testing reflexes, sensation, and muscle strength in each affected nerve distribution — combined with advanced 3D CBCT imaging of your cervical spine. This level of imaging is particularly important for radiculopathy patients because it allows us to visualize foraminal narrowing, disc height, facet positioning, and atlas-axis alignment in three dimensions — information that flat X-rays simply cannot provide. We also perform postural analysis, range of motion testing, and functional nervous system scans to objectively measure how your nervous system is operating before care begins.
If the examination reveals an upper cervical misalignment contributing to your radiculopathy, we will explain our recommendations openly and honestly. If your situation involves significant neurological deficit, profound muscle weakness, signs of myelopathy (spinal cord involvement), or imaging findings that genuinely require surgical evaluation, we will tell you that directly and help you coordinate appropriate medical care. We are not interested in keeping patients in care who need a different kind of help.
For patients who are appropriate candidates, care is delivered through the Knee Chest Upper Cervical technique. There is no popping, twisting, or rotational manipulation of the neck — which is particularly important for patients with disc pathology or instability. The correction is so gentle that most patients describe it as anticlimactic. The work the body does in response, however, is often dramatic.
Cervical radiculopathy is a condition that responds to consistent, repeated input over time. We offer customized treatment plans tailored to the severity and chronicity of your situation. Acute radiculopathy that responds quickly may need a shorter plan. Chronic, longstanding cases that have already led to degenerative changes typically require longer commitment but can still see meaningful improvement.
📞 Call (941) 243-3729 to schedule your complimentary consultation 📅 Book your consultation online 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield
What the Research Says About Cervical Radiculopathy and Conservative Care
The body of research on cervical radiculopathy and manual therapy has grown substantially over the past two decades, and it paints an increasingly clear picture: most cases of cervical radiculopathy can be effectively managed without surgery, and conservative care should be the first line of treatment for the vast majority of patients.
The landmark epidemiological data from Rochester, Minnesota, published in Brain in 1994 by Radhakrishnan and colleagues, remains the most cited reference for cervical radiculopathy incidence. The study followed 561 patients over 14 years and found that 90% of patients were asymptomatic or only mildly incapacitated at last follow-up, and that 26% eventually underwent surgery — meaning roughly three out of four patients improved sufficiently with conservative care alone. This is an important number for patients who are being told that surgery is the only option.
The 2020 systematic review by Mansfield and colleagues published in Musculoskeletal Care established the most current epidemiological estimates and confirmed that cervical spine radiculopathy has significant negative impacts on a person’s mental health, physical functioning, and social participation — establishing the condition as a legitimate driver of disability that warrants targeted, effective treatment.
A 2016 systematic review by Thoomes in Chiropractic & Manual Therapies synthesized the evidence on manual therapy for cervical radiculopathy and found that cervical manipulation and mobilization, particularly when combined with motor control exercises, are effective interventions for cervical radiculopathy in the short term. The review explicitly noted that patients with confirmed cervical disc herniation showed substantial improvement in pain and activity within three months of manual therapy.
A 2016 systematic review and meta-analysis published in Clinical Rehabilitation by Zhu and colleagues evaluated cervical spine manipulation for cervical radiculopathy and concluded that cervical manipulation can reduce pain and improve function in patients with cervical radiculopathy, supporting its use as a first-line conservative treatment option.
Most recently, a 2021 systematic review in PMC analyzing manual therapy for cervical radiculopathy concluded that manual therapy was effective at reducing chronic cervical pain and decreasing cervical disability across all included studies, regardless of the specific manual technique applied — a finding that strongly supports conservative care as an effective first-line approach.
Taken together, this body of research establishes cervical radiculopathy as a condition that responds to skilled conservative care, that surgery is appropriate only for a minority of cases, and that manual therapy — including the precise upper cervical work we perform — has a meaningful role to play in helping patients avoid surgery and recover function.
Lifestyle Factors That Support Recovery from a Pinched Nerve
Upper cervical chiropractic care is powerful, but lasting recovery from cervical radiculopathy requires the patient to address the daily inputs that may have contributed to the problem and that may interfere with healing.
Sleep position. The single biggest contributor to morning radicular pain is poor sleep position. Sleeping on the stomach with the neck rotated for hours is among the worst possible positions for an irritated cervical nerve root. Back sleeping with a thin pillow that supports the natural curve of the neck — or side sleeping with a pillow that keeps the head neutrally aligned with the spine — protects the nerve roots during the seven to nine hours you spend in bed.
Screen ergonomics. Looking down at phones, tablets, and laptops for hours per day increases the load on the lower cervical spine dramatically and contributes directly to disc and foraminal pathology. Bring screens to eye level whenever possible.
Anti-inflammatory eating. Nerve root irritation involves inflammation, and chronic systemic inflammation makes any nerve compression worse. Minimizing processed foods, refined sugars, and seed oils while emphasizing whole foods, healthy fats, omega-3-rich fish, and adequate protein supports nerve healing. Omega-3 fatty acids and B vitamins (particularly B12) have specific roles in nerve repair.
Hydration. The intervertebral discs are roughly 80% water, and chronic dehydration accelerates disc degeneration — one of the primary structural causes of cervical radiculopathy. The Florida heat makes this issue particularly relevant for Sarasota patients. Aim for at least half your body weight in ounces of water daily.
Smoking cessation. If you smoke, this is the single most important lifestyle change you can make. Smoking is a well-documented risk factor for cervical disc degeneration and impairs disc healing. The discs receive their nutrition through diffusion, and nicotine constricts the small blood vessels that supply the surrounding tissue.
Gentle movement. Total immobility makes radiculopathy worse, not better. Gentle, pain-free range of motion exercises, walking, and low-impact activity support circulation, reduce muscle guarding, and promote healing. Avoid heavy lifting, overhead pressing, and aggressive neck stretching until cleared.
Avoid aggressive neck manipulation. During an active radiculopathy episode, aggressive twisting or rotational manipulation of the neck — including some traditional chiropractic adjustments — can worsen disc pathology. The Knee Chest Upper Cervical technique avoids these forces entirely, which is one of the reasons it is appropriate for radiculopathy patients.
If you found this guide useful, you may also want to read our blog on ear fullness after a car accident or whiplash, which explores how cervical trauma can produce symptoms far beyond the neck itself — including in nerve pathways that the upper cervical spine helps regulate.
Serving Sarasota and the Surrounding Communities
Lavender Family Chiropractic is located in Sarasota, Florida, at 5899 Whitfield Avenue, Suite 107 — at the corner of University and Whitfield. From this central location, we serve patients throughout the region, including Bradenton, Lakewood Ranch, Palmetto, Parrish, Venice, Osprey, Nokomis, Ellenton, Ruskin, Myakka City, North Port, and the greater Tampa Bay area. Patients also travel from St. Pete, Riverview, and Manatee County to receive specialized upper cervical care here.
Cervical radiculopathy is a condition where patients are often willing to drive significant distances to find a provider who can offer something different from the medications-then-injections-then-surgery sequence. If you have been on that conveyor belt and are looking for a different approach — or if you are trying to prevent ever getting on it in the first place — we encourage you to reach out.
Top 15 FAQs About Pinched Nerves, Cervical Radiculopathy, and Upper Cervical Chiropractic Care
1. Is a pinched nerve the same thing as cervical radiculopathy? Functionally, yes. “Pinched nerve” is the common term and “cervical radiculopathy” is the medical term for the same condition — compression or irritation of a nerve root as it exits the cervical spine, producing pain, numbness, tingling, or weakness in the arm and hand.
2. Will my pinched nerve heal on its own? Many cases do improve with time. Research suggests roughly 75% of cervical radiculopathy patients improve with conservative care without ever needing surgery. However, “improving on its own” does not address the underlying biomechanical drivers, which is why recurrence is common — affecting nearly a third of patients in long-term studies.
3. How do I know if I need surgery? Surgery is generally reserved for patients with progressive neurological deficit, profound muscle weakness, signs of spinal cord involvement (myelopathy), intractable pain that has not responded to conservative care over several months, or specific imaging findings that warrant surgical decompression. Most patients do not meet these criteria.
4. Is upper cervical chiropractic safe for someone with a herniated disc? The Knee Chest Upper Cervical technique is exceptionally gentle and does not apply rotational or aggressive forces to the cervical spine. This makes it appropriate for many patients with disc pathology, where more aggressive manipulation would be contraindicated. We perform a thorough examination before recommending care.
5. What is the difference between upper cervical care and a regular chiropractic adjustment? A regular chiropractic adjustment typically involves manipulation of the symptomatic vertebral level using rotational or high-velocity techniques. Upper cervical care focuses exclusively on the atlas and axis at the top of the neck and uses sub-millimeter precision with a gentle, controlled correction — no twisting, popping, or cracking.
6. Why would adjusting the top of my neck help a problem in the lower neck? The atlas and axis set the alignment for the entire cervical spine. When they are misaligned, the lower cervical vertebrae compensate with asymmetric loading patterns that drive disc degeneration, foraminal narrowing, and eventually nerve root irritation. Correcting the upper cervical foundation removes the driver of these compensations.
7. How long does upper cervical care take to work for radiculopathy? Some patients notice meaningful improvement within the first few weeks. Others, particularly those with chronic, longstanding cases or significant degenerative changes, require months of consistent care. Your examination findings will give us a realistic timeline.
8. Should I avoid certain activities during recovery? Yes — avoid heavy lifting, overhead pressing, prolonged poor postures, aggressive neck stretching, and any movement that reproduces sharp radicular pain. Gentle movement, walking, and pain-free range of motion are generally beneficial.
9. Will an MRI tell me everything I need to know? MRI is essential for identifying disc pathology, foraminal narrowing, and ruling out serious causes — but it does not capture how the cervical spine moves or how the upper cervical alignment is functioning. A complete evaluation requires both static imaging and functional/postural assessment.
10. Can stress make radiculopathy worse? Yes. Chronic stress increases sympathetic nervous system activity, raises muscle tone, lowers pain thresholds, and increases systemic inflammation — all of which make any nerve root irritation worse. Stress management is an underrated part of recovery.
11. Can radiculopathy come back after it goes away? Unfortunately yes — the Rochester epidemiological data showed recurrence in 31.7% of patients. Recurrence usually points to an unresolved underlying driver, which is exactly why addressing the upper cervical foundation matters: it reduces the asymmetric loading pattern that produced the radiculopathy in the first place.
12. Are nerve pain medications like gabapentin a long-term solution? Medications like gabapentin and pregabalin can reduce nerve pain signals, but they do not address the structural cause of the compression. They are appropriate as part of a broader treatment strategy, but they are not a long-term solution by themselves and they come with side effects, including significant drowsiness and cognitive effects.
13. Can a car accident cause cervical radiculopathy? Yes. Whiplash injuries from motor vehicle accidents are a well-documented cause of cervical disc herniation, ligamentous injury, and subsequent radiculopathy — sometimes appearing immediately and sometimes developing months or years after the initial crash. Our car accident chiropractic care addresses this specifically.
14. How will I know if upper cervical care is right for me? The only way to know for certain is to come in for an evaluation. Our examination will identify whether you have an upper cervical misalignment contributing to your radiculopathy. If you do, we will explain exactly what we recommend. If your situation requires a different kind of care, we will tell you that honestly.
15. How do I get started? Call our Sarasota office at (941) 243-3729 or book your consultation online. We will sit down with you, perform a thorough examination, and give you a straight answer about whether upper cervical care is a good fit for your specific situation.
Take the Next Step Toward Relief
A pinched nerve in the neck is not just an inconvenience. It is a structural and neurological problem that, untreated, tends to either smolder for years with intermittent flare-ups or progress to the point where more aggressive interventions become necessary. The patients who do best are the ones who address every layer of the condition — including the upper cervical foundation that most providers never evaluate.
If you are in Sarasota, Bradenton, Lakewood Ranch, or anywhere in the surrounding region and you are dealing with neck pain, arm pain, numbness, tingling, or weakness — whether it started last week or last year — Dr. Rusty Lavender and Dr. Jacob Temple at Lavender Family Chiropractic are here to help you understand the upper cervical piece of your healing puzzle and chart a path forward that does not start with “let’s try one more medication.”
📞 Call (941) 243-3729 today to schedule your complimentary consultation 📅 Book online here 📍 5899 Whitfield Avenue, Suite 107, Sarasota, FL 34243 — at the corner of University and Whitfield